
Abstract
The current study compared the LeadCare® II test kit system with graphite-furnace atomic absorption spectrometry for blood lead (Pb) analysis in 56 cattle accidentally exposed to Pb in the field. Blood Pb concentrations were determined by LeadCare II within 4 hr of collection and after 72 hr of refrigeration. Blood Pb concentrations were determined by atomic absorption spectrometry, and samples that were coagulated (n = 12) were homogenized before analysis. There was strong rank correlation (R 2 = 0.96) between atomic absorption and LeadCare II (within 4 hr of collection), and a conversion formula was determined for values within the observed range (3–91 mcg/dl, although few had values >40 mcg/dl). Median and mean blood pb concentrations for atomic absorption were 7.7 and 15.9 mcg/dl, respectively; for LeadCare II, medians were 5.2 mcg/dl at 4 hr and 4.9 mcg/dl at 72 hr, and means were 12.4 and 11.7, respectively. LeadCare II results at 4 hr strongly correlated with 72 hr results (R 2 = 0.96), but results at 72 hr were lower (P < 0.01). There was no significant difference between coagulated and uncoagulated samples run by atomic absorption. Although there have been several articles that compared LeadCare with other analytical techniques, all were for the original system, not LeadCare II. The present study indicated that LeadCare II results correlated well with atomic absorption over a wide range of blood Pb concentrations and that refrigerating samples for up to 72 hr before LeadCare II analysis was acceptable for clinical purposes.
Keywords
Lead (Pb) poisoning is the most common metal toxicosis in cattle and other domestic animals 10,14 and, in living animals, is usually diagnosed based on clinical signs and blood Pb concentrations. Analysis of blood by graphite-furnace atomic absorption spectrometry (GFAAS) is a common method for Pb detection in veterinary diagnostic laboratories. 4,16 Although highly sensitive and selective for Pb, 17 GFAAS requires costly equipment that must be used by trained chemists and technicians, and results are often delayed because of the time it takes to ship samples to the diagnostic laboratories and process them for analysis. 13,16
The LeadCare® II Blood Lead Analyzer System (hereafter, LCS II) test kit a has several advantages over other methods of Pb detection in blood. The LCS II requires a sample size of 50 mcl (0.05 ml), whereas GFAAS b requires at least 100 mcl (0.10 ml). The LCS II unit is relatively inexpensive, portable, simple to use, and gives results within minutes. LeadCare has been used for Pb detection in human medicine and to a limited extent in veterinary medicine. 3–5,7,12,13,16 The manufacturer recommends that the blood samples be analyzed within 24 hr of collection.
The goal of the current study was to compare GFAAS with LCS II as methods of Pb analysis for whole-blood samples from cattle exposed to Pb in the field. Although there have been several articles that compared LeadCare with other analytical techniques, all these articles were for the original system, not LeadCare II, and all previous studies compared analysis techniques for human or avian blood samples. 4,11,16 Furthermore, in the present study, GFAAS results for homogenized coagulated whole blood were compared with results of uncoagulated whole blood, as well as use of LCS II on samples at 4 hr and 72 hr after collection (hereafter, LCS II 4 hr and 72 hr, respectively).
Blood samples were collected from 56 male, castrated, 6-month-old, crossbred beef cattle from a single herd that were accidentally exposed, for an unknown period of time, to an unknown Pb-containing substance at a nearby dump site. Samples were collected in heparinized Vacutainers c and were submitted to the Livestock Disease Diagnostic Center (LDDC; University of Kentucky, Lexington, Kentucky) for Pb analysis within 4 hr of collection. The samples were analyzed by LCS II immediately upon receipt (4 hr). Sample remains were refrigerated at 5°C for 72 hr and then reanalyzed by LCS II (72 hr). Sample size did not allow for repeated testing at either time period.
