
Abstract
A 1.5-year-old castrated, male, mixed-breed dog was evaluated because of a 2-week history of lethargy, stiffness, and progressive paraparesis. Spinal radiographs, myelography, and computed tomography of the region showed a locally invasive mass involving the thoracic wall. Upon necropsy, an encapsulated, fluctuant mass was noted attached to the right dorsal body wall in the region of the fifth to seventh thoracic vertebra. Churukian-Schenk staining revealed positive granules within the neoplastic cell cytoplasm and immunohistochemistry was positive for expression for cytoplasmic neuron-specific enolase and synaptophysin. Chromogranin A and S100 expression were found to be negative. Immunohistochemistry and silver staining did not allow further differentiation of the tumor, and the diagnosis remains consistent with either a chromaffin paraganglioma or a nonchromaffin paraganglioma (chemodectoma) with some production of catecholamines. Extra-adrenal paragangliomas are rare neoplasms in dogs but should be considered as a possible differential diagnosis for a primary paraspinal thoracic mass.
Extra-adrenal paragangliomas include a diverse group of neuroendocrine tumors that may arise from multiple sites in the body. 6 Paraganglia are derived from the neural crest cells and arise in association with the autonomic nervous system throughout the body. The paraganglionic system is made up of the adrenal medulla, chemoreceptors, vagal body, and small groups of cells associated with the thoracic, intra-abdominal, and retroperitoneal ganglia. Paragangliomas are neoplasms that arise from any of the paraganglia. Based on the anatomic location, paraganglia neoplasms can be further classified into 3 groups: pheochromocytomas, extra-adrenal pheochromocytomas, and chemodectomas. Mediastinal paragangliomas can arise from the pulmonary artery and aortic arch or from any of the paraganglia located in the autonomic chain in the thoracic region. 10 Chemodectomas are the most common paragangliomas reported in the thoracic region; however, these neoplasms are generally classified using immunohistochemistry (IHC) based on the absence of chromaffin expression staining. The purpose of the current study was to describe the historical, physical, diagnostic, and immunohistochemical findings of a case of mediastinal extra-adrenal paraganglioma with spinal invasion that was not immunohistochemically consistent with a chemodectoma.
