
Abstract
The objective of the present study was to measure serum C-reactive protein (CRP) concentrations in 32 dogs with acute abdomen syndrome at presentation and after 48–72 hr. Data were evaluated to determine if there was an association between CRP concentration and outcome, and if CRP concentration correlated with the white blood cell (WBC) count at both time points. An immunoturbidimetric assay for human CRP, previously validated for use in dogs, was used for serum CRP analysis. Increased serum CRP concentrations were found in 21 dogs at presentation. Fifteen of these dogs had declining serum CRP concentrations by 48–72 hr, but 3 of the 15 dogs were later euthanized. Serum CRP concentrations increased by 48–72 hr in 4 dogs. Of the 32 dogs, 4 were dead or were euthanized prior to the 48–72 hr time point. No significant difference between initial CRP concentration and outcome was found (P = 0.054). Initial and 48–72 hr CRP values taken together were significantly different between outcome groups (P < 0.001). Serum CRP concentrations that were elevated at both time points were associated with a poor prognosis. No correlation was found between CRP concentrations and WBC counts at presentation (P = 0.83); however, a significant correlation was noted at 48–72 hr (P = 0.03). Evaluation of sequential CRP concentrations in dogs with acute abdomen syndrome may be helpful in assessing clinical response to treatment and predicting outcome. Also, serum CRP may be better in detecting tissue injury and/or inflammation at presentation than WBC counts in select cases.
Introduction
The acute phase response (APR), a part of the innate host defense system, occurs following a variety of nonspecific insults, including inflammation, infection, immune-mediated disorders, neoplasia, and trauma. 4,18 The APR includes changes in the concentrations of acute phase proteins (APPs), some of which decrease in concentration such as albumin and transferrin (negative APPs), and others which increase such as C-reactive protein (CRP), serum amyloid A, haptoglobin, alpha-1-acid glycoprotein, and ceruloplasmin (positive APPs). 4 The measurement of individual and combinations of APPs has been studied in human and veterinary medicine as a means of evaluating treatment efficacy and, in some cases, predicting future outcome. 8,12,16 Serial concentrations of serum CRP are used to predict the development of necrosis, infection, or both, and assess treatment efficacy in humans with acute pancreatitis. 2,14,22,24 As a major APP in dogs, serum CRP concentration can increase 10-fold to 100-fold in a variety of conditions, including immune-mediated hemolytic anemia, 7,16 pyometra, 6,27 infections, 12,27 acute pancreatitis, 8,12 and neoplasia. 15,17,20,23,25,26 Previous studies in dogs have demonstrated that decreasing serum CRP concentration following appropriate therapy is associated with clinical improvement. 7,11,16
Acute abdomen syndrome is a multi-etiologic clinical syndrome characterized by sudden onset of abdominal pain and additional clinical signs that may include fever, anorexia, vomiting, diarrhea, weakness, collapse, lethargy, altered gastrointestinal peristaltic activity, shock, and dyspnea. 5 Acute abdominal disease can be fatal; therefore, prognostic indicators for response to treatment and recovery are crucial. As acute abdomen syndrome involves numerous disease processes, including inflammation, infection, trauma, and neoplasia, a nonspecific indicator of tissue injury such as CRP to monitor treatment efficacy and prognosis would be very useful. Sequential serum CRP determination could provide a rapid and inexpensive means of evaluation and prognostication in affected dogs. Studies to evaluate serum CRP concentration as a prognostic indicator in dogs with acute abdomen syndrome have not been previously published.
The objective of the current study was to measure serum CRP concentrations in dogs diagnosed with acute abdomen syndrome at presentation (0 hr) and after 48–72 hr. Data were then evaluated to determine if there was an association between CRP concentration and outcome (dead vs. alive) at presentation and 48–72 hr later, and if CRP concentrations correlated with white blood cell (WBC) counts at presentation, 48–72 hr later, or both.