Analysis was performed on the LCS II on samples per manufacturer's instructions. a Samples were thoroughly mixed by 10–15 tube inversions and rapid rolling of tubes between the palms. Each blood sample was processed as follows: 50 mcl (0.05 ml) of room-temperature blood was dispensed into a reagent-containing test tube. In addition, 2 control samples provided with the LCS II kit were analyzed with samples at 4 hr and 72 hr. The sample and/or reagent tube was mixed thoroughly by inverting the tube 10 times. A sensor was placed in the analyzer, and the required volume of sample and/or reagent mix was placed on the sensor from a dropper supplied with the kit. The results were reported by the analyzer after 2 min. Three blood samples that were moderately to severely coagulated were not analyzed, thus 53 samples were analyzed at 4 hr and 72 hr. Results of control samples were within the target ranges given by the manufacturer of 6.9–13.7 mcg/dl for the level 1 (“low”) control and 21.8–32.6 mcg/dl for the level 2 (“high”) control. Samples with results >65 mcg/dl (the upper limit of quantitation for the analyzer) were diluted 1:1 with distilled deionized water, and reanalyzed, and the results were recalculated by incorporating the dilution factor.
Remainders of all 56 samples were shipped on ice overnight to the Animal Health Diagnostic Center (AHDC; Cornell University, Ithaca, New York). Samples underwent GFAAS Pb analysis within 24 hr of arrival (approximately 120 hr after collection) by using a transversely heated GFAAS with longitudinal Zeeman-effect background correction. Analysis was based on a published method. 8 A 100-mcl subsample was taken of each sample, placed in a 2-ml cup, d and mixed with 900 mcl of matrix-modifier solution. If a blood sample was coagulated, then it was homogenized in a disposable plastic tube by using a tissue homogenizer. e Twelve blood samples were coagulated. Matrix-modifier solution is composed of NANOpure deionized water, 0.02% analytical-grade ammonium phosphate, d 0.05% analytical grade magnesium nitrate, f 1.0% analytical-grade nitric acid, d and 0.1% Triton X. d Standards that contained 2.50, 5.00, 10.00, and 50.00 mcg/ dl Pb to construct a calibration curve were prepared by diluting certified atomic absorption standard solution g in matrix modifier and were placed in cups. d Cups that contained a matrix-modifier blank, standards from low to high concentrations, and blood samples were placed in the autosampler tray. All blanks, standards, and samples were analyzed in duplicate. The calibration curve gave a linear response across this range, with a correlation coefficient of 0.999. Two replicates of each blood sample were analyzed, and the average was taken for statistical analysis. Blood samples that contained >50 mcl/dl of Pb were diluted 1:1 in matrix-modifier solution.
Commercial software h was used for statistical analyses. Shapiro–Wilk normality tests indicate that analytical results had non-Gaussian distributions (all P < 0.0001). Results for GFAAS from noncoagulated versus coagulated samples were compared by using Wilcoxon rank-sum tests (2-sided alpha = 0.05) to determine whether coagulated samples should be included in further comparisons. Comparisons of blood Pb results between GFAAS and LCS II 4 hr were made by using correlation and Bland–Altman difference graphs 1 and the Spearman rank correlation; a least-squares linear regression was calculated to find a conversion formula that could be used to translate LCS II results to GFAAS results. LCS II 4 hr and 72 hr results were also compared by using a Wilcoxon signed rank test, Spearman rank correlation, and correlation and Bland–Altman difference graphs.
When analyzed by GFAAS, blood Pb concentrations ranged from <2.5 mcg/dl (lower limit of quantitation) to 91.2 mcg/dl (median: 7.7 mcg/dl; mean: 15.9 mcg/dl); when analyzed by the LCS II, concentrations ranged from <3.3 mcg/dl (lower limit of quantitation) to >65 mcg/dl (upper limit of quantitation by this method, highest concentration = 70.2 mcg/dl based on dilutions) at both 4 hr and 72 hr, with a median of 5.2 mcg/dl at 4 hr and 4.9 mcg/dl at 72 hr and means of 12.4 and 11.7 mcg/dl, respectively. Results from GFAAS analysis of coagulated samples were not significantly different from results from uncoagulated samples (P = 0.23).
