
Abstract
A 9-year-old female crossbred dog was presented to the Hospital Universitario Veterinario Rof Codina (Universidad de Santiago de Compostela, Lugo, Spain) for acute onset of severe, progressive swelling of the head, neck, and cranial trunk. Survey radiographs and ultrasonography revealed a large, heterogeneous mass in the cranial mediastinum, compressing or growing into a large blood vessel within the cranial mediastinum and displacing the heart dorsocaudally. At postmortem examination, the mass was diagnosed as a large, localized mesothelioma. Localized mesotheliomas are rare neoplasms in dogs but should be considered as a possible differential diagnosis for cranial vena cava syndrome. The anatomic distribution and clinical features of mesothelioma in the present report are similar to other cases in humans.
Mesotheliomas, which are of mesodermal origin and arise from the serosal lining of the body cavities, are rare tumors in dogs and cats. The pleura, peritoneum, and pericardium are more commonly affected, but this neoplasm can also arise in the scrotum and tunica vagina-lis. 2,6,7,19,32,33 Classical mesotheliomas occur as a diffuse nodular mass or multifocal masses covering the surfaces of the body cavity. Extensive effusions occur because of exudation from the tumor surface or from tumor-obstructed lymphatics; therefore, the most common presenting sign is dyspnea from pleural effusion or a distended abdomen from peritoneal effusion. 13 Diagnosis of mesothelioma is challenging because clinical signs are related to the exudation of fluid into cavities rather than the development of a discrete mass. Solitary mesotheliomas are rare in human medicine and have only been reported once in the veterinary literature. 1,17,23,28,35
Cranial vena cava syndrome is an uncommon but easily recognized sequel to obstruction of the cranial vena cava. Impaired blood flow through this vessel causes elevated venous hydrostatic pressure above the point of obstruction. Excessive fluid leakage from capillaries into the interstitial space overwhelms normal lymphatic mechanisms for extracellular fluid clearance. The end result is subcutaneous, pitting edema of the head, neck, and forelimbs, giving rise to the classic clinical presentation of cranial vena cava syndrome. 27 In addition to edema, jugular venous distention and engorgement of conjunctival and scleral vessels may occur. Pleural effusion is frequently part of the clinical picture and tends to be chylous in nature. 18,26,27,29 This clinical presentation should be differentiated from that associated with obstruction or compression of the caudal vena cava. Clinical signs associated with caudal vena cava syndrome include ascites, subcutaneous edema that extends along the dependent parts of the abdomen and hind limbs, and in some cases, hepatomegaly. 12
Mediastinal neoplasia is one of the most common causes of this syndrome reported in veterinary medicine. 27 Thymoma is the most common neoplasm reported in veterinary patients with cranial vena cava syndrome. 8,27 Other neoplasms have also been reported, including mediastinal lymphoma, carcinoma, and aortic body tumors. 24,27 Thrombus formation of the cranial vena cava is another recognized cause of this syndrome. 29 Infectious diseases are rare causes of cranial vena cava syndrome, and only cryptococcosis and blastomycosis have been described in the veterinary literature to date. 18,26 The purpose of the present report is to describe an unusual presentation of mesothelioma due to its massive size, focal nature, and clinical signs.
