
Abstract
Pulmonary alveolar microlithiasis (PAM) is a rare pulmonary disorder characterized by the accumulation of calcium phosphate microliths within the alveoli, with only a few cases described in animals. A 10-year-old female Bulldog was euthanized due to history of dyspnea and recurrent pleural and pericardial effusions. At necropsy, numerous multifocal to coalescent protruding nodules of 1–5 mm in diameter were scattered throughout the thoracic serosal surfaces. Moreover, lungs showed a diffuse pale gray color and had a generalized fine grainy consistency. Histological investigations revealed abundant intra-alveolar laminated microliths that stained positive with periodic acid–Schiff and von Kossa stains. The pulmonary interstitium showed multifocal, mild to moderate thickening, due to collagen deposition and mild hyperplasia of type 2 pneumocytes. The pulmonary lesion was not associated with any inflammatory response, and mineral deposition was not observed in any other organ or tissue. In addition, pulmonary, pericardial, and pleural surfaces were extensively infiltrated by an epithelioid mesothelioma. Immunohistochemical staining revealed neoplastic cells that strongly coexpressed vimentin and cytokeratin, supporting the diagnosis of mesothelioma. An overview of PAM, including pathogenesis and histological characteristics, are discussed in relation to the concurrent pleural mesothelioma. The potential cause and effect relationship between the 2 conditions could neither be established nor ruled out.
Pulmonary alveolar microlithiasis (PAM) is a rare disorder characterized by the deposition of calcium phosphate within the alveoli of the lungs. The deposition usually occurs in the absence of any known disorder of calcium metabolism and quite often is not associated with an inflammatory response. 6 The progression of the disease is generally very slow, and patients can be asymptomatic for years or even decades. Therefore, its diagnosis is usually incidental in both human and veterinary species.12,21 Pulmonary alveolar microlithiasis shows both sporadic and familial occurrence. 9 In human beings, approximately one third of cases are hereditary, with an autosomal recessive inheritance and complete penetrance.6,20 Mutations of the SLC34A2 gene, which encodes a type IIb sodium phosphate cotransporter (NaPi-IIb), are considered to be the cause of the disease, leading to intra-alveolar accumulation of phosphate that favors the formation of microliths. 10 However, the disease in animals is still of unknown cause, probably because of the low number of diagnosed cases. The condition was first described in human beings in 1918, 13 whereas the first report in veterinary species was described 50 years later in a dog. 18 To date, documented reports of PAM can be found only in 5 dogs,2,5,18,21 a cat, 3 a binturong (Arctictis binturong), 4 a breeding colony of Afghan pikas (Ochotona rufescens rufescens), 19 an orangutan (Pongo pygmaeus), 16 an alpaca (Vicugna pacos), 17 and in mice. 23 Herein, a case of PAM associated with a pleural and pericardial mesothelioma in a Bulldog is described.
A 10-year-old spayed female Bulldog weighing 30 kg was presented to the Veterinary Hospital Zurich (Vetsuisse Faculty of the University of Zurich, Switzerland) with a history of recurrent pleural and pericardial effusion and dyspnea. The dog had been treated with repeated pericardiocentesis and finally by subtotal pericardiectomy 2 years before the time of euthanasia. No gross lesions were observed in specimens of the parietal pericardium, and no histological examination of the pericardial tissue was performed. Following pericardiectomy, the dog had subsequent recurrent pleural hemorrhagic effusions. Due to poor prognosis, the dog was euthanized; postmortem examination was performed, and tissue specimens were obtained for detailed histological and immunohistochemical investigations.
Specimens of various thoracic and abdominal organs, including the pleural and epicardial masses and lung, were fixed in 10% buffered formalin, routinely processed, paraffin-embedded, sectioned at 3 µm, and stained with hematoxylin and eosin for light microscopic examination. Selected sections of lung tissue were stained with periodic acid–Schiff (PAS; 0.5% periodic acid solution, Schiff reagent, counterstained with Mayer hematoxylin), von Kossa (3% aqueous silver nitrate solution, 5% sodium thiosulfate, counterstained with 0.1% nuclear fast red solution), and Prussian blue (2% aqueous solution of hydrochloric acid, 2% aqueous solution of potassium ferrocyanide, counterstained with nuclear fast red solution). For immunohistochemical evaluation of pleural and epicardial masses, sections of the tumor masses were incubated with commercially available antibodies to pan-cytokeratin a (anti-mouse, 1:50) and vimentin b (anti-mouse, 1:100). The standard avidin–biotin–peroxidase technique was used to demonstrate the antigen.
