
Abstract
A 7-year-old female German Shepherd Dog was presented with multiple petechiae and ecchymoses along the ventral abdomen, flank, and on the vaginal mucosa. The clinical diagnosis was severe hemoperitoneum and presumed disseminated intravascular coagulopathy. Postmortem examination revealed a 22 cm × 15 cm × 6 cm, firm, and convoluted peritoneal mass along with hemoperitoneum, and multifocal, ill-defined, 0.5–1.5 cm in diameter, white to tan nodules in the pulmonary parenchyma. Histologically, the peritoneal mass was composed of large anaplastic cells consistent with malignant mesothelioma interspersed in abundant fibrous connective tissue. Metastasis of the neoplastic cells occurred to the brain, adrenal glands, lymph nodes, and lungs. On immunohistochemical evaluation, neoplastic cells coexpressed cytokeratin and vimentin, and were negative for cluster of differentiation (CD)18. Electron microscopy revealed numerous surface microvilli around the entire circumference of the neoplastic cells, as well as tight junctions, and desmosome-like structures. Based on test findings, a disseminated sclerosing peritoneal mesothelioma was diagnosed.
Mesotheliomas are neoplasms that arise from mesothelial cells lining the coelomic cavities. 11 The affected domestic animals include young cattle, adult dogs, horses, and cats. 2 In dogs, in particular, mesotheliomas often arise in thoracic and abdominal cavities as well as within the tunica vaginalis of the scrotum.6,17,24 In dogs, mesotheliomas are mostly seen in dogs varying from 4–13 years in age, with a mean age of 7.8 years. 11 Although there are no reports of breed predisposition in mesothelioma, a previous study suggests that German Shepherd Dogs are overrepresented. 21 The current report describes histopathological, immunohistochemical, and ultrastructural features of sclerosing malignant mesothelioma in an adult female German Shepherd Dog.
A 7-year-old, intact, female German Shepherd Dog presented as an emergency referral at the Veterinary Teaching Hospital and Clinic, Louisiana State University (Baton Rouge, LA) with numerous cutaneous petechiae, ecchymoses, and prolonged bleeding time from venipuncture sites. On physical examination, the dog was bright, responsive, and had multiple petechial and ecchymotic hemorrhages along the ventral abdomen, flank, and on the vaginal mucosa. Pulmonary auscultation revealed harsh lung sounds with possible crackles. A complete blood cell count (CBC), serum biochemical panel, and abdominal ultrasonography were performed. Serum toxicological analysis for warfarin, bromadiolone, brodifacoum pival, diphacinone, chlorophacinone, and difethialone was also performed. Briefly, serum samples were extracted using matrix solid-phase dispersion technique, and were subsequently analyzed by high-performance liquid chromatography. Detection of the compounds was accomplished using both florescence and ultraviolet absorption. The animal was administered multiple units of fresh frozen plasma and fluid therapy; however, due to the poor prognosis, the owner elected euthanasia. Necropsy examination was performed as described previously. 16
For histopathologic examination, various tissues including samples of the peritoneal mass, brain, lung, adrenal glands, and lymph node were fixed in 10% neutral buffered formalin, routinely processed, paraffin-embedded, sectioned at 5 µm, and stained with hematoxylin and eosin. Immuno- histochemical staining of histological sections was performed for cluster of differentiation (CD)18 (mouse anti-canine monoclonal antibody [mAb], clone CA16.3C10), vimentin (mouse anti-vimentin mAb, clone V9), and cytokeratin (mouse anti-human mAb, clone AE1/AE3) using the streptavidin–biotin complex peroxidase method as described by the manufacturer. a The positive control tissues were lymph node (for CD18), spleen (CD18), lung (vimentin), and haired skin (cytokeratin) from a healthy dog. The negative controls consisted of the same tissue types but were not treated with the primary mAb during the immunohistochemistry assay. The brain sections were fixed in 10% neutral buffered formalin prior to processing for electron microscopy. For transmission electron microscopic examination, 1-mm3 pieces of the affected brain tissue were fixed in 3% glutaraldehyde, post-fixed in 1% osmium tetroxide, dehydrated in ethanol, and embedded in liquid epoxy resin. b The ultrathin sections (70–90 nm) were stained with lead citrate and uranyl acetate, and examined with an electron microscope. c