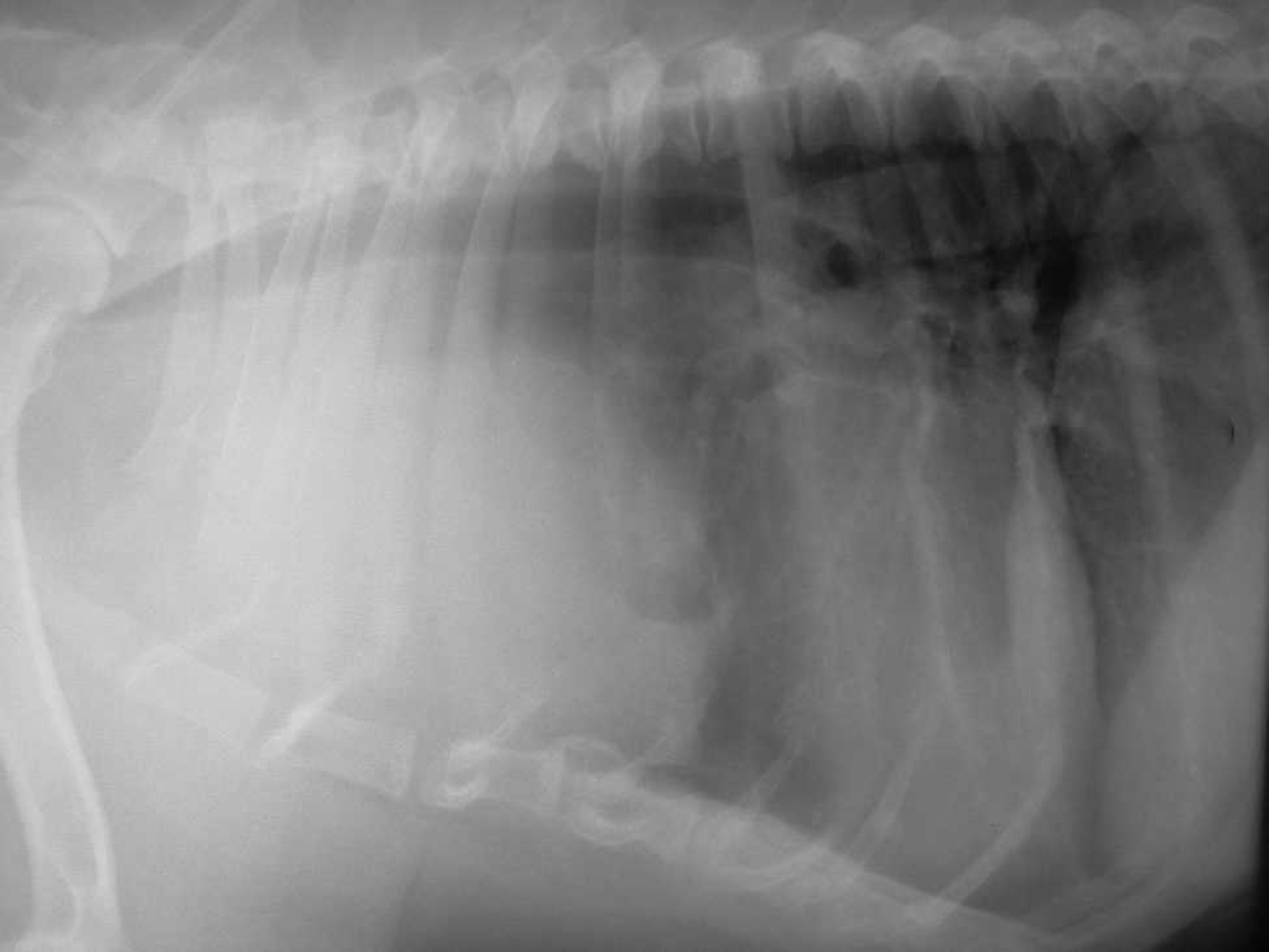
Right lateral thoracic radiograph. A well-defined cranial thoracic mass, approximately 8 cm in diameter, is present. The heart is displaced dorsocaudally by the mass.
