
Abstract
A subcutaneous mass removed from the right rear leg of a 17-year-old, spayed, female Domestic Shorthair cat was characterized histopathologically by granulomatous inflammation, sheets of large atypical lymphoid cells, and necrosis. The walls of the small and medium caliber blood vessels were invaded transmurally by atypical lymphoid cells. A diagnosis of angioinvasive lymphoma (AIL), or lymphomatoid granulomatosis, was made based on histopathologic findings. The cat was euthanized 2 months later because of recurrence of the mass and elevated serum alanine aminotransferase activity, and a necropsy was performed. The histopathologic lesion of AIL was seen in the skin and subcutis of the right rear leg, and neoplastic cell infiltrates were seen in adjacent skeletal muscle, right superficial inguinal lymph node, liver, and spleen. By immunohistochemistry, variable numbers of neoplastic cells expressed B-lymphocyte antigen 36 (BLA36) or cluster of differentiation (CD)3 markers, indicative of B- and T-cell lineages, respectively. Neoplastic cells were uniformly positive for vimentin and uniformly negative for cytokeratins and myeloid/histiocytic antigen. Although the cat had received a Rabies virus vaccine subcutaneously in the right rear leg 6 months earlier, the AIL lesion was not typical of vaccine-induced sarcomas. The AIL in this cat was unusual because the extrapulmonary metastases involved the skin and subcutis.
Angioinvasive lymphoma (AIL), often referred to as lymphomatoid granulomatosis, 22 is a rare lymphoproliferative disease that primarily affects the lung. Features of AIL include a polymorphous lymphoid infiltrate, transmural invasion of blood vessel walls by atypical lymphoid cells, angiodestruction, and necrosis. 22 The pathogenesis of AIL is unclear, but the data suggest that AIL in humans has an inflammatory component, 8 and cytotoxic T cells may play a role in pathogenesis. 16 The data also suggest that most cases of the human disease are analogous to T-cell-rich B-cell lymphomas, 14 and the clonal proliferation of B cells is often associated with Human herpesvirus 4 (also known as Epstein-Barr virus [EBV]) infection. 6,15,17 Primary pulmonary AIL has been reported in humans, dogs, and 1 cat, 2,5,9–12,21 and metastatic disease subsequent to pulmonary AIL has been reported in humans and dogs. 5,9 Although rare, AIL involving the skin and subcutis has been reported in humans and dogs, 1,19 with adjacent skeletal musculature infiltration occurring in 1 dog. 19 The current report describes the histopathologic and immunohistochemical findings in a case of extrapulmonary metastatic AIL involving the skin and subcutis in a cat.
A formalin-fixed, cylindrical, subcutaneous mass measuring 9 cm × 2.5 cm × 1 cm removed surgically from the right lateral femoral region of a 17-year-old, spayed, female Domestic Shorthair cat was submitted for histopathologic examination. The cat had received a Rabies virus vaccine subcutaneously at this site 6 months earlier, and it had been examined 1 month earlier for an unrelated problem; the mass was not palpable at that time. Specimens from the mass were routinely processed for histopathology and sectioned at 4–5 μm. Sections were stained with hematoxylin and eosin, periodic acid–Schiff, Brown–Brenn Gram stain, and Fite acid-fast stain.
Histopathologically, unencapsulated sheets of densely packed, large, atypical lymphoid cells infiltrated the subcutis, and extensive foci of necrosis were present. Variably sized aggregates of epithelioid macrophages and moderate numbers of neutrophils, macrophages, lymphocytes, and plasma cells were mixed with the neoplastic cells. Neoplastic cells were pleomorphic and had large, vesicular, occasionally indented, euchromatic to hyperchromatic nuclei. Cell nuclei had 1–3 prominent or several indistinct nucleoli and coarsely clumped chromatin. Most cells had moderately abundant amphophilic cytoplasm, and occasional binucleated and multinucleated cells were seen (Fig. 1). Scattered cells had a plasmacytoid appearance characterized by amphophilic to basophilic cytoplasm and pale staining Golgi areas. Neo-plastic cells were divided into small packets by a fine fibrous or fibrovascular stroma, and there were 3–7 occasionally bizarre mitotic figures per 400 × field. Angiocentric cuffs of neoplastic cells were prominent, and the walls of small and medium caliber blood vessels were infiltrated transmurally by these cells (Fig. 2). Additional findings included whorl-like foci of fibrosis and neovascularization, blood vessels with recanalized fibrin thrombi, and fibrinoid necrosis of blood vessel walls. Special stains for bacterial and fungal organisms were negative. A diagnosis of AIL was made based on histopathologic findings.
