
Abstract
This study presents a case of a canine thymolipoma, which is a rare, slow-growing, benign tumor of the thymus composed of mature adipose tissue and thymic tissue. A 9-year-old spayed, female miniature pinscher presented with chronic cough and dyspnoea. Radiology revealed pleural effusion and a mediastinal mass with a fatty appearance. The mass was attached to, and silhouetted, the adjacent pericardium. Microscopically, the mass was composed of adipose tissue with numerous cords and nests of thymic tissue without corticomedullary arrangement. To the authors' knowledge, this is the first description of this uncommon neoplasm in a dog. The gross and histological findings are similar to those described for thymolipomas in humans. The possible histogenesis for this neoplasia in a dog is also discussed.
Tumors arising from the thymus in domestic animals include thymomas and lymphomas. 9 Thymic lymphomas are lymphoblastic or immunoblastic true lymphoid tumors, whereas the term thymoma is restricted to define those neoplasms arising from thymic epithelial cells; the lymphoid component is regarded as secondary. 9 Thymomas have been classified as predominantly lymphocytic, predominantly epithelial, or mixed (lymphoepithelial) on the basis of the proportion of proliferating epithelial cells and lymphocytes. 5,9 In humans, thymic neoplasms include lymphomas, thymomas, carcinomas, carcinoids, germ cell tumors, and thymolipomas. 8,10 Thymolipomas are rare, slow-growing, benign tumors of the thymus composed of mature adipose tissue and thymic tissue. They have also been called lipothymomas or thymolipomatous hamartomas and represent 2–9% of all human thymic neoplasms. 7 Review of the veterinary literature yielded only 1 documented case of thymolipoma in an adult cat. 10 This paper describes the clinical and histopathological characteristics of a thymolipoma in a dog with features very similar to those reported for other species.
An obese, 9-year-old, spayed, female miniature pincher dog weighing 3.5 kg was presented at the Clinica Veterinaria Castellarano (Italy) in July 2006 for chronic cough and open-mouth breathing of 2 weeks duration. No other symptoms were reported by the owner. On physical examination, the dog showed dyspnea. Rectal temperature at presentation was 38.4°C, pulse was slightly reduced, and respiratory rate was 32 breaths per min with abdominal effort. The complete blood count (CBC) was normal, and the biochemical profile showed a mild elevation in cholesterol (270 mg/dl; range 120–255). Urine analysis was unremarkable. The veterinarian suspected a cardiac problem and the animal was referred for a radiographic and echocardiographic examination.
Radiologically, a homogeneous opacity obliterated the cardiac silhouette and displaced the lung lobes from the thoracic wall margins. The trachea was elevated, parallel to the vertebral column, and narrowed in the caudal portion (Fig. 1A). Ill-defined soft tissue opacity was seen dorsal to the tracheal carina and caudal trachea. The diaphragmatic margin was partially obliterated by the soft-tissue opacity, but the abdominal organs appeared normal. The radiographic diagnosis was severe pleural effusion. Radiographs of the patient 24 hr after pleural drainage showed a better defined cardiac silhouette. The lungs were less retracted from the thoracic wall, and the caudal trachea was narrowed to a lesser degree. A mass resembling fat effaced the right margin of the cardiac shadow and extended cranially in the right hemithorax (Fig. 1B). Ultrasonography revealed an abundant, anechoic fluid present in the pleural space. A hyperechoic mass resembling fat/fibrinrich tissue was also evident partially attached to the right-dorsal side of the pericardium and partially free-floating in the pleural effusion (Fig. 2). The mass was approximately 1.3 × 2.5 cm long and only 0.5 cm thick, irregular, triangular-shaped, with round margins and a fine nonhomogeneous parenchyma (some areas were less echogenic). No cavities or anechoic areas were present. The owner declined a thoracic computed tomography (CT) examination.
