
Abstract
Lymphomatoid granulomatosis (LYG) is a rare variant of an angioinvasive T-cell lymphoproliferative disorder that primarily affects the lungs, with common sites of metastasis including the skin and subcutis. In humans, it is a B-cell lymphoproliferative disorder associated with Epstein-Barr virus infection. Our case is a 7-y-old, spayed female, domestic longhair cat that decompensated and was euthanized following an initial diagnosis of angioinvasive lymphoma from a skin biopsy. Autopsy revealed nodules in the lungs and subcutis, and corneal thickening and cloudiness. Histologic examination of cutaneous nodules, lungs, and eye showed similar angioinvasive cellular infiltrates and pattern to that of the original skin biopsy, consistent with a diagnosis of LYG. The neoplastic cells displayed CD3-positive immunoreactivity in the skin, eye, and lung, and PCR for antigen receptor rearrangement (PARR) showed T-cell clonality in all tissues tested. This is the third case of LYG to be reported in cats and is the only case in which PARR analysis and immunophenotyping immunohistochemical staining was performed. LYG with ocular involvement has not been reported previously in cats, to our knowledge. Our case demonstrates the necessity for considering LYG when presented with a cat with respiratory signs in conjunction with subcutaneous nodules and ocular lesions.
Lymphoma has been reported in all domestic species and encompasses a wide variety of malignancies. In cats, lymphoma has been historically associated with feline leukemia virus (FeLV) infection resulting in a mediastinal or multicentric T-cell lymphoproliferative disorder. 13 In contrast, feline immunodeficiency virus (FIV)-associated tumors are generally high-grade B-cell lymphomas. Lymphomatoid granulomatosis (LYG) is an extremely rare variant of lymphoma reported in humans and dogs, and has only been reported twice in cats, to our knowledge.7,12,13
In humans, LYG is a rare, angiocentric, and angioinvasive B-cell lymphoproliferative disorder associated with Epstein-Barr virus (EBV; Human gammaherpesvirus 4) infection of B lymphocytes in conjunction with dysregulated immune surveillance of EBV resulting in a large population of recruited reactive T cells. All patients have lung involvement, with other sites variably involved. An established grading scheme divides cases into grades 1–3, with a greater degree of necrosis in EBV-infected cells in higher grades.8,9
LYG has been described rarely in dogs and cats. Histologic findings include a necrotizing angiocentric and angioinvasive process involving small lymphocytes, plasma cells, histiocytes, and atypical lymphoreticular cells, primarily in the lung, although other sites have been reported.2,3,10,13 In canine cases in which immunophenotypic characterization was documented, the infiltrating lymphocytic population appeared mixed with combinations of CD3, CD20, and CD79 positivity.3,6 Immunophenotypic characterization was only defined in one of the previously reported feline cases in which, again, a mixed population was reported with BLA36 and CD3 positivity suggestive of B and T cell, respectively.7,12 Dogs often develop eosinophilia, lymphocytosis, and hyperglobulinemia.1,2,4 In cats, reported sites include lungs, liver, spleen, skin, and subcutis, with clinical signs and aberrations in biochemical parameters related to the affected organ. The disease in cats carries a grave prognosis, with reported survival times of ~2 mo from time of diagnosis.7,12
A 7-y-old, spayed female, domestic longhair cat started losing weight, and had a hard lump noted on the right side of the neck that had enlarged progressively, and another lump starting to appear on the top of the right shoulder. The cat became febrile and was first treated with antibiotics, to which the nodules remained unresponsive. On re-examination, the cat had generalized lymphadenopathy, corneal edema of the left eye, and multiple irregularly thickened subcutaneous nodules on the entire body. A biopsy of the subcutaneous nodule was submitted for histologic evaluation; a diagnosis of angiocentric and angioinvasive lymphoma was made. Following treatment with steroids, the subcutaneous nodules regressed moderately in size, but the cat developed diarrhea, dyspnea, and became febrile. The lesion in the left eye remained unresponsive to the steroid treatment, and the clinical signs worsened with marked respiratory distress. Euthanasia was elected given the progressive clinical signs.
