
Abstract
A 35-year-old horse was submitted to the necropsy service at the University of Kentucky Livestock Disease Diagnostic Center. At necropsy, multiple 1–4-cm-diameter cystic structures were incidentally identified unilaterally in the right renal medulla and the cortex. On histologic examination, the cystic structures compressed the normal renal architecture, were lined by tall columnar epithelium that formed occasional papillary projections, and contained large amounts of mucicarmine and periodic acid–Schiff-positive mucinous material. The masses were diagnosed as renal mucus-gland cystadenomas. This tumor should be considered as a differential diagnosis when cystic structures are identified in the equine kidney.
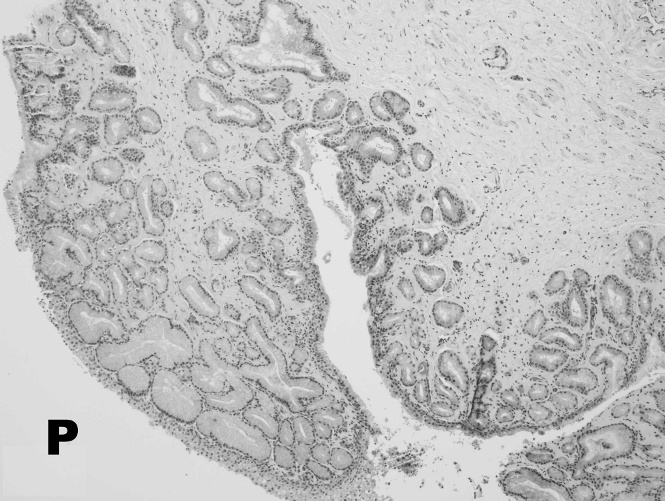
Normal pelvis renalis glands, equine. Mucus glands are located in the submucosa. The renal pelvis is evident (P). Hematoxylin and eosin stain. Total magnification = 40X.
The equine species is unique in that the renal pelvis and proximal ureter contain low numbers of mucus glands referred to as pelvis renalis and uretericae glands, respectively. 2,8 These simple branched tubuloalveolar glands are present in the mucosa and produce viscous mucinous material (Fig. 1). To the authors' knowledge, there has been only 1 previous report of a renal pelvic-gland adenoma described in the literature; this tumor was suggested to have arisen from the pelvis mucus glands. 5 The present article describes the pathologic changes associated with a unique case of multiple unilateral mucus-gland cystadenomas in a horse.
A 35-year-old female horse of unknown breed presented to the necropsy service at the University of Kentucky Livestock Disease Diagnostic Center with a brief history of slight neurologic deficit and hindquarter weakness. At necropsy, the horse was in thin body condition and fair-to-poor postmortem preservation. The normal medullary and cortical architecture of the right kidney was distorted by frequent 1–4 cm in diameter cystic structures that contained translucent, slightly viscous, yellow fluid. There were no blockages associated with the renal pelvis or the ureter. Lesions were not evident in the left kidney. The animal exhibited severe dental attrition of the upper arcade and had only 2 premolars remaining in the lower arcade. Small-to-moderate amounts of poorly to unmasticated plant material were located throughout the distal alimentary tract. Additional findings included a 0.5-cm-diameter cholesteatoma in the right lateral cerebral ventricle and variably sized metastatic melanomas within the spleen and multiple lymph nodes. Appropriate tissues were placed in phosphate buffered 10% formalin, allowed to fix for 24 hr, were routinely processed, and stained with Harris hematoxylin and eosin for microscopic evaluation. In addition, cytokeratin immunohistochemistry (mouse anti-human monoclonal, clone: AE1/AE3), a mucicarmine, and periodic acid–Schiff (PAS) stains were performed on the polycystic right kidney.