The CBC results revealed a mild normocytic, normochromic, highly regenerative anemia (red blood cell count, 4.79 × 106/µl, reference [ref.] interval: 5.4–8.4 × 106/µl; hematocrit, 32.8.%, ref. interval: 35–54%; absolute reticulocyte count of 326.6 × 103/µl, ref. interval: <80,000/µl; and moderate polychromasia), moderate thrombocytopenia (platelets, 53 × 103/µl with few clumps, ref. interval: 220–600 × 103/µl), and moderate leukocytosis (white blood cell count, 25.9 × 103/µl, ref. interval: 8–14.5 × 103/µl) characterized by moderate neutrophilia (20.8 × 103/µl, ref. interval: 3–11.5 × 103/µl) and slight eosinophilia (1.7 × 103/µl, ref. interval: 0.1–1.2 × 103/µl). The other hematological findings were within reference intervals. The blood coagulation profile revealed a prolonged prothrombin time (29 sec, ref. interval: 5–8.5 sec), and markedly elevated partial thromboplastin time (>100 sec, ref. interval: 9–14 sec). No significant findings were noted on the serum biochemical panel. Abdominal ultrasound examination revealed a severely enlarged abdomen with evidence of large amounts of echogenic free fluid in the peritoneal cavity. Serum toxicological results were negative for warfarin, bromadiolone, brodifacoum pival, diphacinone, chlorophacinone, and difethialone. A presumptive diagnosis of severe hemoabdomen with disseminated intravascular coagulopathy (DIC) was made based on the physical examination and laboratory findings.
Postmortem examination revealed approximately 1.5–2.0 l of dark red blood in the peritoneal cavity. A 22 cm × 15 cm × 6 cm firm, multilobular mass with a smooth surface and multiple ecchymotic areas extended from the mid-ventral abdominal wall and protruded into the peritoneal cavity (Fig. 1A). The mass was only localized to the body cavity wall, and adjacent viscera and organs were not involved. The cut surface was white to tan with dark red streaks dissecting the mass into lobules. The lung lobes contained multifocal to coalescing, ill-defined, 0.5–1.5 cm in diameter, white to tan nodules that extended from the pleural surface into the pulmonary parenchyma. The hilar lymph nodes were enlarged approximately 2–3 times their normal size. No other remarkable macroscopic findings were noticed. Based on findings from necropsy examination, the differential diagnoses were metastatic mammary adenocarcinoma and malignant mesothelioma.
Histologically, the peritoneal mass was a moderately cellular, infiltrative, unencapsulated neoplasm extending from the rectus abdominus muscle and dissecting between muscle fibers and adipose tissue. The neoplastic cells were loosely arranged in clusters and nests and were frequently individualized and supported by abundant coarse fibrous stroma (Fig. 1B). Morphologically, the cells were ovoid to epithelioid in shape, had distinct cell borders, and contained moderate to abundant amounts of eosinophilic finely granular to vacuolated cytoplasm (Fig. 1B). Nuclei were round to oval with variably stippled chromatin and centrally placed 1–2 nucleoli. There was marked anisocytosis and anisokaryosis with frequent binucleation to multinucleation. Mitoses averaged 5 per 10× high power fields of view, and the neoplastic cells occasionally showed microvillus borders. There were large areas of hemorrhages, moderate numbers of degenerate and viable neutrophils, plus scattered lymphocytes and plasma cells. Metastatic neoplastic cells were also present in the adrenal glands, subcapsular and cortical sinuses of hilar lymph node (Fig. 1C), brain (Fig. 1D), and lung and frequently occluded the blood vessels in the lungs and brain (neoplastic embolization).