On autopsy, subcutaneous masses of 2–4 cm diameter were found on the right shoulder, right distal antebrachium, and the left distal antebrachium. The left eye had diffuse corneal edema and hypopyon (Fig. 1A). The lungs were firm, heavy, and contained multifocal-to-coalescing, tan-white nodules of 1–25 mm diameter throughout the parenchyma of all lung lobes (Fig. 1B); the nodules extended deep into the parenchyma on cut section. Multiple tissues were submitted for histologic examination. The microscopic lesions were identified in the lung, skin, and left eye only. Both the initial skin biopsy (data not shown) and multiple skin nodules collected during autopsy had deep dermal to subcutaneous infiltrates of sheets and aggregates of round cells with frequent perivascular infiltration (angiocentric) and occasional vascular mural invasion (angioinvasive; Fig. 1C, 1D). The neoplastic cells had distinct borders with scant eosinophilic cytoplasm. The nuclei were 1.5–2.5 times the diameter of erythrocytes, round-to-oval, with vesicular chromatin and had multiple prominent nucleoli. There was moderate-to-marked (1.5 to 2-fold) anisocytosis and anisokaryosis. Mitotic count was 32 in 2.37 mm2 (ten 400× fields). The lungs had multifocal-to-coalescing areas of sheets of round cells with large areas of necrosis that replaced the lung parenchyma. The round cells had morphology similar to the skin nodules, with occasional perivascular infiltration and a few vascular thrombi containing round cells (Fig. 2A). In addition, there were peribronchiolar infiltrates of pleomorphic round cells that formed thick perivascular cuffs. There were occasional bi- and multi-nucleate round cells, macrophages, and rare plasma cells (reactive) in the alveolar spaces. The cornea and anterior uvea of the left eye had marked infiltration of neoplastic round cells (similar to those found in the skin nodules) with frequent invasion of the walls of blood vessels within the cornea and ciliary body (Fig. 2B, C).
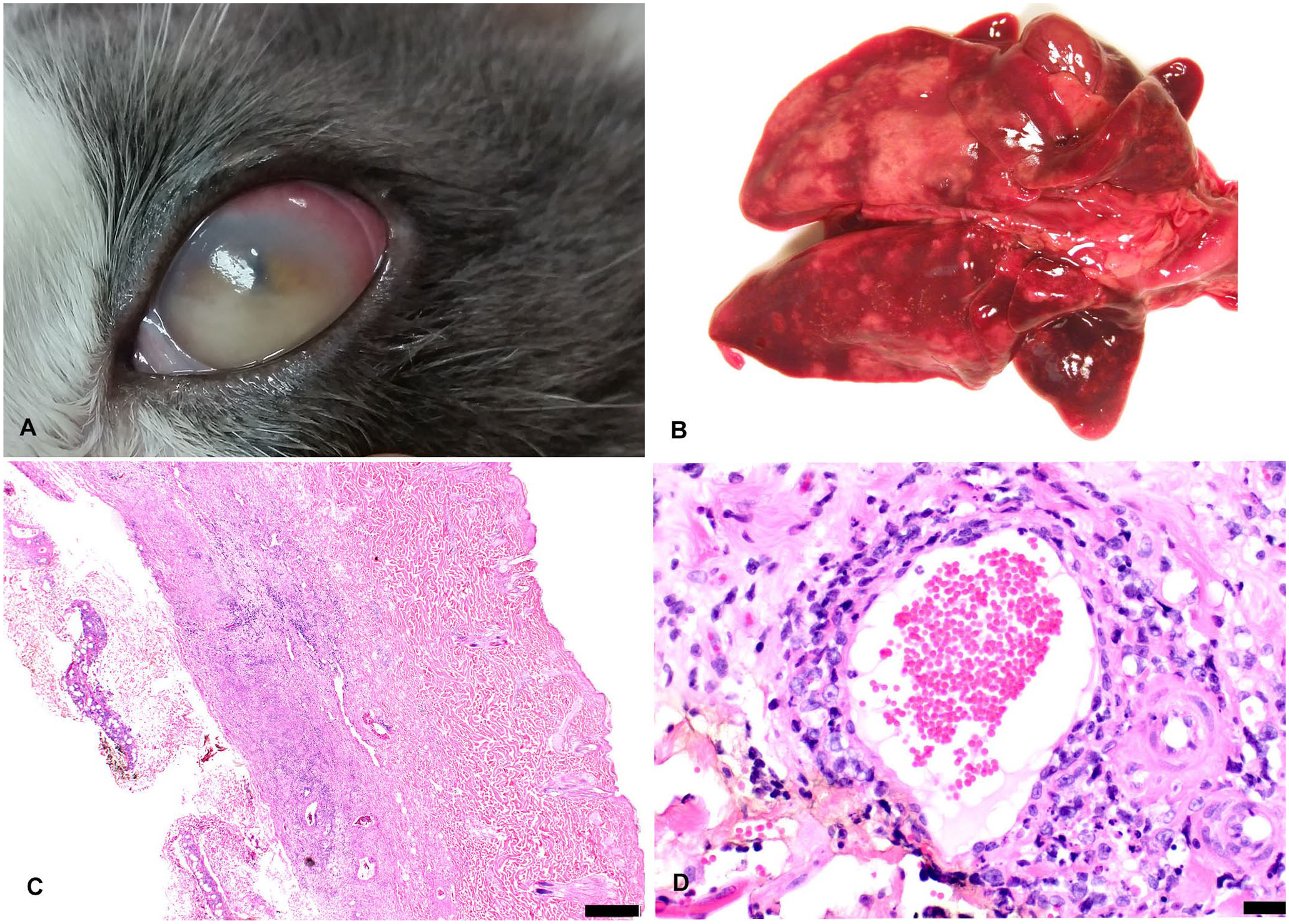
Angioinvasive lymphoma (lymphomatoid granulomatosis) affecting the eye, lung, and skin in a cat.