A 9-year-old female crossbred dog weighing 33 kg was presented to the Veterinary Teaching Hospital Rof Codina (Universidad de Santiago de Compostela, Lugo, Spain) for evaluation of severe, progressive swelling of the head, neck, and cranial trunk. The owners first noted swelling of the face that appeared to spread gradually during the ensuing 7 days. Respiratory difficulty was not noted; however, the dog had become more depressed, with decreased appetite and activity. On physical examination, mild respiratory distress, cranial vena cava syndrome, and caudal displacement of the cardiac impulse were noted. The differential diagnosis included cranial vena cava obstruction due to an intraluminal mass (neoplasia or thrombus) or an extra-luminal compressive lesion. 27 A complete blood cell count revealed mild nonregenerative anemia (hematocrit = 33.8%, reference interval: 37–55%; red blood cell count = 4.9 × 106/μl, reference interval: 5.5 × 106/μl to 8.5 × 106/μl; reticulocyte count = 29.1 × 103/μl). The biochemical profile and urinalysis were unremarkable. Thoracic radiographs demonstrated a large, homogenous, soft tissue density mass in the cranial mediastinum displacing the heart dorsocaud-ally, a nonspecific pulmonary interstitial pattern, as well as incidental thoracic spondylosis (Fig. 1). Thoracic ultraso-nography revealed a mass of heterogeneous echogenicity (approximately 9 cm × 8 cm × 12 cm) compressing or growing into a large blood vessel within the cranial mediastinum. Differential diagnoses included neurogenic tumor, paraspinal tumor, ectopic thyroid or parathyroid tumor, thymoma, thymolipoma, heart-base tumor, and lymphoma. 8,24,30,37 Ultrasound-guided fine-needle aspiration cytology of the mass was inconclusive, revealing only peripheral blood cells. The owners declined a thoracic computed tomography (CT) examination. Permission was obtained to euthanize the dog and perform a necropsy. On postmortem examination, the cranial mediastinum contained a firm, tan to white, nodular, 10-cm diameter mass located cranial to heart. Thoracic effusion was not present. No gross lesions were observed in the other organs. Histologically, the tumor consisted of clusters of irregular, stratified, cuboidal mesothelial cells with arborizing growths supported by fibrous