At necropsy, the pleural cavity contained 2–3 liters of serosanguinous fluids. Numerous multifocal to coalescent, tan to yellowish-red, firm, solid protruding nodules of 1–5 mm in diameter were scattered throughout the epicardial membrane, the pulmonary pleura, and, multifocally but less extensively, on the costal pleural surfaces (Fig. 1). Moreover, the lungs showed a diffuse pale gray color, were diffusely mildly rigid with a reduced elasticity, and had a generalized fine grainy consistency on palpation and on cut section.
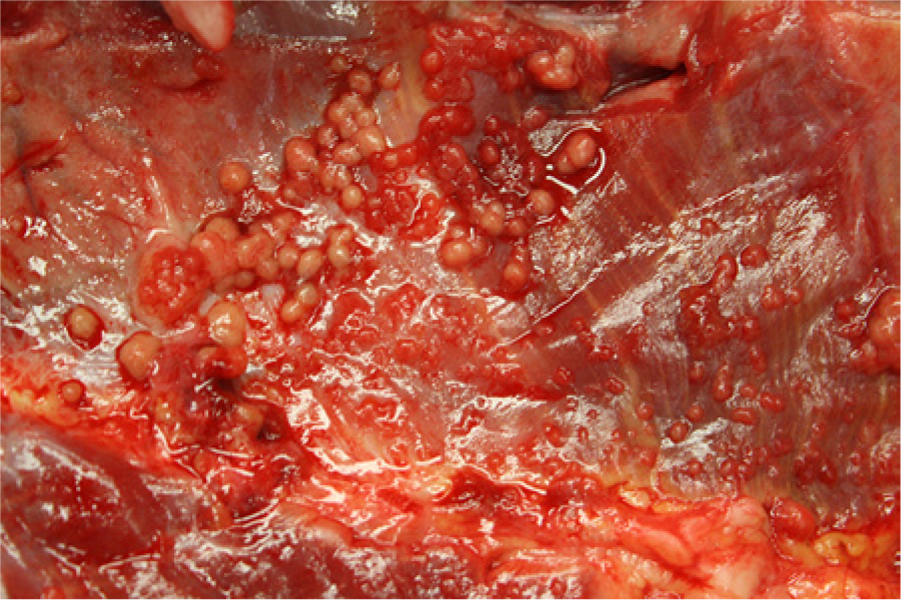
Parietal pleura; Bulldog. Numerous multifocal to coalescent, tan to yellowish-red, firm, solid protruding nodules scattered throughout the costal and diaphragmatic pleural surface.
Histologically, lungs showed abundant multifocal accumulations of circular to irregularly shaped, variably sized (30–100 µm), densely basophilic, nonbirefringent, amorphous to laminated concretions (microliths) that were either attached to the alveolar walls or found free within alveoli, involving up to 80% of the alveolar spaces (Fig. 2A). Some microliths were fragmented, with the majority of fracture lines showing a radial pattern. Others resembled homogeneous structureless spheroids or irregularly shaped masses. In hematoxylin and eosin sections of the lung, the staining of the central cores and peripheral lamellae of the microliths varied from red to bluish-purple, with the central areas appearing either lighter or darker than the periphery. Multifocally and quite often, there was mild to moderate disruption of the alveolar septae and compression of the pulmonary tissue adjacent to the microliths. Nevertheless, no inflammatory response was observed within the pulmonary parenchyma. Multifocally, the pulmonary interstitium showed mild to moderate thickening due to collagen deposition, as was demonstrated by Gomori blue trichrome stain (Fig. 2B). Mild hyperplasia and hypertrophy of type 2 pneumocytes was also multifocally present, and mineral deposition was not observed in any other organs or tissues. The concentric lamellae and cores of the microlith intensely stained in shades of purple with PAS stain (Fig. 2C). Furthermore, the microliths stained brownish to black with von Kossa stain (Fig. 2D). Finally, microliths did not stain with Prussian blue. A diagnosis of PAM was made based on the size, location, and morphology of the concretions and the absence of an inflammatory response.