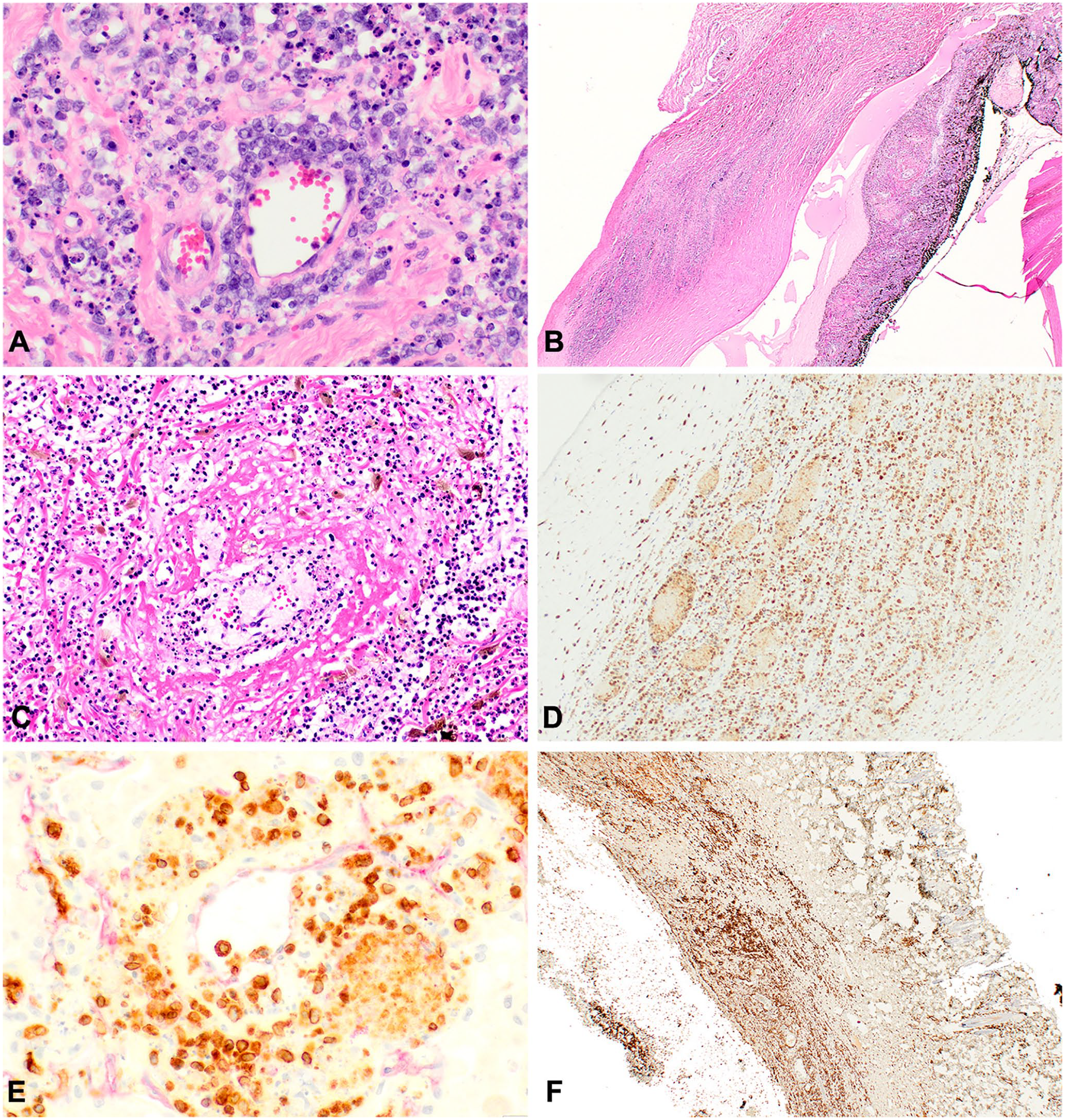
Histologic and immunohistochemical characteristics of lung, skin, and eye of a cat with lymphomatoid granulomatosis.