Materials and methods
Inclusion criteria and laboratory analyses
In the present prospective study, 32 dogs were diagnosed with acute abdomen syndrome by the attending clinicians at the Veterinary Teaching Hospital, Western College of Veterinary Medicine (Saskatoon, Saskatchewan, Canada) from May 2008 to December 2008. All dogs had to have an acute onset (24–48 hr) of 1 or more of the following clinical signs to be included in the study: abdominal pain, abdominal distention, or vomiting and diarrhea. Blood and urine samples were collected by venipuncture and cystocentesis, respectively, at presentation (0 hr) and 48–72 hr later. Four dogs died or were euthanized shortly after admission to the hospital, thus 48–72 hr sampling was not possible. Blood was collected into tubes containing a coagulation activator and a gel separator, a allowed to clot at room temperature, and centrifuged at 2,500 x g for 5 min. Routine complete blood cell count (CBC), b blood chemistry analysis, c and urinalysis were performed immediately. C-reactive protein analysis was performed within 1 month of sample collection on serum that had been separated from cells and stored at —20°C. An immunoturbidimetric assay for human CRP, d which had been previously validated for canine serum using an automated chemistry analyzer c at the Prairie Diagnostic Services Clinical Pathology Laboratory, Western College of Veterinary Medicine, was used in the current study. The established reference interval in healthy, control dogs (n = 41) was previously determined to be 0–9 mg/l (mean ± 2 standard deviations).
Cause of the acute abdomen syndrome for each dog was determined through a complete physical examination together with appropriate additional diagnostic tests for the individual patient. Some dogs required surgical intervention. Treatment modalities included any combination of antibiotics, intravenous fluid therapy, analgesics, packed red blood cells, plasma transfusion, sucralfate, famotidine, induction of emesis for gastric decontamination, anti-emetics, and glucocorticoids. Diagnoses were as follows: parvoviral enteritis (7), pancreatic disease (6), gastroenteritis (4), pyometra (2), jejunal linear foreign bodies (2), gastric ulceration (2), bladder rupture with subsequent uroabdomen and septic peritonitis (2), urinary tract obstruction (2), gastric dilatation and volvulus (1), splenic hemangiosarcoma (1), chocolate toxicosis (1), immune-mediated hemolytic anemia (1), and heatstroke (1; Table 1). Immune-mediated hemolytic anemia and heatstroke are not commonly associated with acute abdomen syndrome. However, both dogs were presented with acute onset of abdominal pain, therefore meeting the inclusion criteria for the study.
Statistical analysis
Statistical analysis was performed using specific computer software. e As there were fewer than 30 dogs in each group, nonparametric methods were used. Differences in CRP values between outcome groups were evaluated using the Mann—Whitney U-test. The repeated measures analysis of variance was used to evaluate CRP concentrations at the 2 different time points, with outcome, age, and sex as confounders. The Spearman correlation test was used to assess the correlation between WBC counts and CRP concentrations at presentation and 48–72 hr later.
Results
Final diagnoses and serum CRP concentrations at 0 hr and 48–72 hr for the study group are depicted in Table 1. The 32 dogs with acute abdomen syndrome had CRP concentrations ranging from 0 mg/l to 202.5 mg/l at presentation. Samples were available for 28 of the 32 dogs at 48–72 hr, and these CRP concentrations ranged from 0 to 91 mg/l. At initial presentation, 21 out of 32 dogs had CRP concentrations above the reference interval. The CRP concentrations declined by 18–86% in 15 out of the 21 dogs by 48–72 hr. Four of the 21 dogs with increased CRP concentrations at presentation (dogs 12, 18, 23, 27) died or were euthanized prior to the 48–72 hr time point. Eleven dogs had CRP concentrations within the reference interval at presentation and exhibited little to no change in CRP concentrations at 48–72 hr. At presentation, dogs 2 and 11 had increased CRP concentrations, which increased further at 48–72 hr. Dogs 8 and 19 had CRP concentrations within the reference interval at presentation with mild (less than 2 times the upper reference limit) increases by 48–72 hr.
No significant association was found between CRP concentrations at presentation and outcome (P = 0.054). The average decline in serum CRP concentrations between 0 and 48–72 hr in dogs that survived versus dogs that were euthanized was 52% and 61%, respectively. Although the magnitude of decrease in CRP concentration at 48–72 hr compared with 0 hr was similar in both outcome groups, there was a statistically significant difference (P < 0.001) in the initial and 48–72 hr CRP concentrations between the outcome groups (Fig. 1). Dogs that were euthanized (n = 3) had greater CRP concentrations at presentation and at 48–72 hr on average compared with dogs that survived (n = 21). C-reactive protein concentrations were not significantly associated with age (P = 0.554) or sex (P = 0.152). No correlation was noted between WBC count and CRP concentration at presentation (P = 0.83; Fig. 2); however, a significant correlation was noted between CRP concentrations and WBC counts at 48–72 hr (P = 0.03; Fig. 3) in that decreasing serum CRP concentrations paralleled decreasing WBC counts. Statistical analysis revealed 2 outliers, shown in Figure 3, and these were excluded from data correlation determination. The outliers were later determined to be the 2 cases of pyometra.