Neoplastic cells stained strongly positive for cytokeratin (diffuse pattern) and vimentin (nuclear pattern; Fig. 1E, 1F), and were negative for CD18. Ultrastructurally, neoplastic cells were joined by tight junctions and desmosome-like structures, had prominent heterochromatin, rough endoplasmic reticulum, and numerous surface microvilli around the entire circumference (Fig. 2). Histomorphological, immunohistochemical, and ultrastructural features of this neoplasm were most consistent with the sclerosing variant of a malignant epithelioid mesothelioma.5,8,21
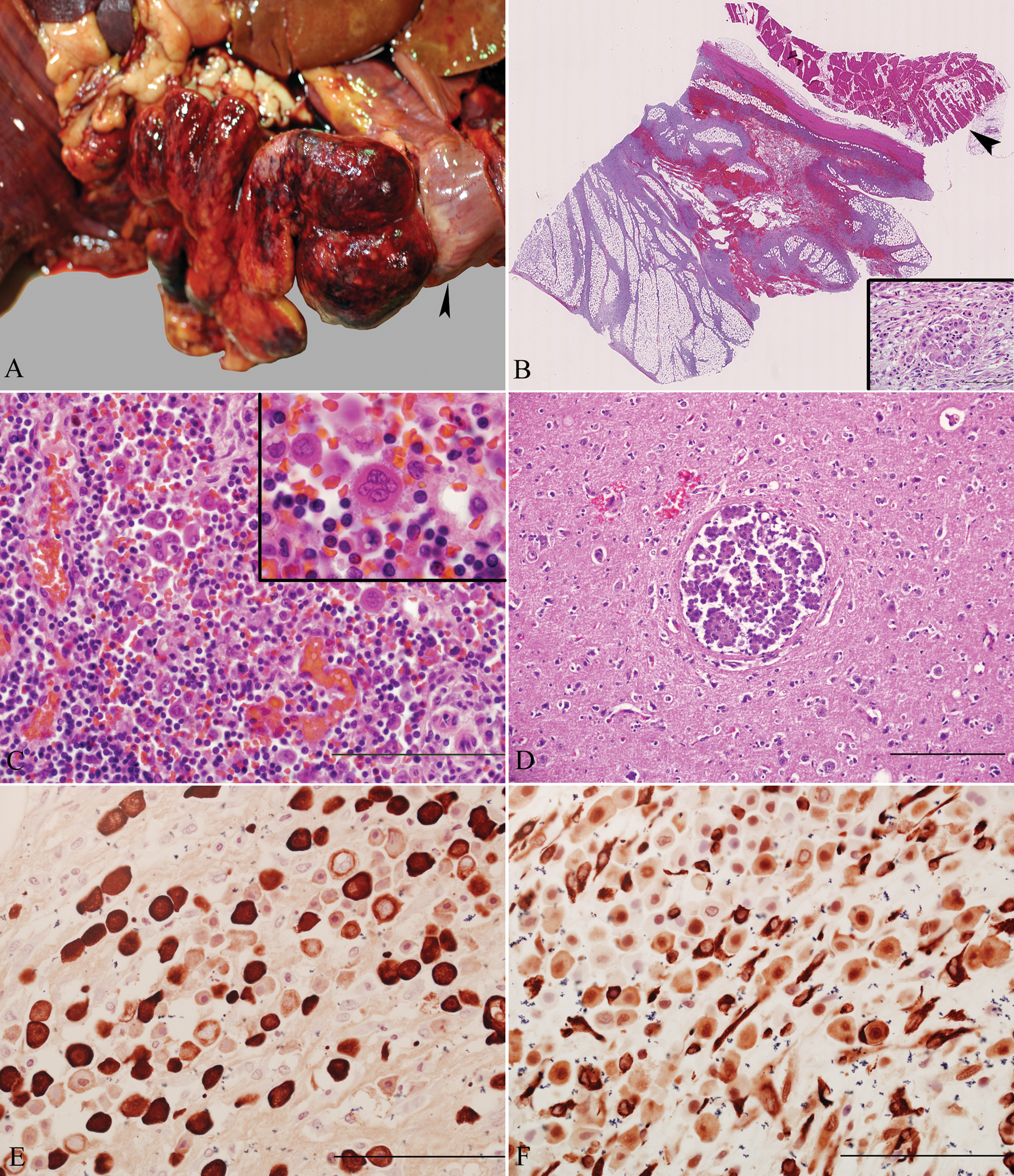
Peritoneal mass; dog.