A 1.5-year-old, 23-kg, castrated, male, mixed-breed dog was evaluated at the University of Tennessee Veterinary Teaching Hospital because of lethargy, stiffness, and progressive paraparesis of 2 week's duration. On physical examination, the dog was found to be lethargic and febrile (39.7°C). On neurologic examination, the dog was found to be depressed and paraparetic, and postural reactions and normal spinal cord reflexes were absent in the pelvic limbs. Superficial pain sensation was decreased in both pelvic limbs, although deep pain sensation remained intact. The cutaneous trunci reflex was absent caudal to T4. Thoracic limbs and cranial nerves were normal, and there was no sign of spinal pain. The lesion was localized to the T4 to T6 spinal segments.
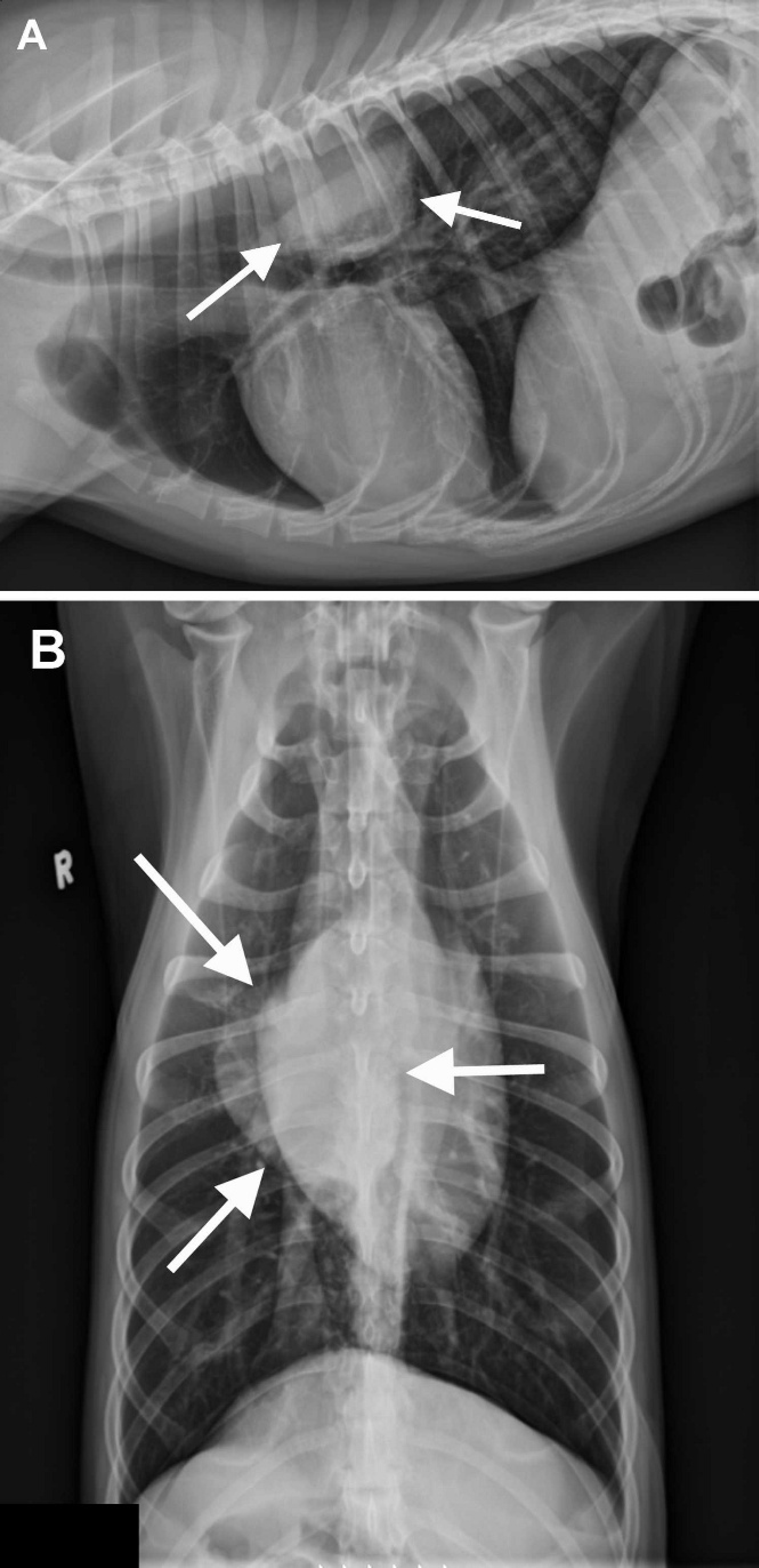
Notable laboratory findings included moderate hypoglycemia and mild hypernatremia. Survey radiographs of the spine revealed a mild narrowing of the C2 to C3 intervertebral disc space. A myelogram disclosed an attenuation of the dorsal and ventral contrast column at the level of T4 to T6, centered over T5. A soft-tissue opacity ventral to the spine was also seen at this location. Subsequent thoracic radiographs revealed a right dorsal thoracic mass approximately 9 cm long and to the right of the thoracic spine, extending from the 5th to 7th thoracic vertebra (Fig. 1A, 1B). Computed tomography (CT) revealed a mass of approximately 6 cm in diameter associated with the right dorsal aspect of the thoracic cavity immediately ventral to the spine and ribs that showed invasion of the right ventral aspect of the vertebral canal at the level of the intervertebral foramen T5–T6 (Fig. 2) resulting in displacement of the spinal cord. Based on the imaging findings, a neoplasm of the paraspinal soft tissues or a large nerve sheath tumor was considered the most likely diagnosis. The dog was euthanized because of the poor prognosis.
Gross postmortem examination revealed a 7.5 cm × 7 cm × 5 cm encapsulated, fluctuant mass attached to the right dorsal body wall in the region of the third and fourth thoracic vertebra. The mass was variegated, tan, and purple to gray to red on cut surface. The mass entered the vertebral canal between T3 and T4, and the dorsal and ventral nerve roots traveled through the mass without grossly visible disruption. In addition, T4 was focally lytic adjacent to the mass, and there was dark red, gelatinous material in the vertebral canal between T1 and T4. The spinal cord was moderately compressed and soft at T3. The gross preliminary diagnosis was an invasive neoplasia/malignancy, with focal moderate subacute myelomalacia and spinal cord compression.