Diagnosis and serum C-reactive protein (CRP) concentrations at presentation (0 hr) and at 48–72 hr in 32 dogs with acute abdomen syndrome.*
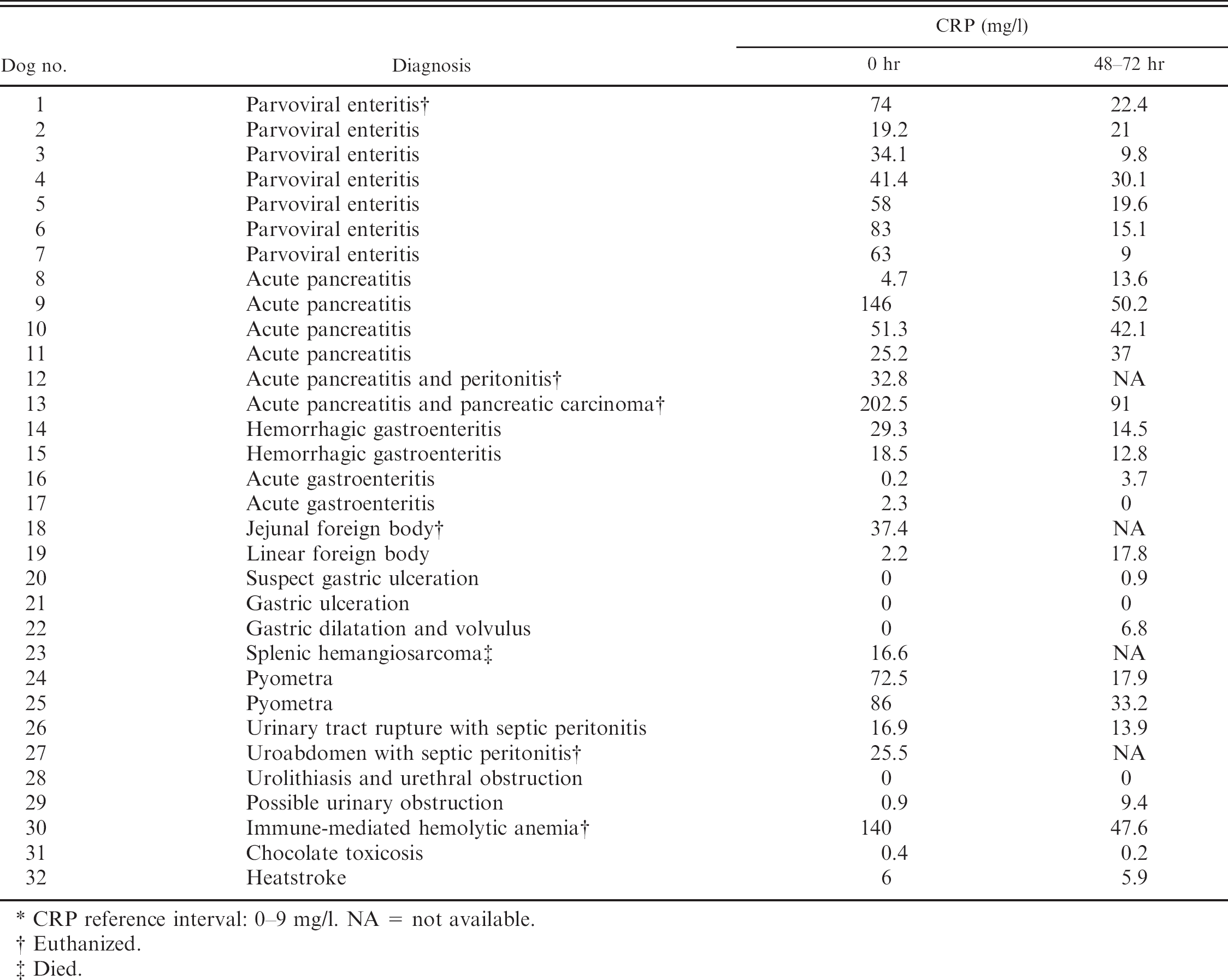
CRP reference interval: 0–9 mg/l. NA = not available.
Euthanized.
Died.