By immunohistochemistry (IHC), the neoplastic round cells were strongly immunoreactive (cytoplasmic and membranous) for CD3 (T-cell marker), and lacked immunoreactivity for CD20 (B-cell marker) and CD18 (histiocytic marker) in the sections of tissue taken from skin, lungs, and left eye (Fig. 2D–F). Dual immunohistochemical staining was performed with claudin-5 and CD3 to highlight the endothelial cells (claudin-5 marker) and show invasion of the vascular wall by CD3-positive staining neoplastic T-cell lymphocytes (Fig. 2E). PCR for antigen receptor rearrangement (PARR) analysis was performed at the University of California, Davis on sections from the skin, lung, and eye. The clonal rearrangement of the feline T-cell locus (TRG) matched exactly across all of the submitted samples, indicating that the cells were of the same neoplastic population. The gross, histopathologic, and IHC findings supported a diagnosis of angioinvasive, angiocentric T-cell lymphoma, described as LYG in the veterinary literature.
The angioinvasive-angiocentric nature of lymphoma seen in the lungs in our case is consistent with lymphomatoid granulomatosis, which is a rare lymphoproliferative disorder that was first reported in humans in 1972, and occasionally in dogs and only twice in cats.7,11 LYG in humans is an EBV-associated, angiocentric, and angioinvasive lymphoproliferative disease, composed of variable numbers of T cells and variable numbers of atypical clonal EBV-positive B cells in a polymorphous inflammatory background, which always involves the lung with subsequent skin, central nervous system, and renal involvement. 8 In dogs, the disease is characterized as a T-cell angiotropic lymphoma; however, a few reports have demonstrated a mixed population of small lymphocytes, plasma cells, histiocytes, and atypical lymphoreticular cells.1,3–6,10 Clinical signs vary extensively and are related to the organ systems involved.
LYG was first reported in a cat in 2000, and was characterized by gross and histologic lesions confined to the pulmonary parenchyma and tracheobronchial lymph nodes, but IHC results were inconclusive. 12 A report of LYG in a cat in 2009 described the presence of atypical lymphoid cells invading transmurally the small and medium caliber blood vessels of the skin, subcutis, superficial inguinal lymph node, liver, and spleen. By IHC, the infiltrative mononuclear cells were confirmed to be a mixture of B and T cells. 7 The histologic lesions in the lung, skin and other organs reported in these 2 previous studies are consistent with those found in our case. To our knowledge, LYG with typical pulmonary presentation and concurrent ocular and cutaneous lesions has not been reported previously, nor has PARR analysis been reported, which confirmed clonal rearrangement of the T-cell locus of neoplastic cells. The lymph nodes examined in our case showed no evidence of neoplasia. The histopathologic characteristics in lungs, skin, and eye with clear demonstration of the neoplastic T-cell lineage by IHC and clonal rearrangement of TRG locus is strongly supportive of T-cell angiotropic and angioinvasive lymphoma, consistent with LYG. Previous publications have described the utility of HLA-DR IHC in determination of cell lineage; however, given the strong positivity for CD3 and absolute lack of immunoreactivity for CD20 in conjunction with the PARR results, this was considered unnecessary in our case. 7 Unfortunately, the FeLV status of our case was not available, although its status as a T-cell lymphoma may suggest a viral component. In cats, further exploration in identifying a possible viral contribution to the disease process, as in the human correlate, may be warranted.
Lymphomatoid granulomatosis is a rare disease with correlates across humans, dogs, and cats, although initiating factors, cell lineages involved, and prognosis appears to vary across species. Our case shows that, in LYG, the neoplastic cells can also affect the eye along with other previously described locations, and that it is a variant of T-cell angioinvasive lymphoma, in contrast to its human counterpart. Although a rare disease, the differential diagnosis of LYG should be considered if histologic examination of skin, subcutaneous tissues, eye, or internal organs shows evidence of a proliferative lymphocyte population with vascular invasion. The differential diagnosis of LYG should also be considered by practitioners presented with a cat with subcutaneous nodules and concurrent respiratory distress that could be of infectious or neoplastic causes.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.