Fluid from the thorax was white-colored, which suggested chylous or pseudochylous effusion, but cytology identified an aseptic exudate rich in small lymphocytes. A differential diagnosis of inflammation or neoplasia was made. Amoxicillin and clavulanic acid a (20 mg/kg PO q12h for 12 days) and prednisolone b (1 mg/kg PO q12h for 7 days and q24h for 5 days) was prescribed, but there was no response. The fatty tissue surrounding the pericardium enlarged from July to the end of August, which suggested a neoplastic disease. After clinical signs worsened, resulting in the thorax being drained every other day, an exploratory thoracotomy was performed. A uniform mass was seen surrounding the pericardium, containing large blood vessels and black spots. The well-circumscribed and apparently encapsulated mass was not adhered to the surrounding tissues. No apparent mediastinal lymph node enlargement or other gross lesions were detected. The anomalous tissue was completely removed and submitted for histopathological examination. The dog recovered well from anesthesia but the clinical condition worsened and the dog died 5 days after surgery.
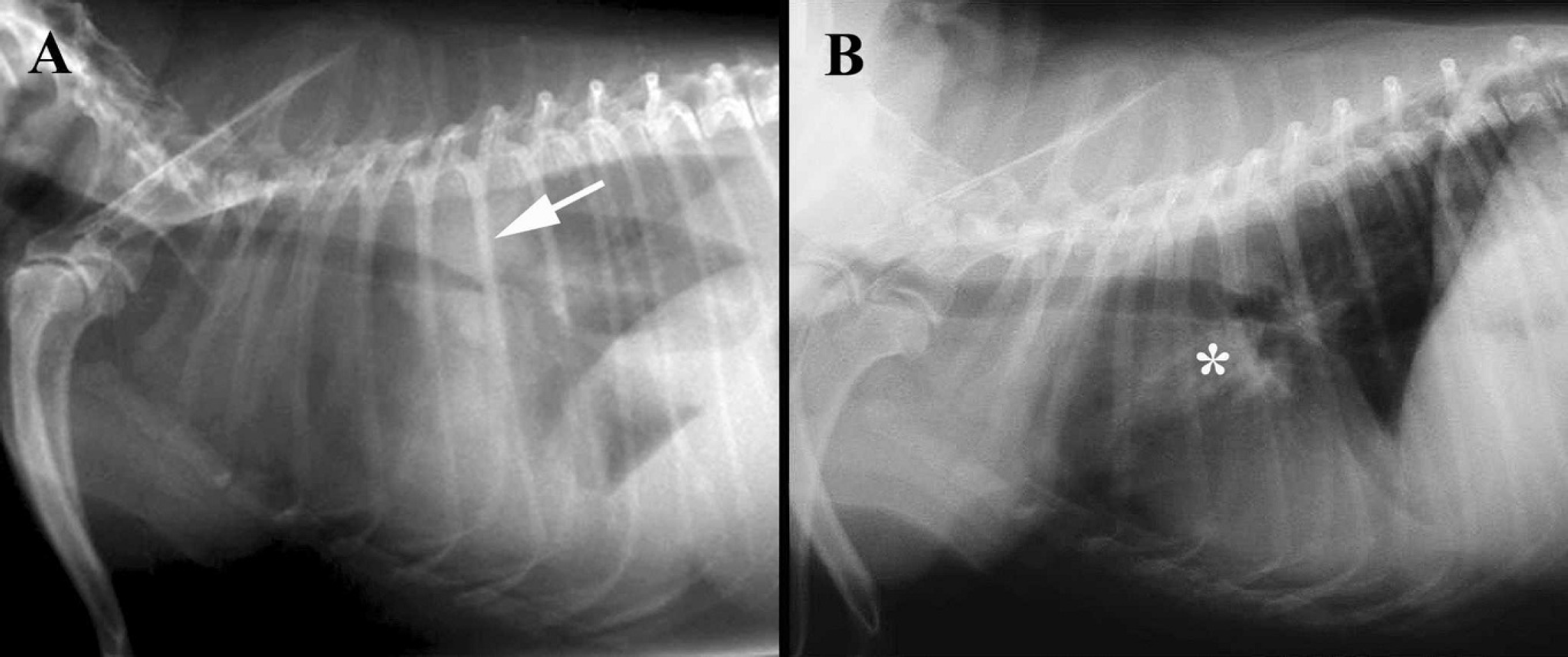
Lateral radiographic projections, thorax.