Discussion
The purpose of the present study was to determine if there was an association between CRP concentration and outcome in dogs with acute abdomen syndrome. Such an association would facilitate the evaluation of treatment modalities and prediction of survival in dogs with acute abdomen syndrome. In the current study, although serum CRP concentration was elevated on presentation in 21 out of 32 dogs, a single CRP determination did not facilitate prediction of outcome, a finding that has been previously reported in dogs with various inflammatory conditions. 3,7,8,12,13,21 Only 3 out of the 28 dogs that had serial CRP concentrations died. Figure 1 suggests that average initial CRP concentrations are predicative of survival. However, this could not be shown statistically given the low number of dogs in the group that died. As the results of the study show, sequential CRP measurement may aid in prognostication in dogs with acute abdomen syndrome. Twenty-one dogs that had elevated serum CRP concentrations, had mild to marked (18–86%) declines in serum CRP values at 48–72 hr, and were later discharged from the hospital. Interestingly, although the magnitude of the decrease in CRP concentrations was similar in both outcome groups on average, there was a statistically significant difference in the 0 hr and 48–72 hr serum CRP concentration in the group of dogs that died compared to dogs that survived. Furthermore, the 48–72 hr CRP values in the dogs that died did not approach the reference interval to the same extent as the survival group. This suggests that sequential CRP concentrations that normalize or approach the reference interval are associated with a better outcome. In addition, serum CRP values that remain elevated on sequential analysis may reflect a poorer prognosis, regardless of the inciting cause.
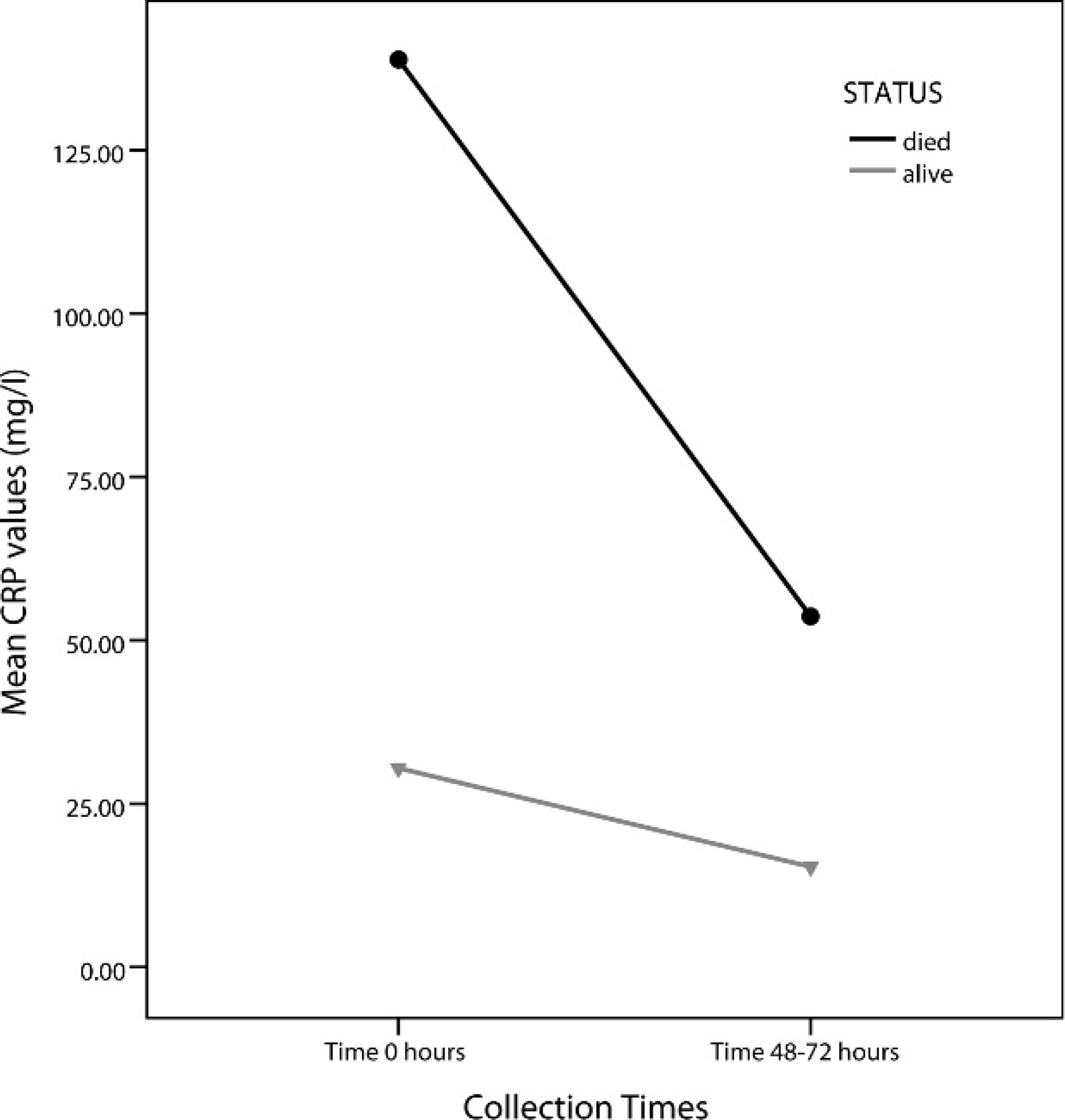
Serum C-reactive protein (CRP) concentrations at presentation (0 hr) and 48–72 hr in 2 outcome groups: dead (n = 3) versus alive (n = 28). Dogs that died had higher initial and 48–72 hr CRP concentrations compared with dogs that survived (P < 0.001).