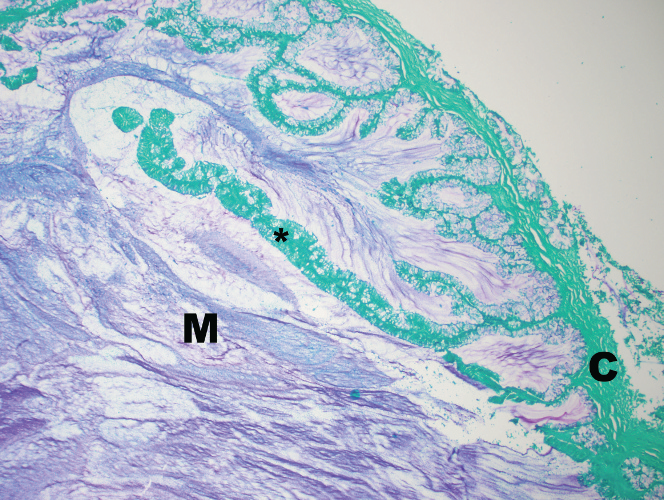
Mucus gland cystadenoma, equine. Basophilic mucinous material (M) fills the cystic mucus gland. A papillary projection of epithelial cells is evident (asterisk). A thin fibrous connective tissue capsule surrounds the mucus gland (C). Periodic acid–Schiff stain. Total magnification = 100X.
The cystic structures appeared histologically similar. The well-demarcated and thinly encapsulated cystic masses slightly compressed the normal renal architecture. The cysts were lined by tall, columnar, hyperplastic epithelial cells that occasionally formed papillary projections and were supported by a scant fibrovascular stroma (Fig. 2). The 5–7 × 15–20-μm columnar epithelial cells had distinct cell borders and large amounts of acidophilic cytoplasm, and contained a single basally located 4–6-μm nucleus that had finely clumped chromatin. Cellular atypia and mitotic figures were not evident. The cystic lumens contained large amounts of homogenous acidophilic material. Mucicarmine and PAS stains revealed large amounts of positively stained mucinous material within the cytoplasm of the neoplastic cells and within the cystic lumens. Neoplastic cells stained positive for cytokeratin.
Primary equine renal tumors are a rare occurrence and are most commonly identified as incidental lesions at necropsy. Equine renal-cell carcinomas and adenomas are most commonly reported, but undifferentiated sarcomas, transitional-cell carcinomas, embryomas, squamous-cell carcinomas, and nephroblastomas have also been described. 3,6,7,9 A previous study described the ultrasonographic and gross pathologic changes associated with a renal pelvic adenoma. 5 The authors suggested that the tumor arose from the pelvic mucus glands, but histopathologic descriptions were not provided.
The masses reported in the present study were incidentally discovered at necropsy and were diagnosed as multiple mucus-gland cystadenomas. It should be noted that this entity was hard to differentiate from mucus-gland hyperplasia. Although this differentiation may be arbitrary, mucus-gland cystadenoma was favored over hyperplasia based on the presence of a thin fibrous connective-tissue capsule, the expanding and compressive nature of the masses, multiple proliferative intraluminal papillary projections, and the presence of large mucus-filled cystic lumens.
Renal cysts are commonly observed in the kidneys of many species. Characteristics of renal cysts include a primarily cortical location, flattened or cuboidal epithelium, and the presence of watery fluid. 1,4 The tumors of the current report differed from renal cysts in that the cystadenomas were primarily medullary in location, lined with columnar epithelium that contained basally located nuclei, formed papillary projections, and contained intraluminal and intracytoplasmic PAS- and mucicarmine-positive mucous material.
A definitive cause of the neurologic deficit and hindquarter weakness was not determined. The spinal cord was not removed or examined, because owner authorization was not granted. Based on gross examination and histopathology, the primary differentials for the neurologic deficit included metastatic melanoma and generalized weakness because of dental attrition, maldigestion, and malabsorption.
These mucus-gland cystadenomas were an incidental finding at necropsy and may be related to the marked age of the animal. On histologic examination, but not gross examination, the masses were readily differentiated from renal cysts. The etiologic development and prognosis of this tumor is not currently known. Mucus-gland tumors should be considered as a differential diagnosis when cystic renal or ureteral masses are evident at necropsy.
Footnotes
a.
Dako North America Inc., Carpinteria, CA.