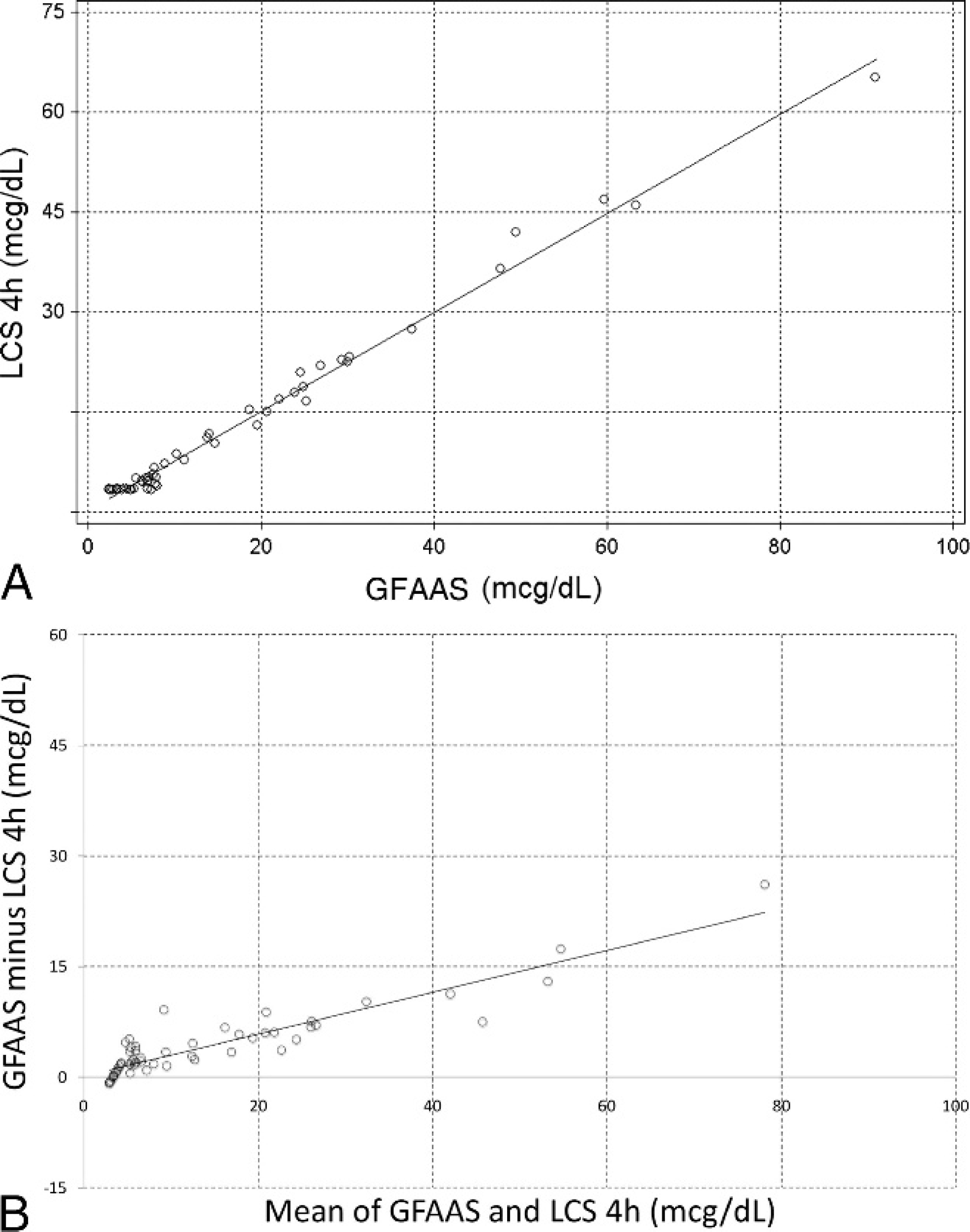
When comparing the LCS II to GFAAS results, there was strong rank correlation (r sp = 0.96; P < 0.01) but a clear systematic error (Fig. 1). Based on least-squares linear regression, a conversion formula was determined: GFAAS [Pb] = 1.33(LCS II [Pb])–0.11 (P ≤ 0.01, R 2 = 0.99). However, standardized residuals were relatively high (compared with the fitted values) at higher blood Pb concentrations.