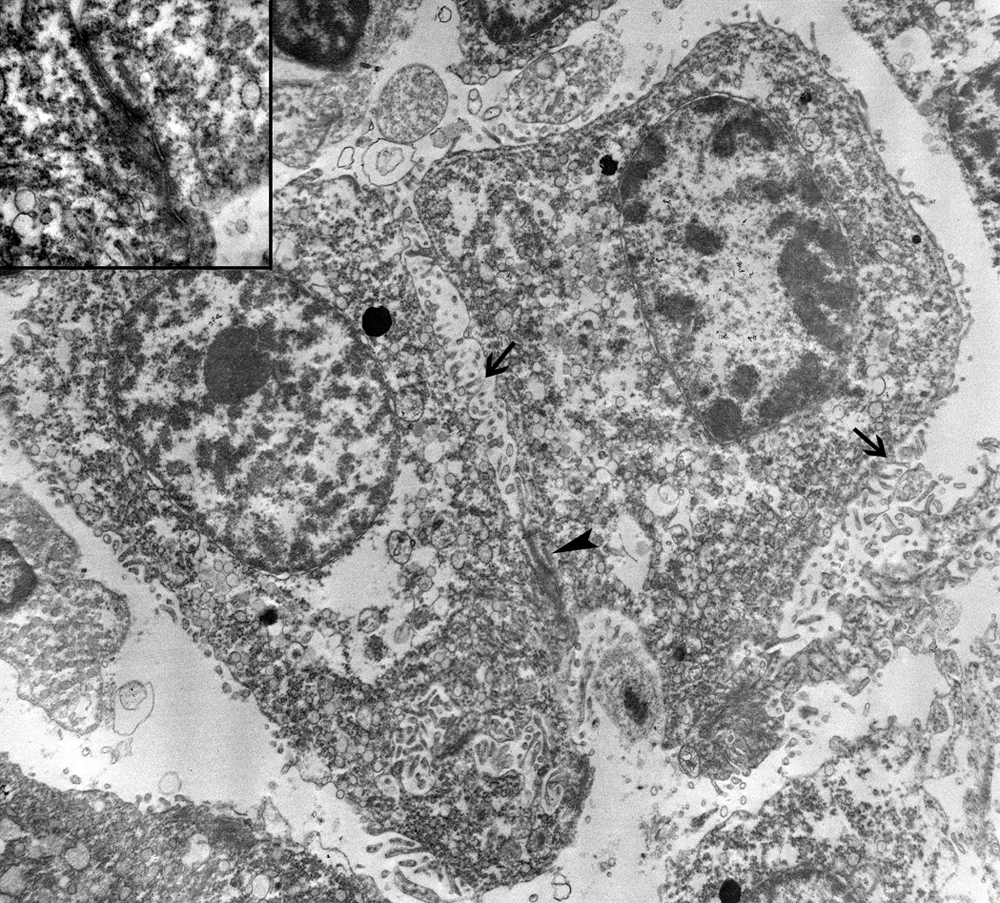
Ultrastructural view of embolized neoplastic cells in the brain demonstrates the presence of numerous slender surface microvilli (arrows), round to oval nuclei, and prominent cell junction (arrowhead). Transmission electron microscopy. 6,000× magnification. Inset: higher magnification of intercellular cell junction. 50,000× magnification.
Mesothelioma has 3 distinct histological patterns: epithelioid, fibrous (sarcomatoid), and mixed cell (biphasic). 11 According to the nomenclature presented in the Histological Classification of Tumors of the Alimentary System of Domestic Animals, the term scirrhous, sclerosing, or desmoplastic is used in the presence of excessive fibrous stroma for the epithelioid variant of malignant mesothelioma. 10 These neoplasms may show foci of chondroplasia, and osteoid or mineralized bone formation, which were absent in this case. The fibrous variant of malignant mesothelioma in some ways resembles fibrosarcoma, while the biphasic variant contains areas of carcinomatous and sarcomatoid appearance. 10 Neoplastic epithelioid and spindle cells coexpress cytokeratin and vimentin in the biphasic variant of mesothelioma. 20 In the present case, neoplastic epithelioid cells were interspersed in abundant fibrous connective tissue, and the spindle cells within the fibrous stroma did not exhibit arrangement typical of fibrosarcoma. Furthermore, only epithelioid cells coexpressed cytokeratin and vimentin. Additional subtypes reported in dogs include deciduoid peritoneal mesothelioma, 17 cardiac mesothelioma with granular cell morphology, 19 lipid-rich pleural mesothelioma, 1 and cystic peritoneal mesothelioma. 4 Grossly, mesotheliomas mostly appear as fragile, pedunculated nodules with villous projections on the serosal surface. 2 In contrast, the sclerosing mesotheliomas are large, firm, multinodular, and irregularly shaped masses with smooth surfaces.8,21 Histologically, conventional mesothelioma consists of arborizing papillary structures lined by cuboidal to polygonal cells with abundant eosinophilic cytoplasm. 11 As in the current case, sclerosing mesothelioma is constituted by thick fibrous sclerosing masses composed of large anaplastic mesothelial cells. 5 In dogs, sclerosing mesothelioma has been reported in the stomach, intestine, urinary bladder, pancreas, prostate, and omentum,5,8,21 but not in the peritoneal cavity per se. The current report further documents the presence of metastasis of neoplastic mesothelial cells in the brain, adrenal glands, lymph nodes, and lungs. While there are no previous reports of malignant mesothelioma metastasizing to brain in the veterinary literature, rare cases of brain metastases have been reported in human beings. 14
Mesothelial cells resemble epithelial cells, and it is difficult to differentiate them from adenocarcinoma, particularly when they occur in metastatic foci. In contrast with adenocarcinoma, mesothelial cells are ultrastructurally characterized by well-developed surface microvilli, which are considered to be one of the typical structural differentiations.11,21,23 Diagnosis can be supported by unique immunohistochemical features of mesotheliomas. A consistent feature of these neoplasms is the coexpression of epithelial and mesenchymal markers such as cytokeratin and vimentin which is due to a mesodermal ontogeny (precursor of both epithelial and mesenchymal cells).11,19 However, coexpression of cytokeratin and vimentin has been reported in other neoplasms as well, including, but not limited to, anaplastic carcinomas, amelanotic melanoma, renal carcinomas, and Sertoli cell tumor. 