The cat was examined 2 months later because of lethargy and recurrence of the mass. Radiographic examination of the thorax revealed no abnormalities, and hematologic values were within reference intervals. A serum chemistry profile indicated elevated (225 IU) alanine aminotransferase activity, and the owner elected euthanasia. The body was icteric at necropsy, and the recurrent mass (3 cm × 2 cm × 2 cm) had invaded the adjacent skeletal musculature. The right superficial inguinal lymph node was enlarged (3 cm × 2 cm × 1.5 cm), and surfaces of the liver and spleen had multiple, oval, raised, red–tan foci that were 5–8 mm in diameter. Skin, subcutis, and skeletal muscle from the surgical site and right superficial inguinal lymph node were immersed in 10% neutral buffered formalin and processed for routine histopathology. Additional specimens processed for histopathology included brain, lung, tracheobronchial lymph nodes, heart, liver, spleen, stomach, pancreas, kidneys, adrenal glands, small intestine, mesenteric lymph nodes, and colon. Bone marrow was not sampled.
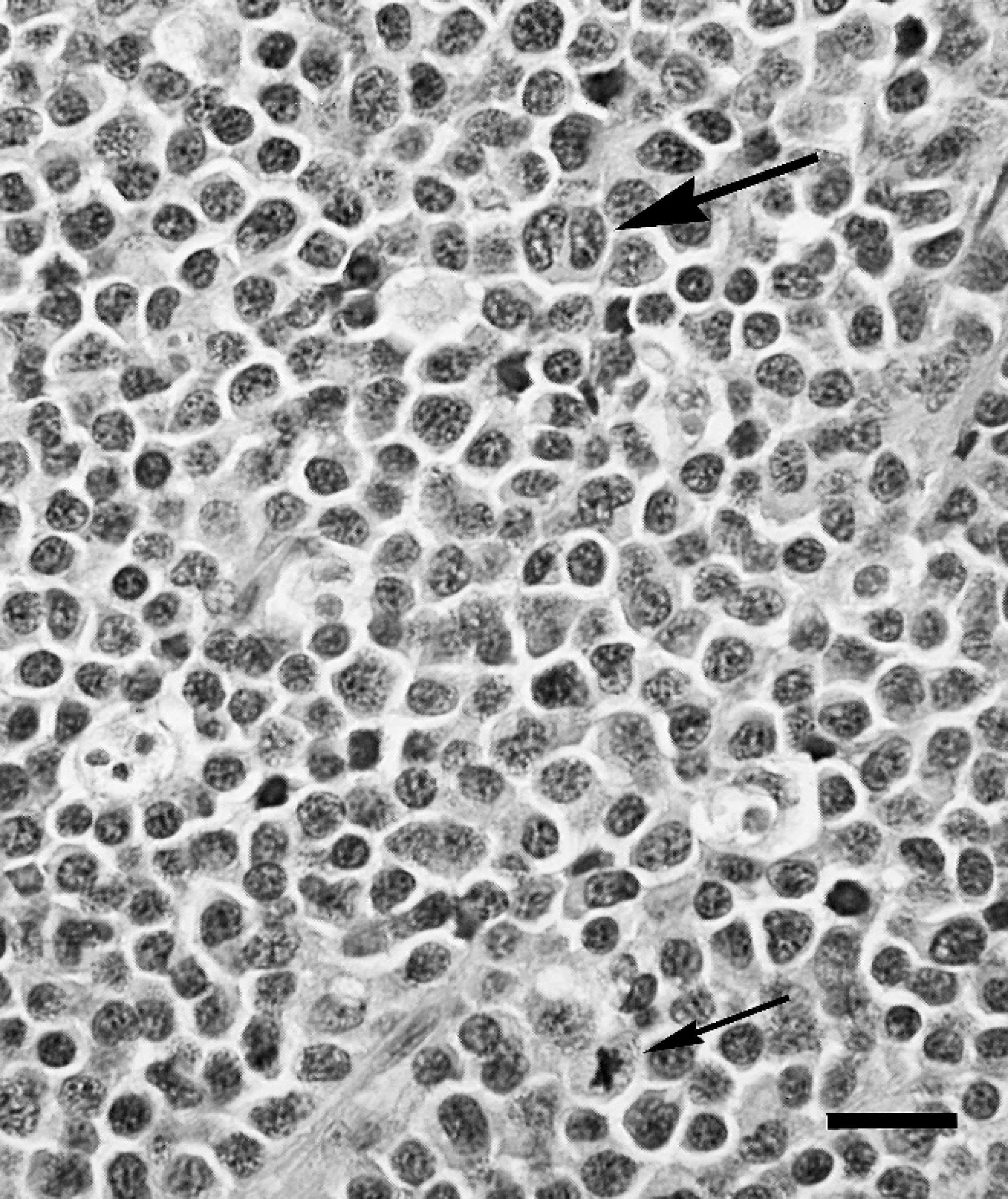
Subcutis; cat. Densely packed neoplastic cells are pleomorphic with large vesicular nuclei and moderately abundant cytoplasm; scattered cells have prominent nucleoli. Note multi-nucleated cell (large arrow) and mitotic figure (small arrow). Hematoxylin and eosin. Bar = 20 μm.
The histopathologic lesion in skin and subcutis from the surgical site was identical to that described previously. Occasional periadnexal cuffs of neoplastic cells were seen in the skin, but there was no epidermotropism. Skeletal muscle bundles, architecture of the right superficial inguinal lymph node, and red pulp of the spleen were effaced by sheets of neoplastic cells. Foci of necrosis, neoplastic cell infiltrates within attenuated sinusoids, bile stasis, and lipidosis were seen in sections of liver. There were no histologic lesions in the other specimens collected at necropsy.