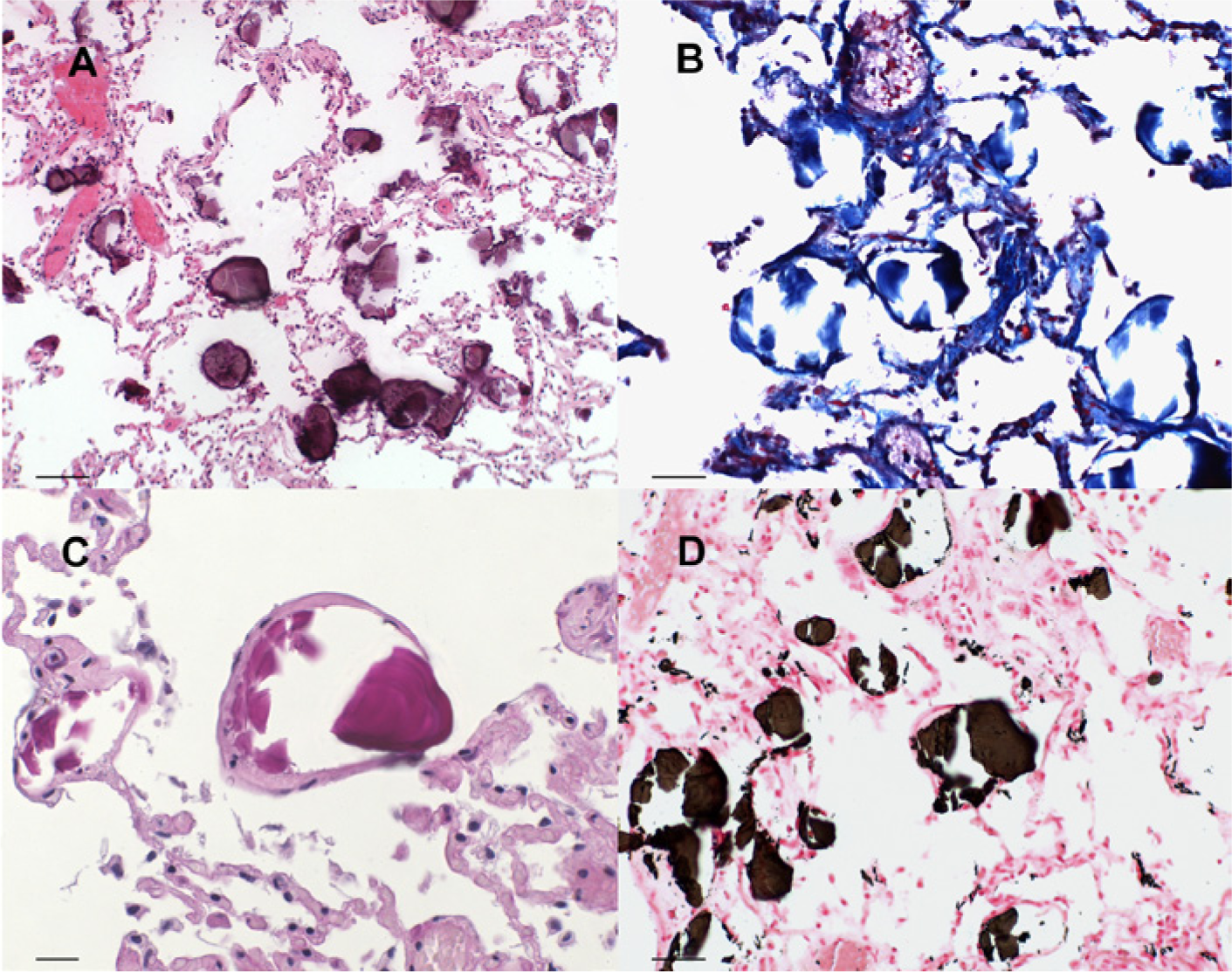
Lung; Bulldog.