Grossly, the mass measured approximately 1.8 × 3.6 cm long and 1 cm thick, and was confined in a thin fibrous capsule. On cut section, the mass was homogeneous, soft, yellow to tan, and divided into lobules by thin trabecula; it somewhat resembled mature adipose tissue. Tissue samples were routinely processed, sectioned, and stained for light microscopy.
Microscopic examination revealed a well-defined encapsulated mass composed of multiple lobules and consisting of thymic tissue (approximately 40% of the tumor) and mature adipose tissue (60%). Both components could be clearly recognized (Fig. 3). Thymic tissue consisted of the typical mixed epithelial/lymphocytic cellular population with numerous Hassall's corpuscles. The lymphoid component contained numerous tightly packed small mature lymphocytes without corticomedullary arrangement (Fig. 3). Germinal centers were not observed. Some areas contained numerous Hassall's corpuscles or showed marked epithelial proliferation composed of polygonal cells displaying acidophilic cytoplasm, oval nuclei, and prominent nucleoli arranged in nests or a tubular pattern. Cystic degeneration of epithelial corpuscles was quite prominent throughout the tumor. Cysts were filled with proteinaceous material and lined by a single layer of squamous or ciliated cuboidal-to-columnar cells (Fig. 4). Some islands of thymic tissue were connected by cordlike strands of lymphocytes. Well-differentiated mature adipose tissue surrounded the islands of thymic tissue and was arranged in lobules separated by fibrous septa (Fig. 3). Hemorrhage and necrosis were not observed, but numerous hemosiderin-laden macrophages were seen scattered in the thymic component of the neoplasia (Fig. 3). The lesion was diagnosed as thymolipoma by the presence of a mixture of thymic and mature adipose tissue in a pericardial–mediastinal mass at microscopic evaluation.
Thymolipoma is a very rare, slow-growing, benign, human neoplasm of the thymus that occurs at any age and without sex predilection. 6,7 It represents 2–9% of all human thymic neoplasms. 7 The pathogenesis of this lesion is uncertain. Its peculiar composition has given rise to different theories about its origin. It has been proposed to represent hyperplasia of mediastinal fatty and thymic elements, true mixed neoplasia of both endodermal (thymic tissue) and mesodermal (adipose tissue) components, fatty neoplasia or hyperplasia that incidentally engulfs a normal thymic remnant, fatty degeneration of a hyperplastic thymus, abnormal hyperplasia of fatty tissue with subsequent involution of the normal thymic elements, or true thymomas undergoing fatty change in a similar manner to fatty replacement of the normal aging thymus. 6–8,10
In case presented here, the thymolipomas could be a variant of a thymoma undergoing fatty change. Gradations of epithelial proliferation and microscopic cysts filled with pink proteinaceous material were noted in this case and are frequently observed in thymomas of domestic animals. 5,9 These cysts are branchial duct remnants, have a lining that varies from squamous to columnar and ciliated, and can change abruptly from one to the other. 9 Cystic degeneration of Hassall's corpuscles is reported quite often in human thymolipoma. 6 Also, the typical corticomedullary anatomy can be absent in thymomas of domestic animals, 5,9 as in this case. The tumor reported in this study shares many characteristics with thymomas in domestic animals, suggesting a possible common origin for both.