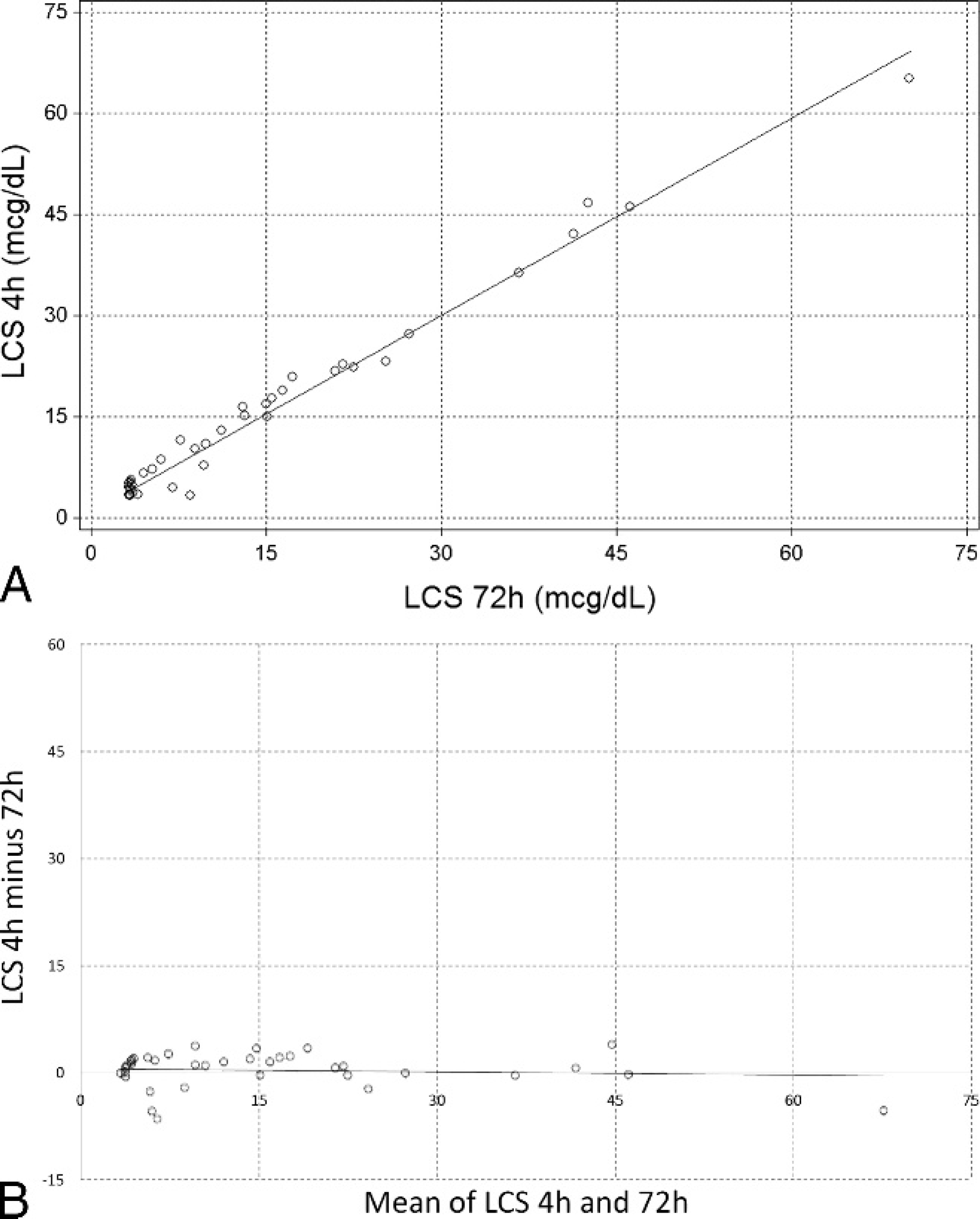
There was a strong correlation (r sp = 0.93) with LCS II measurements taken at 4 hr versus 72 hr, but values from 72 hr were significantly lower (means: 12.4 and 11.7 mcg/dl; medians: 5.2 and 4.9 mcg/dl, respectively; P = 0.0098). More importantly, despite the strong rank correlation, the disagreements arising from delayed testing with the LCS II occurred in either direction over the entire range of measurements, and the differences often were proportionally >5% of the mean measurements (Fig. 2).