Tissues were collected in neutral buffered 10% formalin solution, processed routinely, and stained with hematoxylin and eosin. Within a section of dorsal intercostal muscle there was a partially encapsulated, poorly demarcated, multilobulated mass made up of a proliferation of round to polygonal cells arranged in trabeculae and packets delineated by fine fibrovascular tissue (Fig. 3). These neoplastic cells had abundant fine granular eosinophilic cytoplasm and eccentrically located round vesicular nuclei with basophilic to finely stippled chromatin. There was moderate anisocytosis, marked anisokaryosis, and 1–2 mitotic figures per high power field. Foci of necrosis characterized by loss of cellular detail and karyolysis were accompanied by regions of hemorrhage and siderophage accumulation. Churukian-Schenk staining revealed positive granules within the neoplastic cell cytoplasm (Fig. 4). Fontana-Masson staining, an argentaffin stain, was negative within the mass. In the associated spinal cord, the central canal was focally dilated and filled with blood, fibrin, granular eosinophilic material, and rare mononuclear cells. Marked Wallerian degeneration with axonal vacuolation and spheroid formation was noted. The associated vertebrae was infiltrated with neoplastic cells through the intercostal space through the articulation of the vertebrae and rib.
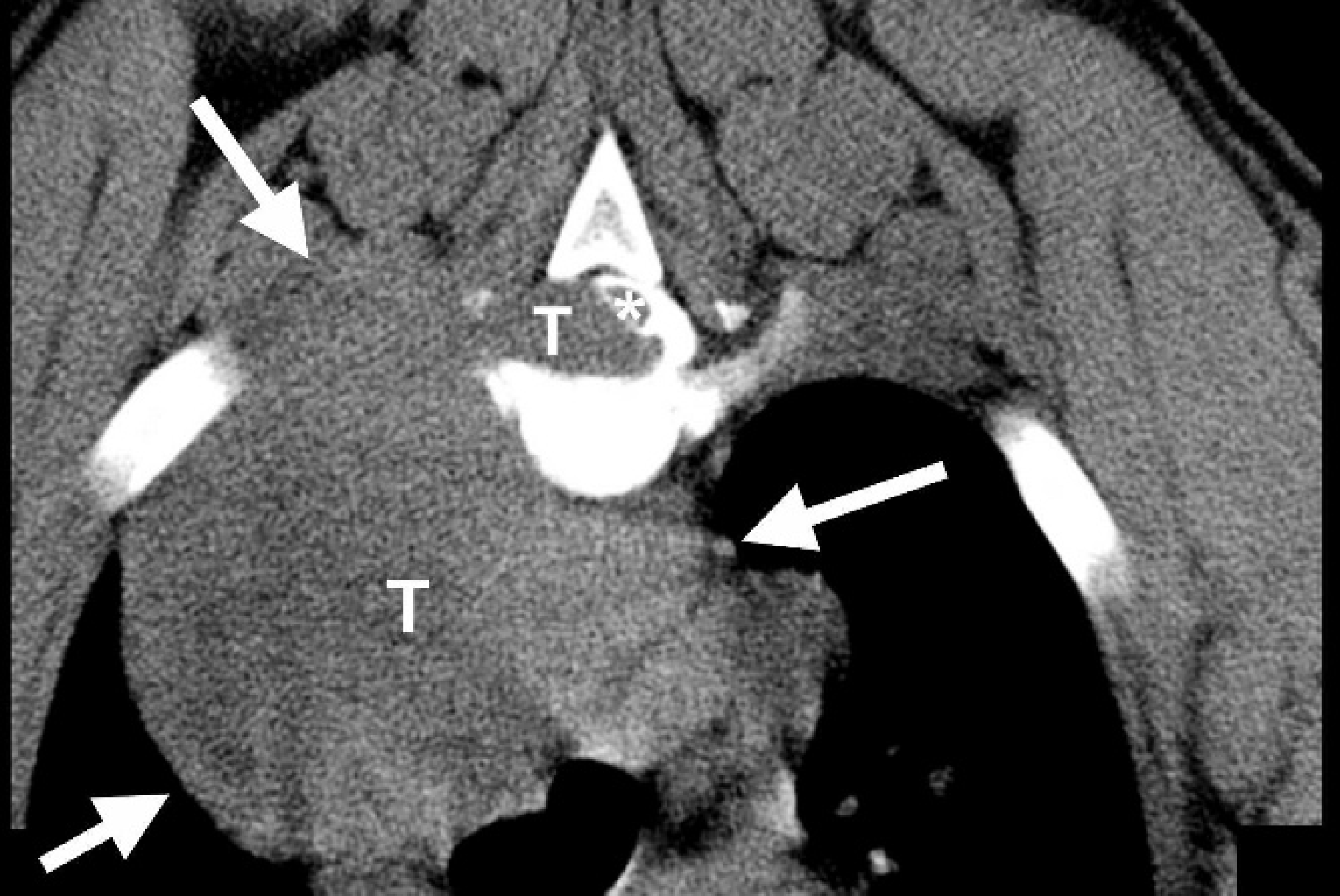
Transverse computed tomography image of the thoracic spine at the level of the intervertebral disc space T5-T6. There is an approximately 6-cm mass (T; arrows) associated with the right dorsal aspect of the thoracic cavity immediately ventral to thoracic spine and ribs, with invasion of the right ventral aspect of the vertebral canal, left dorsal displacement of the spinal cord (white asterisk), and widening of the vertebral canal.