Histological evidence of malignancy or malignant transformation has never been described in thymolipomas. 7 Because of the lack of malignancy, the importance of histopathology for thymolipomas lies in its differentiation from other thymic lesions. Thymic involution with fatty replacement was not considered for this mass because of evidence of proliferation and growth of the mass. Proliferative or neoplastic thymic lesions in dogs include lymphoma, thymoma, thymic hyperplasia, and thymic cyst formation. 2,9 In this study, no epithelial or lymphoid neoplasia were seen. Normal corticomedullary arrangement is retained in thymic hyperplasia, 2,8,9 as opposed to the tumor described in this study, in which this feature was lost. Cyst formation was apparent, but always in association with epithelial proliferation. For these reasons, the tumor described here best fits a diagnosis of thymolipoma. Additionally, mediastinal or thymic lipoma, a rarely reported tumor in humans and dogs, should be considered. 4,11 However, the theory that these lesions might represent lipomas of the thymus is not well accepted because the total quantity of thymic tissue usually exceeds the weight of a normal thymus. 7 In addition, mediastinal lipomas are not expected to contain thymic epithelial elements as an integral component.
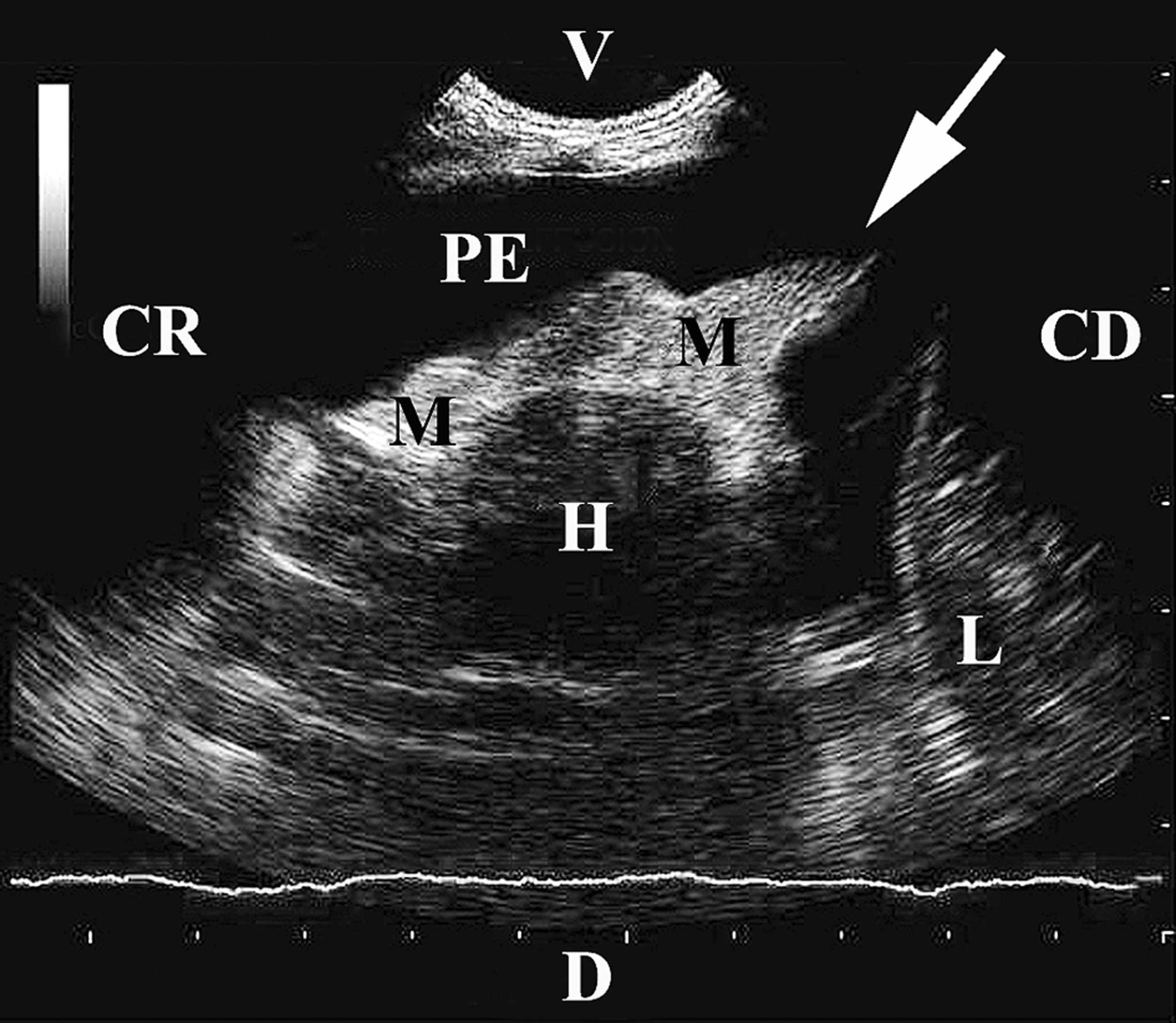