connective tissue. Individual neoplastic cells were cuboidal and had round to oval atypical nucleus, prominent nucleoli, and a small to moderate amount of eosinophilic cytoplasm (Fig. 2). Very few mitotic figures were observed. Single cells or clusters of neoplastic cells were also observed in the subcapsular sinuses of the lymph nodes, but other tissues and organs were devoid of metastases.
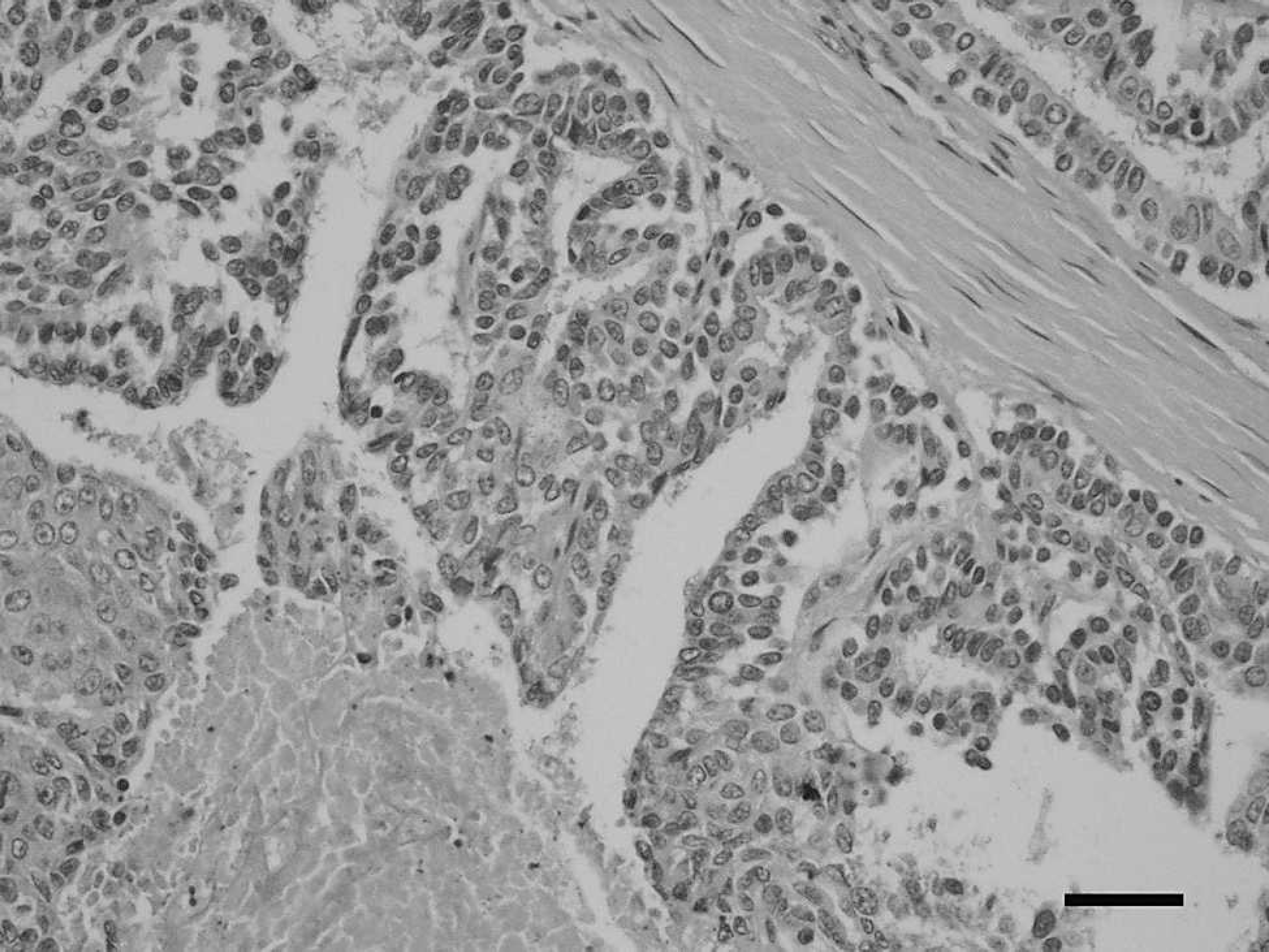
Light microscopy, mediastinal mass. Note the papillary outgrowth of the neoplastic mesothelial cells supported by fibrous connective tissue. Mesothelial cells display a high degree of pleomorphism with nuclear atypia and few mitotic figures. Hematoxylin and eosin. Bar = 50 μm.
For immunohistochemical evaluation, cytokeratin a and vimentin b antibodies were applied to replicate tissue sections. The neoplastic cells were weakly to strongly positive for both cytokeratin (Fig. 3) and vimentin (Fig. 4). Based on the histopathological and immunohistochemical findings, a diagnosis of mesothelioma was made. 31 Meso-theliomas are subclassified according to the histologic growth pattern into epithelial, fibrous (sarcomatous), or biphasic types. 3,10,15,34 The histological characteristics of the tumor in the current study were consistent with an epithelial mesothelioma that has been reported previously and is by far the most common form of mesothelioma in small animals. 3,15,16,31,36
Mesothelioma is a rare neoplasm of dogs and cats affecting the cells lining the coelomic cavities of the body. In dogs, primary mesotheliomas arise in the thoracic cavity, abdominal cavity, pericardial sac, and tunica vaginalis of the scrotum. 6,10,13,19,32 Mesothelioma develops in dogs of various ages, usually ranging from 4 to 13 years, with a mean of 7.8 years. 16 However, mesothelioma also has been reported in puppies as young as 7 weeks. 20,22 Although there is no proven breed predisposition, 2 previous studies reported a preponderance of mesotheliomas in German Shepherd Dogs. 10,25 In humans, exposure to asbestos has been closely implicated in the development of pleural mesotheliomas. 3,5,34 Although asbestos exposure is also considered to be a risk factor in dogs, 12–14,17 there was no known exposure to this compound in the dog of the present study.