Three-micron thick tissue sections were placed on positively charged slides and processed for IHC staining for S100, neuron-specific enolase (NSE), and synaptophysin using the IHC laboratory at the University of Tennessee. Appropriate positive control tissue included canine pancreatic islets, brain, nerve, and adrenal medulla. Negative control slides included the neoplasm processed without primary antibody and with substitution of universal negative control rabbit serum. The neoplastic cells revealed moderate expression for cytoplasmic neuron-specific enolase and strong and diffuse expression for synaptophysin (Fig. 5). The S100 expression was negative. Additional formalin-fixed tissue was sent to an independent IHC laboratory (New Bolton Center, Immunohistochemistry Lab, University of Pennsylvania) for chromogranin A staining. The additional tissue was found to be negative.
As a group, endocrine cell system tumors can be divided into 2 main categories, neuroendocrine and endocrine tumors. 12 Endocrine tumors usually arise from either the follicular cells of the thyroid gland or from the suprarenal cortex (adenomas and adenocarcinomas), and their identification can be accomplished using routine histologic staining. 12 Special histochemical stains are not usually needed.
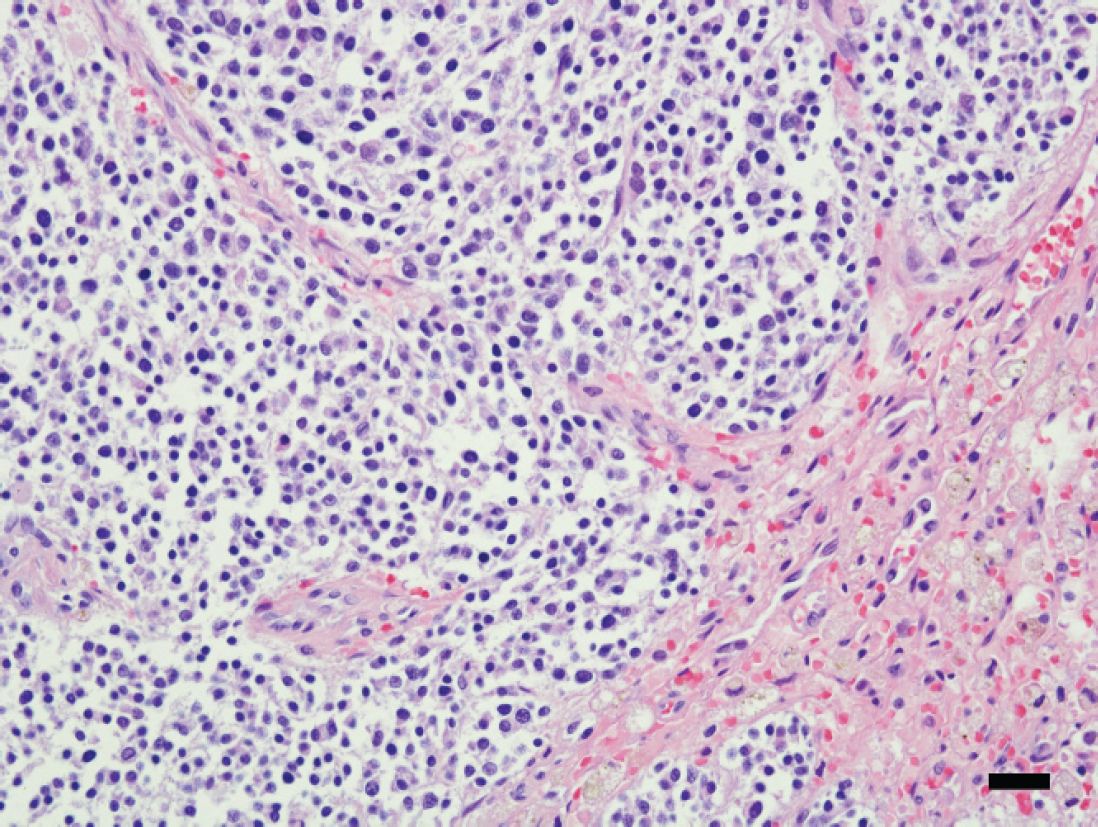
Photomicrograph demonstrates the neoplastic round cells arranged in small clusters or packets. The cells are round with discrete borders, minimal cytoplasm, and large round vesicular nuclei. Hematoxylin and eosin. Bar = 75 μm.