Histologically, pleural and epicardial surfaces were markedly thickened due to 1 or multiple layers of epithelial-like neoplastic cells showing papillary outgrowths supported by thin to moderately thick fibrous connective tissue (Fig. 3A). Neoplastic cells measured 15–25 µm in diameter, were cuboidal to polygonal in shape, and were characterized by small to moderate amounts of eosinophilic homogenous to finely granular cytoplasm, distinct cell borders, and occasionally showed microvillus borders. The nuclei were central or eccentric, round to oval, and characterized by finely stippled basophilic staining chromatin and 1–2 prominent eosinophilic nucleoli. The degree of anisocytosis and anisokaryosis was moderate, and few regular mitotic figures were observed (0–1 per high-power field). The neoplasm had multifocal areas of necrosis and hemorrhage, as well as multifocal areas with moderate numbers of infiltrating lymphohistiocytic cells and few neutrophils. No evidence of metastasis to any parenchymal organs was seen.
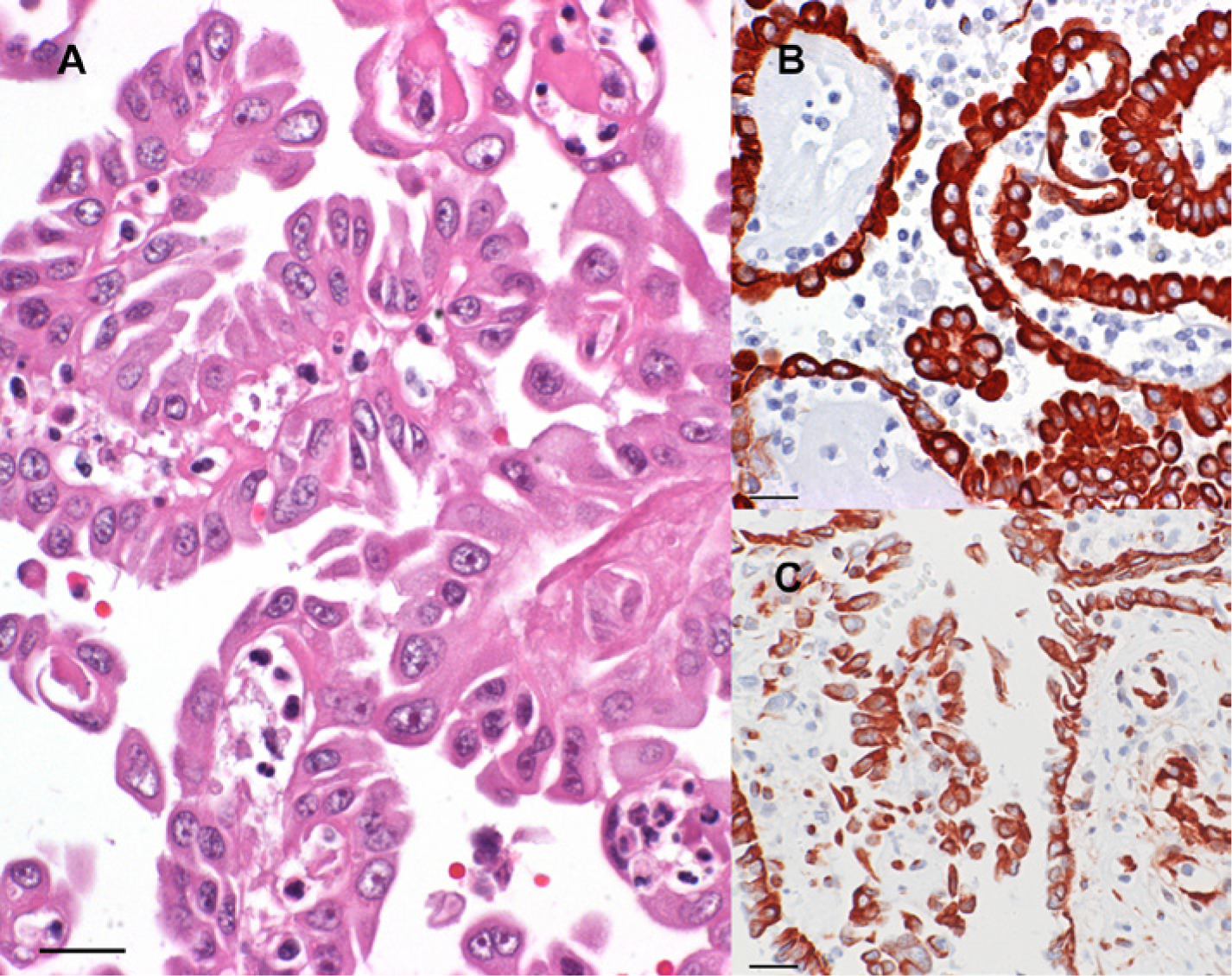
Pleural mesothelioma; Bulldog.