For immunohistochemistry (IHC), formalin-fixed, paraffin-embedded tissue sections were stained with antibodies to B-lymphocyte antigen 36 (BLA36), cluster of differentiation 3 (CD3), myeloid/histiocytic antigen, cytokeratins, and vimentin (Table 1). BLA36 and CD3 markers in each tissue section were assayed with a double-labeling technique using horseradish peroxidase and alkaline phosphatase visualization systems according to the manufacturer's instructions. a The other markers were assayed with a labeled streptavidin–biotin–alkaline phosphatase visualization system. b Fast-red c was used as the substrate-chromogen in alkaline phosphatase-based visualization procedures, and all sections were counterstained with Mayer hematoxylin. Formalin-fixed, paraffin-embedded tissues with the antigen of interest were stained in parallel and served as positive controls. Nonimmune murine ascites fluid or rabbit serum served as negative controls.
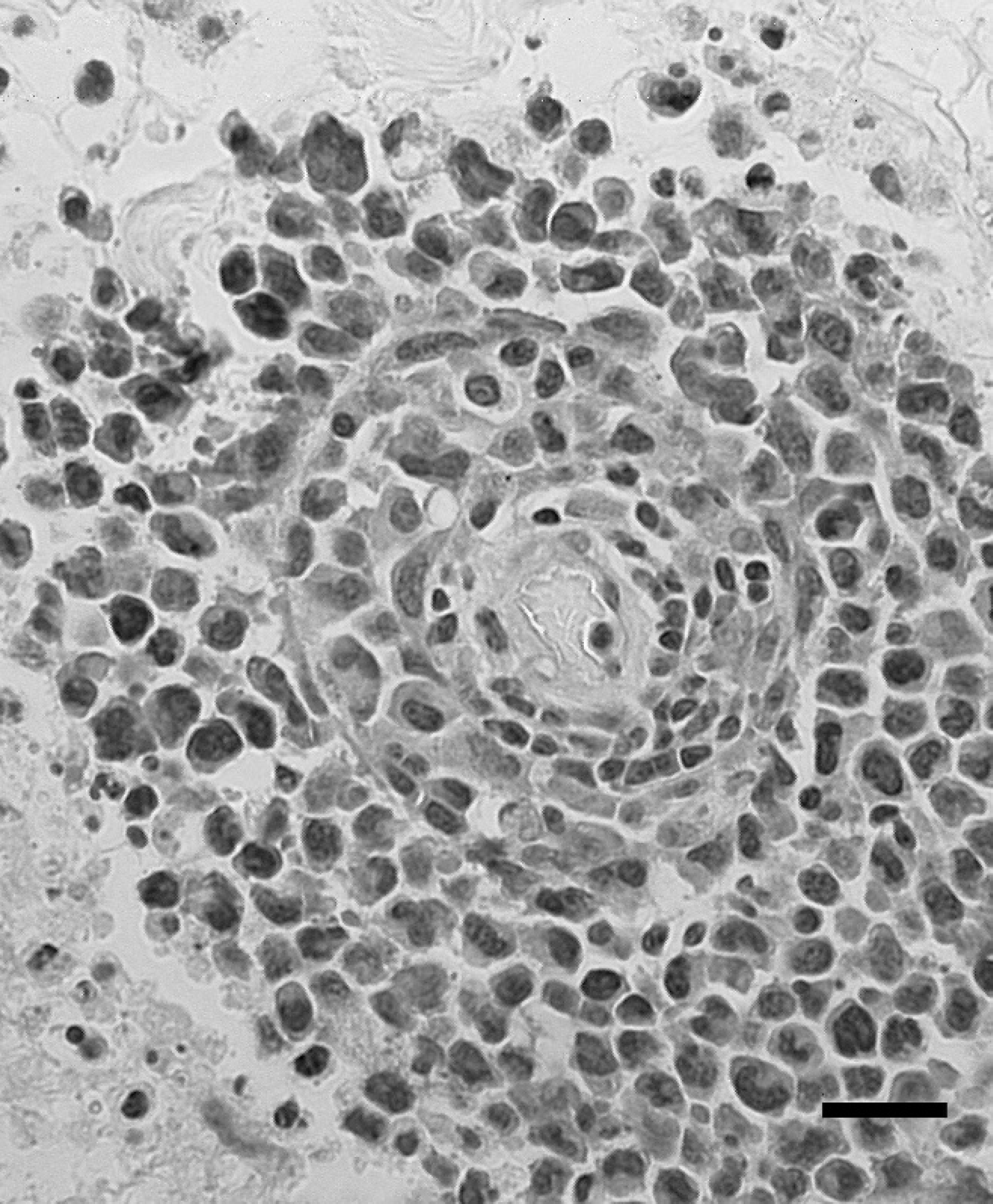
Subcutis; cat. A blood vessel is surrounded by neoplastic cells, and the vessel wall has been infiltrated transmurally by neoplastic cells. Hematoxylin and eosin. Bar = 20 μm.
By IHC, variable numbers of neoplastic cells in the skin and subcutis expressed BLA36 or CD3 markers (Fig. 3). Approximately 20–50% of neoplastic cells in each tissue section expressed one or the other marker, and positive staining for these markers was prominent around blood vessels. Neoplastic cells in blood vessel walls expressed BLA36 or CD3 (Fig. 4) markers or neither marker. A majority of small lymphocytes interspersed amongst neo-plastic cells