Ultrasound image, thorax. A hyperechoic, fibrous/fat echotexture mass is seen attached and surrounding the cranial/right side of the pericardium and is partly floating in the anechoic pleural effusion (arrow). CD = caudal; CR = cranial; D = dorsal; H = heart; L = liver; M = mass; PE = pleural effusion; V = ventral.
Most thymolipomas in humans are entirely asymptomatic. However in some cases, signs related to the presence of a space-occupying mass within the anterior mediastinum, such as cough, dyspnea, tachypnea, and chest or neck pain, are seen. 6,7,10 They are rarely associated with systemic disease (myasthenia gravis, aplastic anemia). 6–8 A single case of thymolipoma in the veterinary literature was reported in an adult cat. 10 Clinical signs in the cat were anorexia, lethargy, vomiting, dyspnea, mild anemia, and chylous pleural effusion. Although thoracic effusion has not been reported in humans with thymolipoma, 6,7 it seems to be a feature of thymolipoma in domestic animals. Effusion could result from increased thoracic duct pressure, secondary to compression of the cranial vena cava or thoracic duct by the thymolipoma, as suggested for mediastinal lymphoma and thymoma. 1–3,5,12
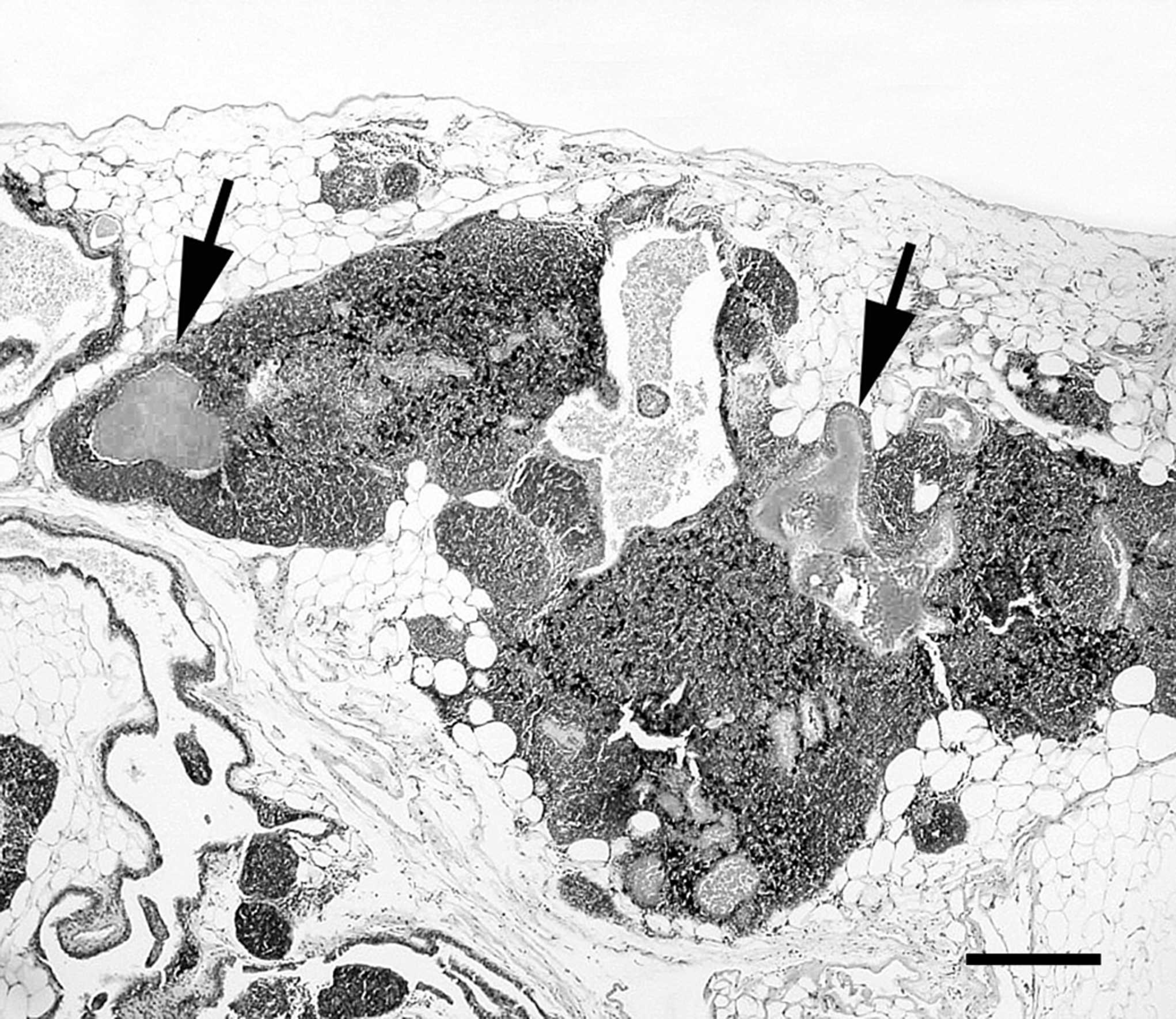
Light microscopy, mediastinal mass. The mass is well defined and composed of thymic tissue with numerous fluid-filled cysts (arrows) and lobules of mature adipose tissue separated by fibrous septa. Hematoxylin and eosin. Bar = 200 μm.