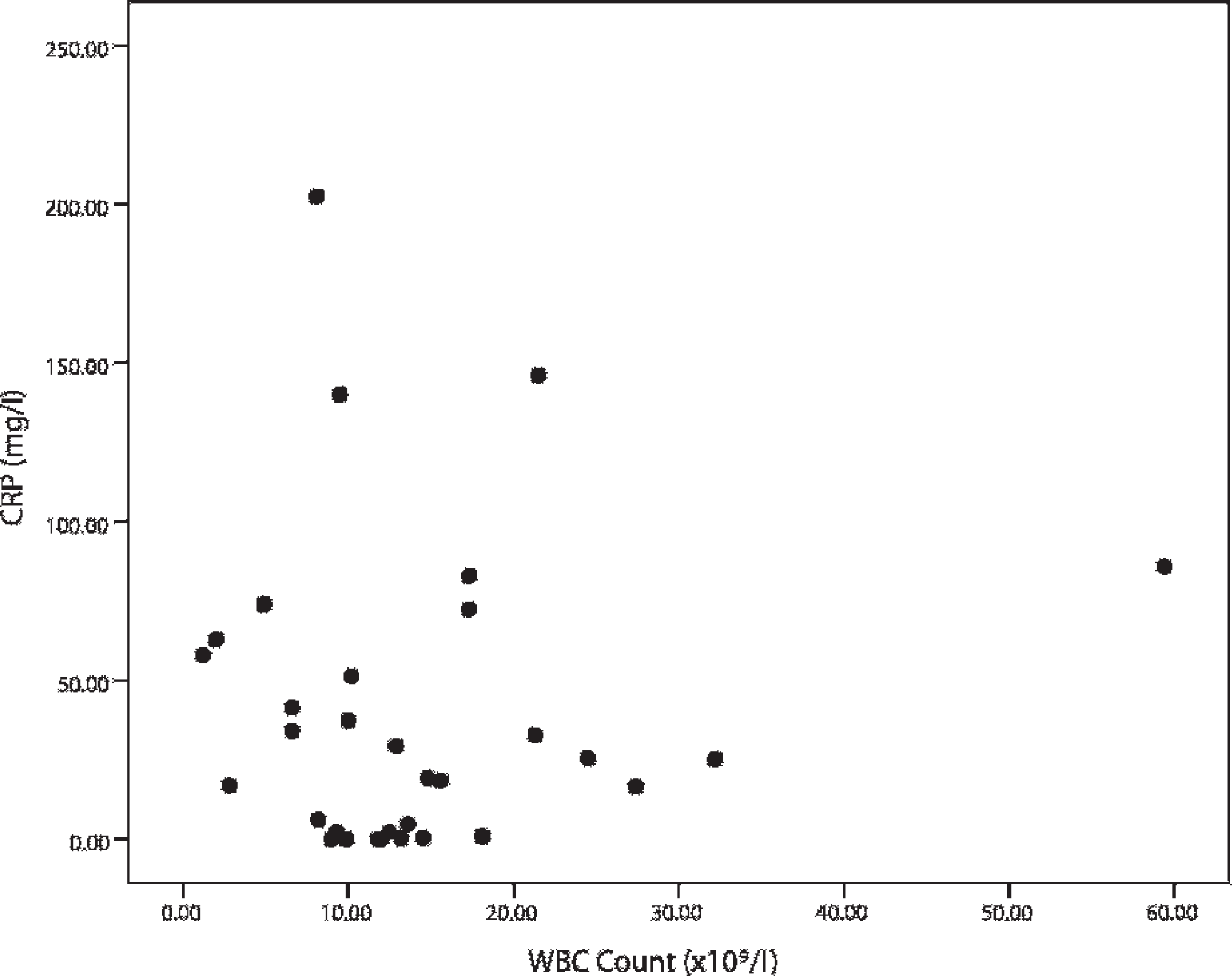
Serum C-reactive protein (CRP) concentrations and white blood cell (WBC) counts at presentation (0 hr). WBC counts did not correlate with serum CRP concentrations at 0 hr (P = 0.83).