were positive for BLA36 or CD3 markers, and epithelioid macrophages, macrophages, and neutrophils were consistently positive for myeloid/histiocytic antigen. Variable but generally small numbers of neoplastic cells in skeletal muscle, right superficial inguinal lymph node, liver, and spleen stained positively for BLA36 or CD3 markers. The neoplastic cells were uniformly positive for vimentin, indicative of mesenchymal origin, and uniformly negative for cytokeratins and myeloid/histiocytic antigen.
The histopathologic lesion in the skin and subcutis of the cat in the current study was consistent with AIL, a rare disease often referred to as lymphomatoid granulomatosis. 22 Cutaneous AIL in humans and dogs is characterized by erythematous plaques or nodules, with or without subcutaneous nodules, and with or without ulceration. 1,19 Although the AIL lesion was present in the initial biopsy from the cat in the present study, biopsies of skin and/or subcutis taken early in the disease may appear as inflammatory lesions, and a series of biopsies may be necessary to detect the AIL lesion. 19 Primary pulmonary AIL has been reported in humans, dogs, and 1 cat, 2,5,9–12,21 but lung lesions were not seen in the cat in the present study. Based on clinical history and pathologic findings, tissues of the right rear leg were believed to be the primary sites of AIL in the cat in the present study. Although the cat had received a Rabies virus vaccine subcutaneously in the right rear leg 6 months earlier, the AIL lesion was not typical of vaccine-induced sarcomas. 3,4,7 However, vaccine-induced sarcomas and AIL have inflammatory components that may play a role in malignant transformation, 8,13 and the possibility that AIL in this cat developed secondarily to vaccination could not be excluded.