Immunohistochemical staining of the tumor cells revealed a diffuse intracytoplasmic labeling of moderate and high intensity for vimentin and pan-cytokeratin, respectively (Fig. 3B, 3C). The diagnosis of an epithelioid pleural and pericardial mesothelioma with associated pulmonary alveolar microlithiasis was made based on the characteristic gross, histological, and immunohistochemical findings.
In summary, concurrent diagnosis of PAM and pleural mesothelioma is made in an adult spayed female Bulldog. The staining and other histomorphological characteristics of the intra-alveolar concretions are characteristic of PAM 12 and remarkably dissimilar from that associated with metastatic and dystrophic calcification, where mineral deposits are located in the interstitial compartment or associated to areas of necrosis, respectively. 8 In agreement with previous reports,12,22 characterization of the intra-alveolar microliths showed strong positive histochemical reactions with PAS and von Kossa stains. The strong positive reaction obtained with von Kossa stain demonstrates a high content of calcium salts within the microliths. Additionally, concretions did not stain with Prussian blue staining suggesting absence of iron. On the other hand, gross, histomorphological features, and immunohistochemical staining characteristics of the thoracic and pleural nodules were diagnostic for mesothelioma. Neoplastic cells were immunoreactive for both cytokeratin and vimentin. The 2 immunohistochemical markers are useful for differentiating mesothelioma from other neoplasms, as the latter tumors consistently coexpress both epithelial and mesenchymal antigens. 26
Mesotheliomas are tumors that arise from cells lining the coelomic cavities, including the pleura, pericardium, peritoneum, and occasionally, the vaginal tunic of the testis. In the present case, the neoplastic process involved both the pleural and visceral pericardial surfaces making it rather uncertain as to the primary site of origin of the tumor. However, the extensive involvement of the visceral pleura in both lungs together with the fact that most mesotheliomas tend to occur in the pleural surface rather than in the pericardium, 15 makes pleural origin more likely in the present case. Mesothelioma has 3 distinct histological patterns: epithelioid, fibrous or sarcomatoid, and mixed cell or biphasic. 14 The present case showed an epithelioid pattern, which, together with the biphasic type, is one of the most common mesothelioma variants reported in dogs. 15 Factors implicated in the pathogenesis of mesothelioma are exposure to asbestos, iron, or silica dust in industrial settings, 26 in addition to viral or genetic factors.7,25,27 In the current case, there was no known history of exposure to industrial dusts nor occurrence of cases of mesotheliomas in relative dogs. Finally, no lesions suggestive of any viral infections were observed in the studied organs and tissues.