The mediastinal location of most thymolipomas, the soft and malleable nature of these lesions, and the semisolid consistency of fat at body temperature contribute to the ability of these tumors to conform to the shape of adjacent mediastinal structures. These properties might cause the mass to resemble cardiomegaly on frontal chest radiographs. 7 Ultrasounds, CT scans, and magnetic resonance images minimize the complications and substantially improve the diagnosis of this tumor in humans 7 and for other mediastinal masses in canine and feline species. 12 Ultrasonography and radiology showed that the echotexture and opacity of the tissue was prevalently compatible with adipose tissue. It was also possible to differentiate between the neoplastic tissue and the heart. Thus, ultrasounds and postdrainage radiographs appeared to be highly useful diagnostic tools to detect mediastinal masses with fatty or soft tissue appearance, such as thymolipoma, in animals with idiopathic thoracic effusions. However, definitive diagnosis could only be obtained on the basis of observation of thymic tissue included in mature fat tissue by histopathological examination. This report is the first description, to the authors' knowledge, of thymolipoma in a dog and should be included in the group of thymic neoplasms in small domestic animals.
Acknowledgements. The authors thank referring clinicians for providing additional clinical history. Histotechnicians at the HISTOVET Laboratory (Barcelona, Spain) are acknowledged for their technical assistance.