The cattle in the current study were from a single herd with a history of accidental exposure to Pb. Approximately 6 steers showed acute clinical signs, including blindness, circling, head-tilt, incoordination, bruxism, and anorexia. Three of the 6 steers died and underwent postmortems at the LDDC. Exposure to Pb was diagnosed via inductively coupled plasma analysis of tissues from 2 steers at LDDC (liver Pb concentrations of 3.48 and 39.0 ppm wet weight; kidney Pb concentrations 13.9 and 156 ppm wet weight). The owner reported that the fence that separated the herd from a neighboring dump area was disrupted for an unknown period of time, and cattle had access to a white–brown granular substance found in the dump area. The granular material contained 25.4% Pb based on inductively coupled plasma analysis at AHDC. The cattle were moved to another pasture, after which time no additional steers developed clinical signs. Although all the cattle sampled for the present study were asymptomatic at the time of testing, 7 of 56 cattle had blood Pb concentrations (by GFAAS) >30 mcg/dl and 5 of 56 had concentrations >35 mcg/dl. Concentrations greater than 30 mcg/dl have been associated with Pb toxicosis in some cattle and other domestic animals (analytical method unspecified). 6,15 Because the analytical results had non-Gaussian distributions, nonparametric methods were used when possible. However, no transformation to a Gaussian variable could be found for the regression analysis, which might have contributed to the problem with the model fit (shown by the analysis of the standardized residuals).
GFAAS has historically been the most common method for blood Pb analysis and has high specificity. 17 GFAAS is commonly used in veterinary diagnostic laboratories. A 5% error tolerance has been established for GFAAS 2 (i.e., analysis of Pb in a standard reference material should yield a result that is within 5% of the accepted Pb concentration of the reference material). However, samples usually must be mailed to the laboratory for testing, which causes a delay in diagnosis and treatment. The error tolerance for LCS II is also 5% according to the package insert.
Because Pb is closely associated with erythrocytes, whole blood is the preferred antemortem sample for Pb testing in cattle and other domestic animals. 6 Use of coagulated samples is discouraged to ensure the accuracy of the Pb measurement. However, based on the current study, homogenization of coagulated samples allows GFAAS testing for diagnostic purposes when uncoagulated samples are not available.
Although the LCS II results were strongly correlated with GFAAS results, there was an unpredictable error, particularly in blood samples with Pb concentrations >40 mcg/dl. The reason for this difference is not clear and may have been because of imprecision inherent in the test kit. Only 5 of the 7 samples classified as having high Pb concentrations (>30–35 mcg/dl, consistent with toxicosis 6,14 ) based on GFAAS would have been similarly categorized as high based on LCS II (30.21 mcg/dl and 37.56 mcg/dl via GFAAS vs. 23.1 mcg/dl and 27.3 mcg/dl via LCS II 4 hr), without the use of the conversion formula. When the conversion formula was applied, these samples were categorized as high (30.6 and 36.2 mcg/dl, respectively), thus all 7 of the samples were categorized the same (>30 mcg/dl), regardless of the method of analysis. However, it should be noted that blood Pb concentrations do not correlate well with clinical signs of Pb poisoning in domestic animals, and other factors must be considered when diagnosing Pb toxicosis.
Previous comparisons of LeadCare to GFAAS analyzed human and avian blood and used the original LCS kit, not the LCS II kit used in the present study 3–5,9,11,16 (a literature search revealed no previous reports that used LCS II). LCS II was developed as a more robust kit, with less risk of technical error. LCS II includes a measuring device, does not require a calibrated pipettor, and requires control analyses with each new kit, rather than with every test, as was needed for the original LCS kit.