The respiratory clinical signs caused by pleural effusions observed in the present case were attributed to the mesothelioma. On the other hand, however, PAM was considered to be an incidental finding in this dog. Indeed, PAM is an uncommon alveolar filling disorder usually diagnosed incidentally. Human patients affected with PAM are often asymptomatic for years with a generally stable, though progressive course of the disease. 12 In those cases where clinical signs are observed, human patients typically present with progressive dyspnea and reduced pulmonary function. Respiratory insufficiency may eventually progress to pulmonary fibrosis, end-stage lung disease, and chronic pulmonary heart disease. In severe cases, death is often due to a combination of pulmonary dysfunction, pulmonary hypertension, and subsequent cor pulmonale.6,12 Studies have confirmed that familial PAM cases are caused by autosomal recessive inheritance of a mutation in the gene SLC34A2. 10 In addition, several reports have suggested that environmental factors may play a role in the etiology. 22 Whether individual susceptibility plays a major role in the pathogenesis of PAM following exposure to sand, silica, or other extrinsic factors is still unclear. The occurrence of PAM in animals is very rare with only a limited number of cases reported in the literature. Reports of 5 dogs with PAM can be found that showed a varied clinical and pathological presentation including ruptured chordae tendineae and hard, incompressible lungs in 1 dog 18 ; 2 dogs with chronic Strongyloides stercoralis infection 5 ; a dog with hypothyroidism 2 ; and a dog suffering from osteoarthtitis. 21 When comparing the pathological findings described in the previous cases, no common lesion other than PAM could be found. All 5 cases showed a multifocal and generalized deposition of microliths within alveolar lumen, with variable interstitial fibrosis. It is worth mentioning that interstitial fibrosis was also observed in the present case, which, together with the hyperplasia of pneumocytes type 2, might be due to the physical damage that microliths cause to the alveolar walls. The 5 canine cases previously reported all belong to different and unrelated breeds and the dogs ranged from 4 months to 11 years old. Similarly, human PAM cases are reported to occur at any age, ranging from a few months to advanced age, with the mean age of diagnosis being 35 years. 12 Regardless, a higher number of descriptions in veterinary species is necessary to contrast this and other epidemiological factors. While the etiology of PAM in veterinary species remains obscure, both genetic and environmental factors are suspected. In the present case, it is unknown if PAM occurred in other blood-related dogs. Moreover, as mentioned above, the owner reported no exposure to dust or pollutants other than the ones usually present in the city where he lived with his dog.
A possible association between PAM and mesothelioma in the present case cannot be ruled out. There are 3 possibilities to explain the concurrent presentation of both lesions: 1) initial development of mesothelioma followed by PAM; 2) PAM developing first and then followed by the mesothelioma; or 3) independent formation of both PAM and mesothelioma, without any cause–effect connection between the 2 lesions. In favor of the first hypothesis, there is a report describing human PAM cases in a single area of the lung as a secondary localized lesion associated with adenocarcinoma or pleural mesothelioma. 1 In the present case, both the mesothelioma and PAM extensively affected the pulmonary pleura and pulmonary parenchyma, respectively. As such, a focal initial relationship of both lesions cannot be ruled out. Supporting the second hypothesis, a similar association has been suggested in some testicular tumors and testicular microlithiasis (TM) in human beings.11,24 Testicular microlithiasis has been linked to an increased risk for developing germ cell tumors; it is proposed that TM may result from the same genetic abnormalities as germ cell tumors. 11 Even though TM is not uncommon in human beings, this condition, to the authors’ knowledge, has not been described in dogs. Additionally, an association between prostate microlithiasis and mammary calcifications and malignancies have also been described in human beings. 10 On the other hand, it is well known that mesotheliomas are associated with inhalation of asbestos fibers or other foreign body materials.26,27 Taking into account that, in the present case, the pulmonary pleura was more extensively affected than the parietal pleura, it may be speculated that the presence of microliths could have acted as a foreign material inducing damage to visceral pleura and leading to tumor development. Nevertheless, it might also be possible that the relationship between the 2 lesions was not of cause–effect nature. In this regard, both lesions are reported to be etiologically linked to inhalation of environmental substances,22,27 although the influence of such factors could not be evidenced in the present case. Finally, it cannot be ruled out that concurrence of both lesions was purely incidental. The study of potential future cases showing both conditions in the same individuals might elucidate whether such an etiological relationship exists between both lesions. Further studies of PAM might also lead to a better understanding of the epidemiology and pathogenesis of this disorder in veterinary species.
Footnotes
Acknowledgements
The authors would like to thank Dr. Karoline Forster (Clinic for Small Animal Medicine, University of Zürich) for presenting the dog for necropsy.
a.
Product no. M082101, Dako Sweden AB, Stockholm, Sweden.
b.
Product no. M7020, Dako Sweden AB, Stockholm, Sweden.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.