The immunophenotypic findings indicated that AIL in the cat in the current study was of both B- and T-cell lineages, and these findings correlated with those reported for 1 case of canine pulmonary AIL 18 and for other types of canine lymphoma. 20,23,24 These findings were in contrast to human AIL, where most cases have been classified as T-cell-rich B-cell lymphomas. 14 The present study did not investigate B- and T-cell clonality, and clonality studies would be necessary to more fully characterize feline AIL.
Antibodies and methods used for immunohistochemical analysis of angioinvasive lymphoma in a cat.*
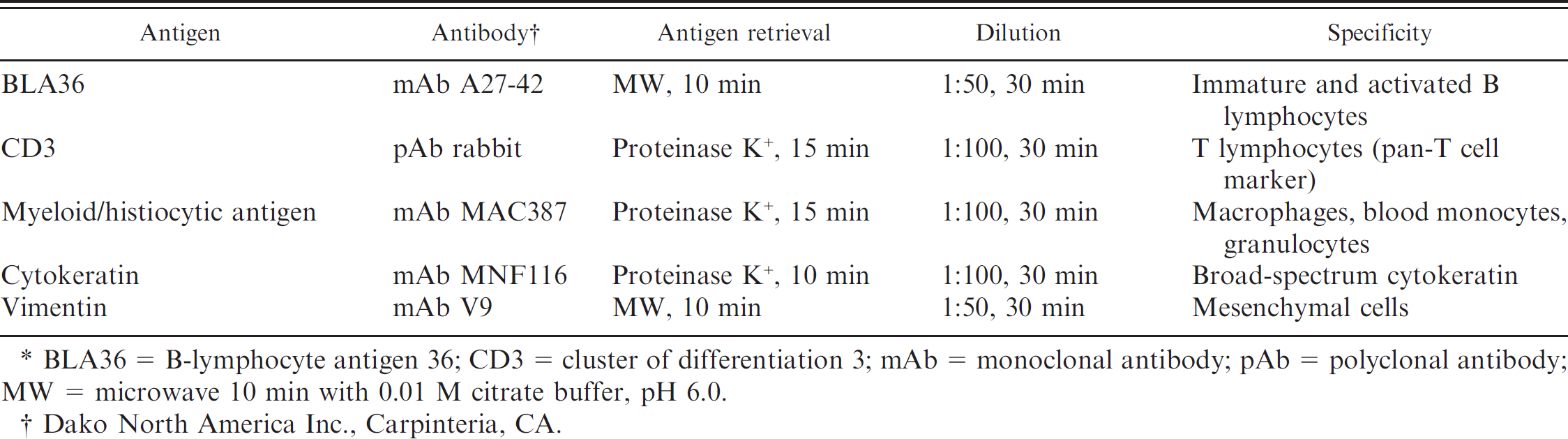
BLA36 5 B-lymphocyte antigen 36; CD3 = cluster of differentiation 3; mAb MW = monoclonal antibody; pAb = polyclonal antibody; MW = microwave 10 min with 0.01 M citrate buffer, pH 6.0.
Dako North America Inc., Carpinteria, CA.