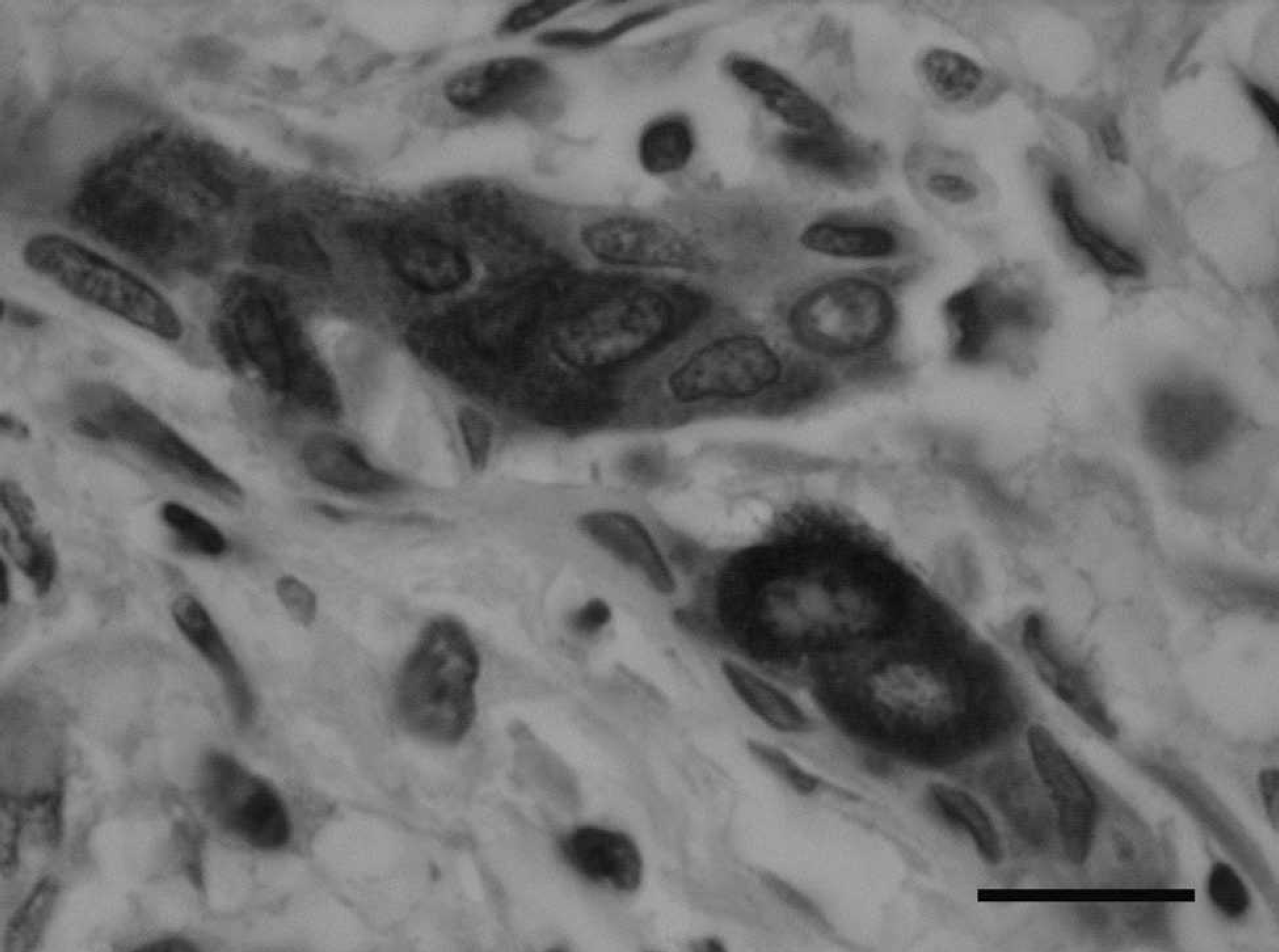
Light microscopy, mediastinal mass. Neoplastic cells stain strongly positive for cytokeratin. Immunoperoxidase stain, hematoxylin counterstain. Bar = 20 μm.