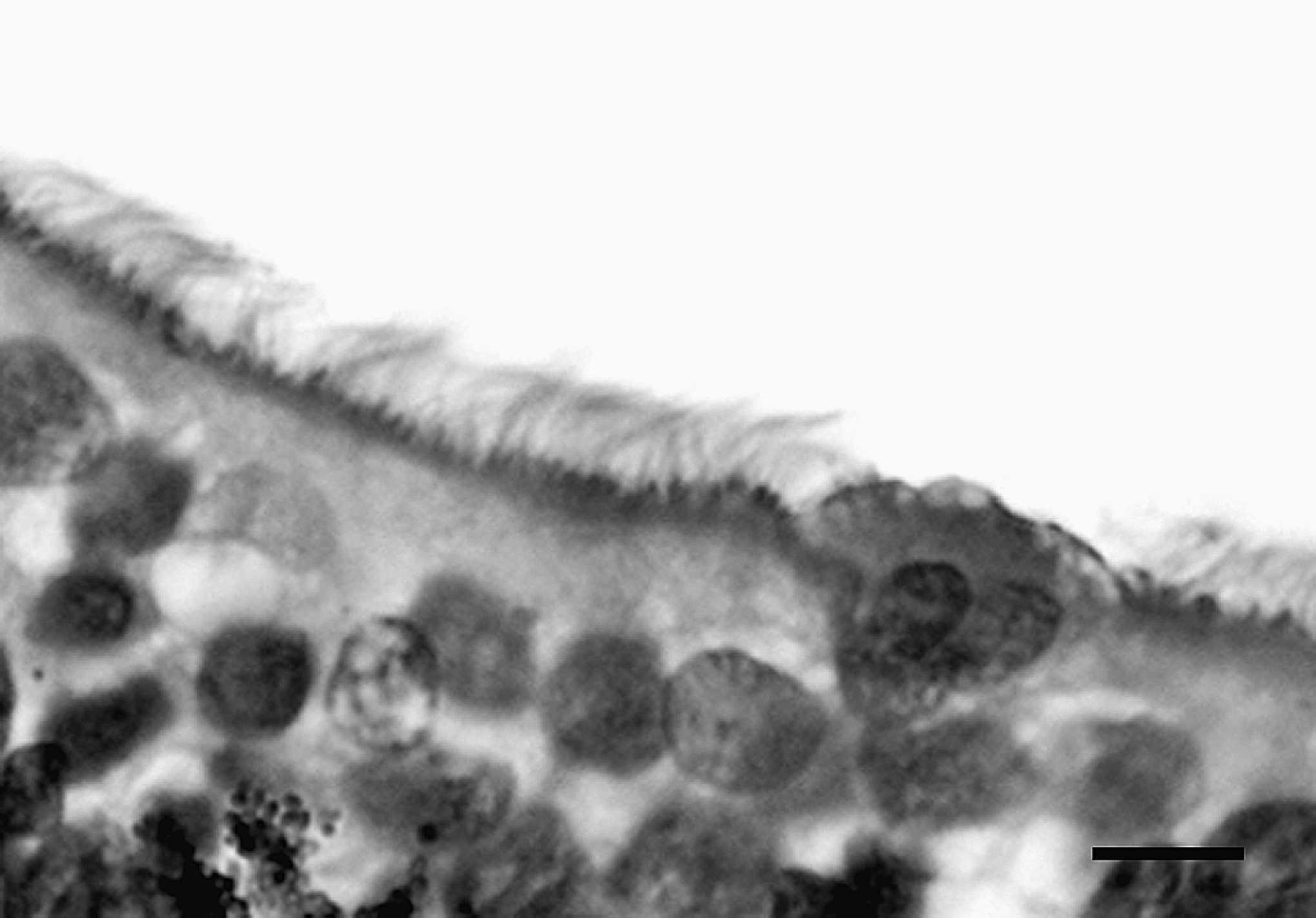
Light microscopy, thymic mass. A cyst in the mass is lined by a single layer of ciliated cuboidal epithelial cells. Hematoxylin and eosin. Bar = 10 μm.
Footnotes
a.
Synulox, Pfizer Italia srl, Rome, Italy.
b.
Vetsolone® compress, Bayer SpA, Milan, Italy.