One study of the original LCS kit found no significant difference between results of Pb analysis by GFAAS and LCS, 11 but another study reported that Pb results were consistently higher with LCS versus GFAAS. 4 Although the latter study used blood samples acquired by finger-stick, Pb contamination from the skin was ruled out as the cause for the higher Pb result via LCS. Two other studies found that LCS results were consistently lower than GFAAS results. 7,12 This difference was attributed to glutathione interference with the test in one of the studies. 12 Some of the differences in results of those studies might be because of differences in the individual LCS analyzers. 12 LCS has been used in veterinary studies that involved waterfowl, California condors, and other raptors. 3,5,9 Results of studies found a good correlation between LCS and GFAAS on avian samples, with 93% agreement between methods on blood samples from waterfowl. 3 Furthermore, because analysis only takes minutes, captured birds need be held only briefly to determine the necessity of treatment before release. LCS could be useful in a large clinical veterinary practice for the same reasons it is useful in field research.
The LCS II unit costs between $2,000 and $3,000 and is validated for blood Pb concentrations between 3.3 mcg/dl and 65.0 mcg/dl. Although LCS II is adequate for most diagnostic purposes, GFAAS is needed for more precise quantitation of blood Pb concentrations ≥40 mcg/dl (when there were few data points). 2
A proficiency-testing program is needed when using LCS II kits in-house. Negative error caused approximately 50% underestimate of prevalence of Pb >10 mcg/dl in human patients, which caused a partial recall of the original LCS testing kits in 2005. 2 The LDDC, which uses LCS II, is used in the Wisconsin State Laboratory of Hygiene National Blood Lead and EP Proficiency Testing Program, which uses bovine whole blood as the proficiency sample. Proficiency testing is performed 6 times a year. The LDDC has a 100% pass rate for this program. Information about blood Pb proficiency testing in the United States is available through the Centers for Disease Control and Prevention.
The manufacturer of LCS II recommends that whole-blood samples be <24 hr old and stored between 10°C and 32° for analysis. a Testing within 24 hr is not always practical in veterinary practice because field collection of samples and the relative paucity of veterinary testing laboratories often require a period of refrigeration and transportation of samples. The stability of Pb and human blood has been studied. No significant difference in blood Pb concentration measured by GFAAS was detected in samples that were stored for 10 weeks at 22°, 4°, and −20° in glass or polypropylene tubes that contained ethylenediamine tetra-acetic acid or heparin. 15 Blood samples in the current study were tested by LCS II at 4 hr and after 72 hr of refrigeration. Although there was a strong rank correlation (r sp = 0.93) between results taken at these 2 time periods, the values differed in either direction. The reason for this difference is not clear and may have been because of imprecision inherent in the test kit. Fortunately, the difference between results at 4 hr and 72 hr did not change the diagnosis in any of the cattle tested (when the conversion formula was applied, the same 7 cattle exceeded the diagnostic threshold at both times and were the only cattle to do so). Thus, the difference is unlikely to be clinically relevant.
LCS II is a relatively new technology for blood Pb analysis that is more rapid than GFAAS and requires less-expensive instrumentation and technical ability to perform. The original LCS kit has had limited use in veterinary medicine thus far and has been mainly restricted to birds. 3,5,9 Results of the present study indicate that LCS II is useful for clinical determination of blood Pb concentrations in cattle. However, more research is needed to determine the reliability and potential utility of this method for other species of veterinary interest. Samples should preferably be analyzed <24 hr after collection, but holding samples for up to 72 hr under refrigerated conditions can still give clinically relevant information.
Acknowledgements
The authors thank the U.S. Department of Agriculture for funding this study and Ms. Katherine Neafsey for her help with data generation. The authors have no affiliation with or financial interest in ESA Biosciences Inc., Chelmsford, MA.
Footnotes
a.
LeadCare® II Blood Lead Analyzer System, ESA Biosciences Inc., Chelmsford, MA.
b.
PerkinElmer Inc., Waltham, MA.
c.
Heparinized Vacutainer® tubes, BD, Franklin Lakes, NJ.
d.
Auto Analyzer Cup, Krackeler Scientific, Albany, NY.
e.
IKA Ultra-Turrax®, IKA Works Inc., Wilmington, NC.
f.
Fisher Scientific Co., Pittsbu
g.
EMD Chemicals Inc., Gibbstown, NJ.
h.
Statistix™ 9 2008, Analytical Software, Tallahassee, FL.