Light microscopy, mediastinal mass. Clusters of neoplastic cells have marked immunoreactivity for vimentin. Immunoperoxidase stain, hematoxylin counterstain. Bar = 20 μm.
Pleural mesothelioma is typically characterized by pleural thickening with multifocal nodules and pleural effusion. Therefore, the most common presenting sign is dyspnea from pleural effusion. 13 In the current report, the mesothelioma was a solitary mass in the cranial mediastinum with no effusion or evidence of multifocal or diffuse mesothelial involvement. The location of the mass with compression of the cranial vena cava can explain the development of the clinical signs observed in this dog. 18,27 Solitary mesotheliomas are rare in human medicine, and only 1 case has been reported in the veterinary literature. 17,23,28,35 The major differential diagnosis for localized mesothelioma in human medicine is a mesenchymal neoplasm called solitary fibrous tumor. Mesothelioma and solitary fibrous tumor cannot be easily differentiated by routine examination of hematoxylin and eosin (HE)–stained tissue sections, especially if the 2 tumors are histologically composed of predominantly spindle cells. In this case, immunohistochemical staining is required for definitive diagnosis. 17,28,35 Histologically, the diagnosis of mesothelioma is known to confound even experienced veterinary pathologists because it is a rare neoplasm in domestic animals and has a wide range of morphologic appearances. Adenocarcinoma originating from other parenchymal organs, such as mammary gland or prostate, and mesothelial cell hyperplasia represent the most important lesions in the differential diagnosis of epithelialtype mesothelioma. 16,20,36 Accurate diagnosis may be difficult by microscopic examination of HE-stained tissue sections alone, and additional immunohistochemical studies are often needed. The expression of both epithelial and mesenchymal markers (cytokeratin and vimentin, respectively) is a consistent feature in mesotheliomas because of the origin of mesothelial cells from the mesoderm that can differentiate into both epithelial and mesenchymal cells. 2,16,20,31,36 In the current neoplasm, coexpression of these antibodies was found. Cytokeratin and vimentin are also coexpressed in other neoplasms, including some anaplastic carcinomas, amelanotic melanomas, renal carcinomas, and Sertoli cell tumors, but there was no evidence of any other potential primary masses in the dog in the present study. 31 In humans, detection of calretinin (a calcium-binding protein) in tumor tissue may be diagnos-tically useful, but this marker is not useful in the diagnosis of canine mesotheliomas. 9,10,31
In humans, contrast-enhanced helical CT is the imaging technique of choice for evaluation of pleural mesothe-lioma. 4 In veterinary medicine, there is only 1 report of the use of CT for evaluation of a pleural mesothelioma. In that study, the presence of a mild pleural effusion and the use of CT allowed the authors to identify the pleural nodules. 11
The most common cranial mediastinal masses in dogs and cats are lymphoma and thymoma, followed by idiopathic mediastinal cyst, ectopic thyroid tumor, and chemodectoma. 21 Other, less frequent mediastinal neoplasms include neurogenic tumor and paraspinal tumor. 8,37 Typical pleural mesothelioma is characterized by pleural thickening with multifocal nodules and pleural effusion. 13 In the dog of the current report, the mesothelioma was a solitary mass with no evidence of multifocal or diffuse mesothelial involvement or metastatic disease in the abdominal or thoracic cavities. Solitary mesotheliomas are rare in human medicine and have only been reported once in the veterinary literature. 17,23,28,35 The anatomic distribution and clinical features of mesothelioma in the present study are similar to other cases in humans; however, to the authors' knowledge, a cranial mediastinal mesothelioma leading to compression of the cranial vena cava has not been previously described in the dog.
Footnotes
a.
Cytokeratin (Ref. M0717), Dako Denmark A/S, Glostrup, Denmark.
b.
Vimentin (Ref. M0725), Dako Denmark A/S, Glostrup, Den mark.