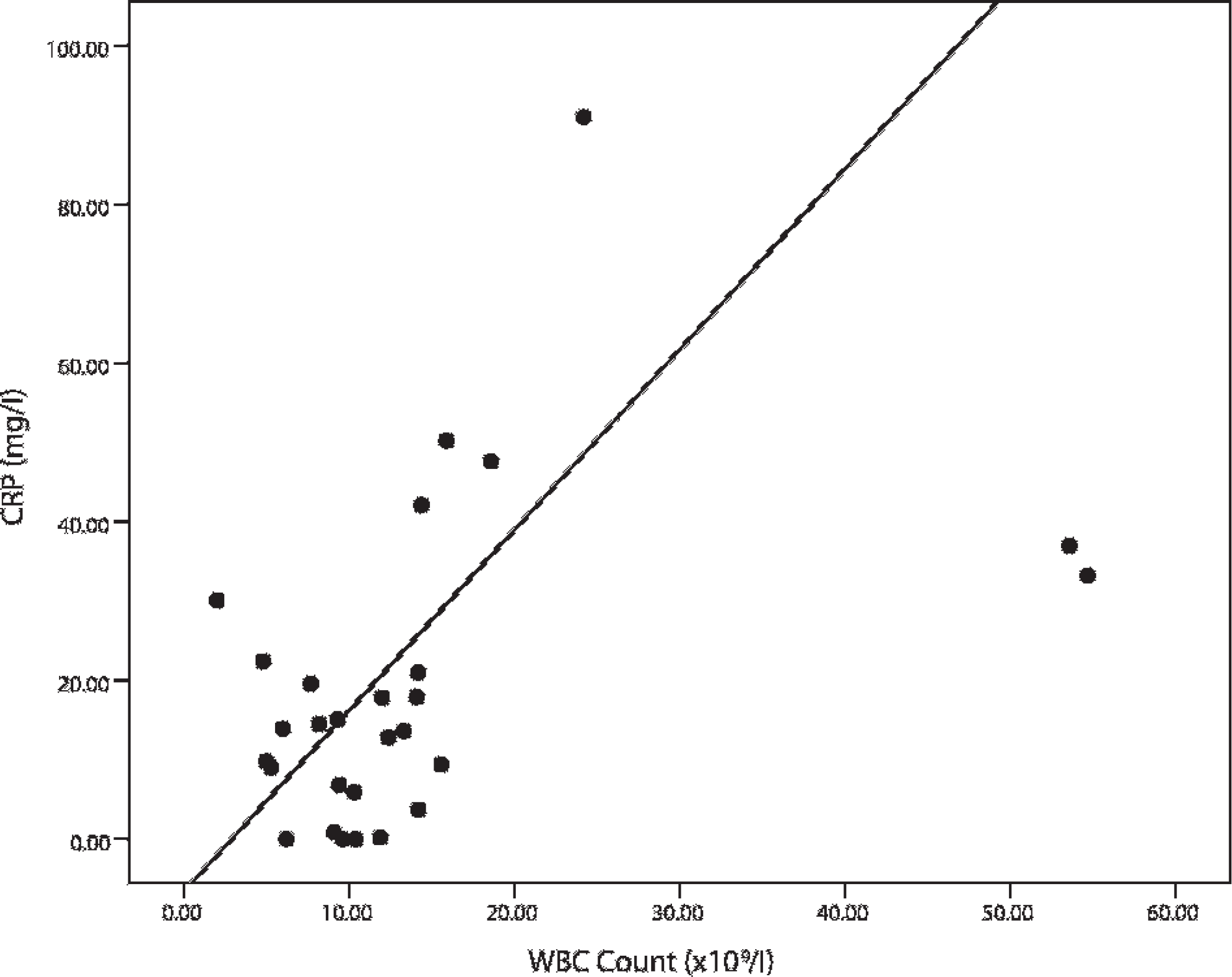
Serum C-reactive protein (CRP) concentrations and white blood cell (WBC) counts at 48–72 hr. Decreasing serum CRP concentrations correlated with decreasing WBC counts (P = 0.03). The 2 outliers to the right of the graph represent the 2 cases of pyometra where a rebound/exaggerated leukocytosis occurred following ovariohysterectomy, as expected.