Neuroendocrine tumors can be further divided into either neuroectodermal or endodermal etiologies. 12 Neuroectodermal tumors arise from the adrenal medulla (pheochromocytomas and neuroblastomas) and from the paraganglia, whereas endodermal tumors arise in the pituitary gland, parathyroid gland, thyroid gland, or pancreas or from the diffuse endocrine system of luminal organs such as the gastrointestinal tract (carcinoids). 12 All neuroendocrine tumors can be characterized by the intracytoplasmic hormonal secretory granules. These granules can only be visualized at the light microscopic level using silver stains such as the Grimelius argyrophil reaction or Churukian-Schenk stain. 12 Immunohistochemistry using antibodies against chromogranin can also be used to identify neuroendocrine tumors. 12
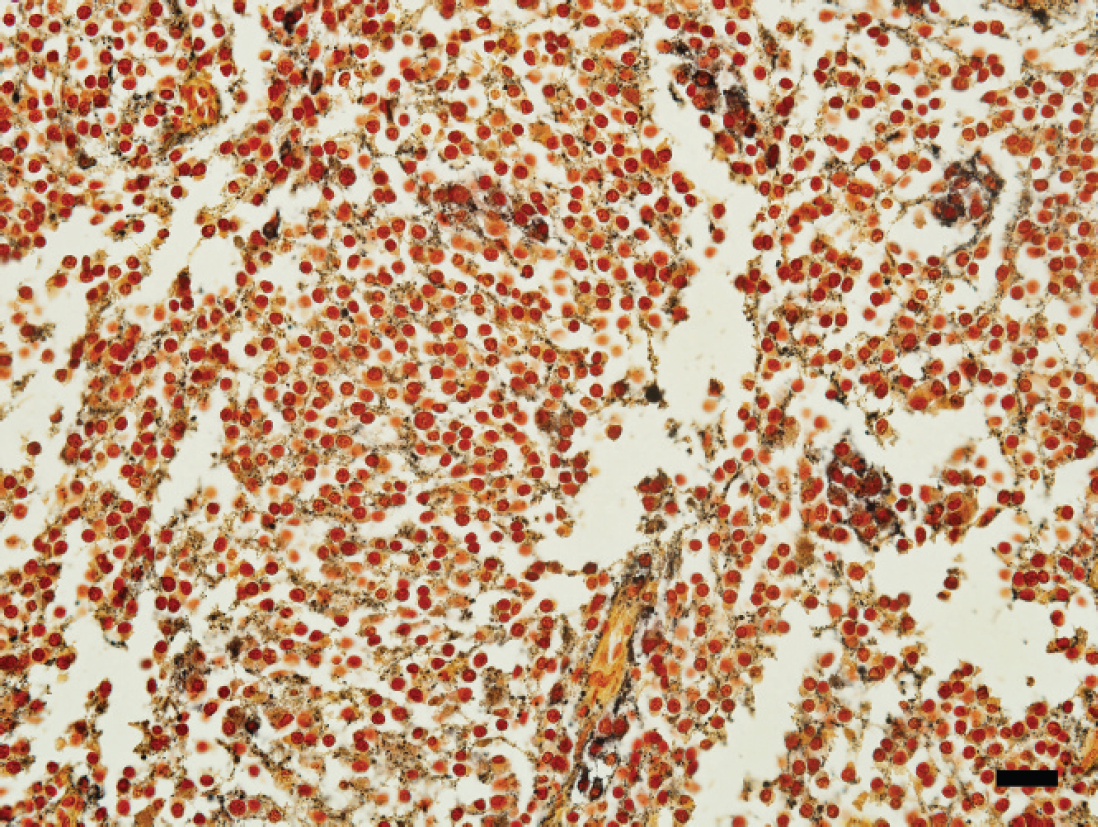
The neoplastic cell cytoplasm contains granules that stain black with the argyrophilic silver stain. Churukian-Schenk. Bar = 75 μm.