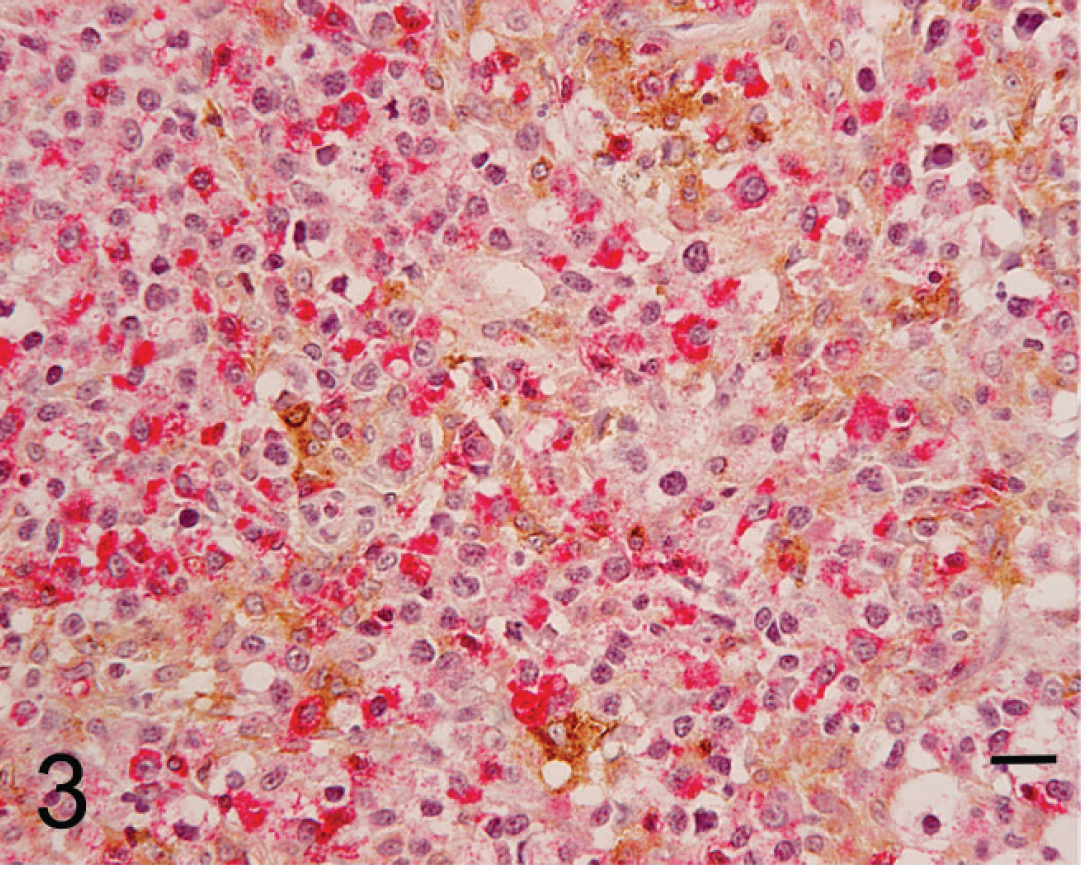
Subcutis; cat. Neoplastic cells stain positively for B-lymphocyte antigen 36 (BLA36; brown precipitate) or cluster of differentiation 3 (CD3; red precipitate) markers, which are indicative of B- and T-cell lineages, respectively. Double-labeling immunohistochemistry using horseradish peroxidase and alkaline phosphatase visualization systems. Mayer hematoxylin counterstain. Bar = 20 μm.

Subcutis; cat. A blood vessel is surrounded by small numbers of cluster of differentiation 3 (CD3)-positive neoplastic cells, and the vessel wall has been infiltrated transmurally by a uniform population of CD3-positive neoplastic cells. The arrow denotes the narrow lumen of the blood vessel. Double-labeling immunohistochemistry using horseradish peroxidase and alkaline phosphatase visualization systems. Mayer hematoxylin counterstain. Bar = 20 μm.
Many cases of human AIL are believed to be caused by neoplastic transformation of B cells by EBV infection. 6,15,17 Whether or not lymphoma-associated viruses, such as Feline leukemia virus (FeLV) and Feline immunodeficiency virus (FIV), play a role in AIL remains to be determined. The cat in the present study was housed indoors and had been routinely vaccinated for FeLV but not for FIV. The present report is unique in describing extrapulmonary metastatic AIL involving the skin and subcutis in a cat. Although rare, AIL should be considered as a differential diagnosis for cutaneous and subcutaneous lesions in cats, and affected cats should be evaluated for evidence of metastasis.
Footnotes
a.
Dako EnVision™ Doublestain System, Dako North America Inc., Carpinteria, CA.
b.
Dako LSAB™2 System-AP, Dako North America Inc., Carpinteria, CA.
c.
Bio-Red Fast Red, Biopath Laboratories Inc., Oklahoma City, OK.