Dogs in the present study with similar diseases, such as acute pancreatitis, had variable CRP values on presentation; some were even within the reference interval. One hypothesis for the lack of association between CRP elevations and pancreatitis is the timing of CRP measurement with respect to stage and onset of disease. 12,24 Serum CRP concentrations are thought to relate to the extent of tissue damage and/or inflammation; 18 however, only 1 dog had a pancreatic biopsy to assess tissue damage/inflammation in the current study. Although CRP response can vary dramatically in different individuals with the same disease process at presentation, evaluating sequential measurements and degree of decrease in serum CRP concentrations may provide more useful information than a single CRP value. Generally, serum CRP concentrations in dogs with inflammatory bowel disease, 10 immune-mediated polyarthritis, 11,21 and immune-mediated hemolytic anemia 7,16 decrease as clinical signs and leukocytosis resolve in response to therapy. Excluding dogs that were euthanized or died soon after initial CRP analysis in the current study, 88% of dogs with elevated CRP values at presentation had decreases in CRP concentrations by 48–72 hr. The declining sequential serum CRP concentrations in these dogs suggested a good response to therapy. However, successful treatment cannot be determined solely based on sequential CRP levels given that 3 such dogs (1, 13, and 30) were ultimately euthanized due to a poor prognosis or poor response to therapy. Dogs 1 and 30 had parvoviral enteritis and immune-mediated hemolytic anemia, respectively, and were refractory to treatment for these diseases. Dog 13 was found to have a pancreatic carcinoma in addition to pancreatitis. Although CRP concentrations in dogs 1, 13, and 30 declined between presentation and 48–72 hr, mean serum CRP values remained significantly above the reference interval compared with the dogs that survived. This suggests that more than 2 sequential CRP concentrations may be required to better assess disease progression and response to therapeutics, and that sequential CRP values that remain markedly above the reference interval may be associated with a poorer prognosis. A larger test group would be required to determine the relationship between sequential CRP levels and death or euthanasia as only 3 dogs in the current study were euthanized within the time interval that permitted 2 sequential CRP determinations.
Two dogs (dogs 24 and 25) with pyometra had marked decreases in serum CRP concentrations at 48–72 hr compared with presentation. C-reactive protein concentrations in dog 24 decreased from 72.5 mg/l to 17.9 mg/l and in dog 25 from 86 mg/l to 33.2 mg/l. Serum CRP concentrations at admission were comparable with previously published results for dogs with pyometra. 6,27 On initial presentation, dogs with pyometra frequently have an inflammatory leukogram (leukocytosis, neutrophilia, and a left shift). Following ovariohysterectomy, a rebound/exaggerated leukocytosis commonly occurs. Granulocytic hyperplasia is established in the bone marrow, and neutrophils continue to be released into the peripheral blood for several days after the focus of infection, the uterus, is removed. 9 In that situation, rising WBC counts can be misinterpreted as worsening or ongoing inflammation or both by the clinician. Serum CRP concentrations determined prior to and after ovariohysterectomy can be a more reliable, rapid, and sensitive indicator of resolution of inflammation/infection and improving health status than trends in the WBC count. Serum CRP concentrations at the 48–72 hr time point in the 2 cases of pyometra declined substantially when compared to serum CRP concentrations at presentation; however, surgical intervention likely accounted for serum CRP concentrations remaining above the reference interval at the second time point.