19 In the present case, neoplastic cells showed intense staining for both cytokeratin and vimentin, and there was no evidence of primary mammary masses. Histiocytic sarcoma, considered one of the differentials on the basis of frequent multinucleation, was ruled out by negative CD18 immunostaining and ultrastructural examination. Further, histological and ultrastructural features as described above supported the diagnosis of malignant sclerosing mesothelioma.
Some of the unique features of mesothelial cells are constitutive of high expression of the tumor suppressor gene p53, acquisition of epithelial or fibroblast morphology with specific inflammatory stimuli, and phagocytic potential. 3 Asbestos exposure, which has been implicated in the development of pleural mesothelioma in human beings, 13 is considered to be a risk factor in canine mesothelioma as well. 9 Mesothelioma has been experimentally induced in rats by injection of asbestos, glass fibers, aluminium oxide, and Simian virus 4015,18; however, the precise role of asbestos exposure and development of mesotheliomas in domestic animals is currently unknown. Malignant mesothelioma preferably metastasizes via lymphatic routes, even though distant metastases are rarely reported. 11 Transcoelomic implantation, usually associated with copious effusion as a result of lymphatic blockade has also been reported. 11 The presence of intravascular tumor emboli in the current case most probably contributed to the thrombocytopenia and possible DIC. The possible explanation is that tumor cells may directly activate platelets causing thrombocytopenia and shortening of the platelet survival time. Secondly, the chronic deposition of platelets and fibrin on the tumor surface and concurrent fibrinolysis may be responsible for the consumption coagulopathy. 22 However, these assumptions are merely speculative since testing for D-dimers was not done in the present case. In human beings, DIC has been reported with pericardial mesotheliomas. 12 A possible explanation is that tumors initiate DIC by expression of tissue factor, which in conjunction with factors VII–IX, can activate extrinsic and intrinsic coagulation pathways. 7 In conclusion, the current report presents a case of metastatic malignant peritoneal epithelioid sclerosing mesothelioma in a German Shepherd Dog that presented with clinical signs suggestive of DIC.
Footnotes
Acknowledgements
The authors thank Dr. Xiaochu Wu and Greg McCormick for providing assistance with electron microscopy.
a.
EnVision+ System-HRP Labeled Polymer (DAB), Dako North America Inc., Carpinteria, CA.
b.
Epon™, Hexion Specialty Chemicals, Columbus, OH.
c.
JEM-1011, JEOL Ltd., Tokyo, Japan.
The authors declared that they had no conflicts of interests in their authorship and publication of this contribution.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.