Acute phase proteins such as CRP have a higher diagnostic sensitivity than leukocyte counts in detecting inflammation and are increased in cases in which total and differential WBC count show no changes. 4,19 Significant increases in serum CRP concentrations can be seen 4 hr after initiation of inflammation without concurrent elevations in WBC counts. 4 The lack of association between serum CRP concentrations and WBC counts at presentation is likely attributed to the rapid production of CRP; thus, CRP may be a better indicator of tissue injury early in the course of disease. A direct correlation was noted between serum CRP concentrations and WBC counts at 48–72 hr. Excluding the 2 cases of pyometra, normalizing serum CRP concentrations paralleled normalizing WBC counts at 48–72 hr, coinciding with effective treatment and resolution of clinical signs.
Among the 28 dogs with sequential CRP determination, 4 dogs (dogs 2, 8, 11, 19) had higher CRP concentrations at 48–72 hr compared with presentation (Table 1). Dogs 2 and 8, which were diagnosed with parvoviral enteritis and acute pancreatitis, respectively, were discharged from the hospital 1 day after the second CRP analysis as the animals showed clinical improvement. Ongoing inflammation as a result of incomplete response or delayed therapy could explain the increasing CRP concentrations. Monitoring CRP concentrations at more than 2 time points may improve assessment of dogs with acute abdomen syndrome based on the CRP trends noted in dogs 2 and 8. Dog 19 underwent exploratory surgery to remove gastric and enteric foreign material. The 48–72 hr CRP analysis was performed on blood taken a few hours after surgery, which may have contributed to or caused the rapid increase in CRP in this dog, as has been previously reported. 4,27 One month following discharge from the hospital with an initial diagnosis of acute pancreatitis, dog 11 returned and was diagnosed with hepatitis, congestive heart failure, and abdominal effusion. Serum CRP concentrations may not have normalized at 48–72 hr because of ongoing or underlying disease and an incomplete response to treatment. 16,26 Persistently elevated serum CRP concentrations in patients receiving appropriate therapy warrants further clinical investigation to determine if additional and/or secondary conditions exist. 16,26,27
Not all dogs with acute abdomen syndrome had CRP elevations at presentation in the current study. Gastric mucosal injury experimentally produced by the administration of nonsteroidal anti-inflammatory drugs has been associated with rapid elevations in serum CRP and other APPs. 1 In the current study, serum CRP concentrations were within the reference interval in dogs with gastric ulceration (dogs 20 and 21). Gastroscopy was not conducted to determine the extent of injury in either case. Reason for the lack of CRP response in these dogs is unknown. Elevations in CRP were not present in certain dogs with conditions involving the gastrointestinal and urinary tracts, such as gastroenteritis (dogs 16 and 17), gastric dilatation and volvulus (dog 22), and urolithiasis (dogs 28 and 29), a finding that has been previously reported. 19,27 C-reactive protein may not be a sensitive indicator of tissue injury and/or inflammation in the urinary system and with specific gastrointestinal diseases. 4 Studies evaluating CRP concentrations in additional dogs with urinary or gastrointestinal conditions of various types are warranted.
In summary, initial serum CRP concentrations were not predictive of outcome in dogs with acute abdomen syndrome. Persistent elevations in serum CRP concentrations at presentation and at 48–72 hr were associated with a poor prognosis in dogs with acute abdomen syndrome. Dogs whose serum CRP concentrations reached normalcy within 48–72 hr of initial presentation were later discharged. Conversely, rising CRP concentrations despite appropriate therapy warrant additional diagnostic investigation as a secondary/underlying disease process may be contributing to the CRP elevation. Sequential CRP determination may provide better insight into tissue injury and, together with sequential WBC counts, may allow a means of evaluating persistence of disease and efficacy of treatment in dogs with acute abdomen syndrome. Additional studies, particularly in dogs that do not survive acute abdomen syndrome, may help determine a CRP level predictive of a negative outcome.
Acknowledgements
This research study was funded by the Companion Animal Health Fund, Western College of Veterinary Medicine. The authors would like to thank Mrs. Gloria Patry, Prairie Diagnostic Services, the clinicians at the Veterinary Teaching Hospital for enrolling dogs in this study, and Dr. Tasha Epp for performing the data analysis.
Footnotes
a.
Vacutainer®, BD, Franklin Lakes, NJ.
b.
CELL-DYN 3500, Abbott GmbH & Co. KG, Ludwigshafen, Germany.
c.
Hitachi 912 analyzer, Boehringer-Mannheim, Mannheim, Germany.
d.
Randox Laboratories Ltd, Crumlin, United Kingdom.
e.
SPSS software, version 16.0, SPSS Inc., Chicago, IL.