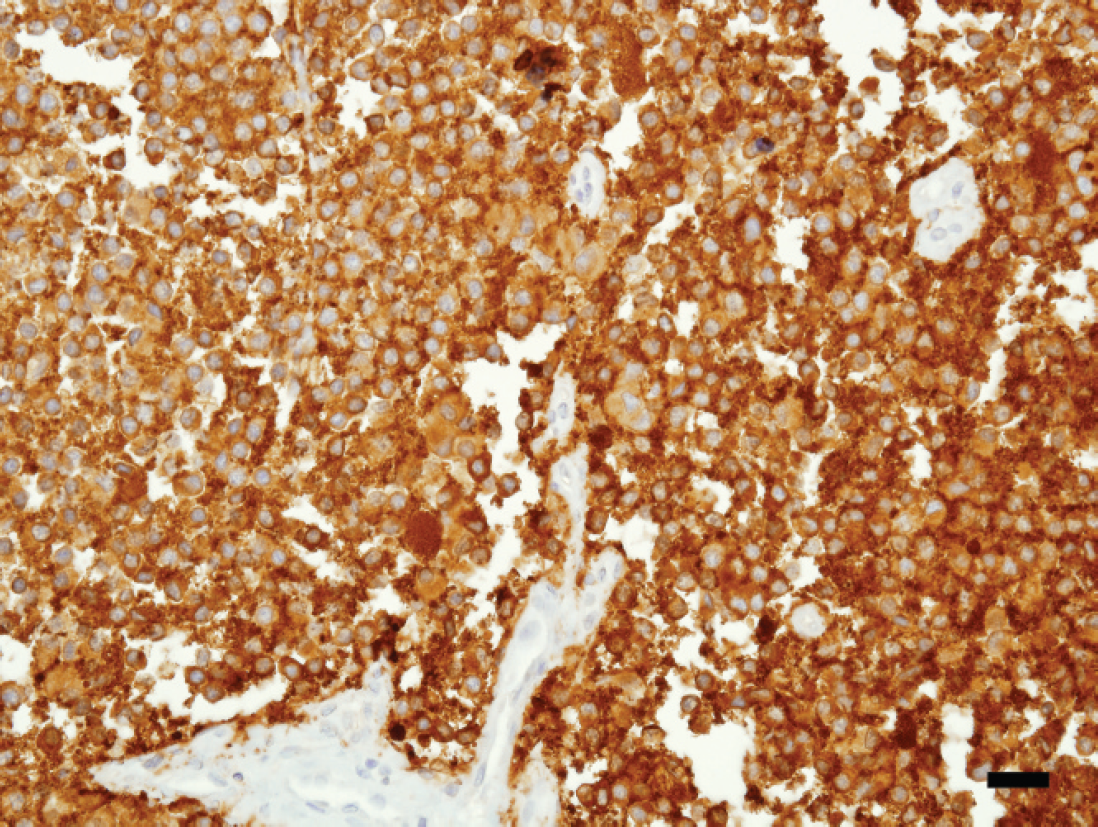
The neoplastic cells show strong diffuse cytoplasmic expression for synaptophysin. Bar = 40 μm.
The mammalian paraganglion system includes the adrenal medulla, chemoreceptors, the vagal body, and small groups of cells associated with the thoracic, intra-abdominal, and retroperitoneal ganglia. 10 Neuronal and nerve cell tumors arise most frequently from the sympathetic and paraganglionic components of the autonomic nervous system. 8 Tumors arising from the sympathetic component of the nervous system are referred to as neuroblastomas whereas parasympathetic nervous system tumors are called paragangliomas. 8 Paragangliomas can be further divided into pheochromocytomas and chemodectomas. 8
In human medicine, paragangliomas were initially classified based on their chromaffin reaction. 10 Chromaffin reaction suggests sympathetic origin or at least production of catecholamines. 11 Although this classification system is not perfect, chromaffin reaction is rare, except in the adrenal gland, and such tumors are generally described as extra-adrenal chromaffin paragangliomas or pheochromocytomas. 11 Tumors originating from the parasympathetic nervous system are called nonchromaffin paragangliomas or chemodectomas. 10
Unfortunately, chromaffin reaction does not always reliably separate these tumors, and all paragangliomas can produce catecholamines to some extent. 10 This can be especially true in cases of malignant undifferentiated neoplasms that may have lost characteristic traits or acquired new neurosecretory traits. 2,3
Paragangliomas have been reported to arise from the pulmonary arch, aortic arch, or the segmental paraganglia of the sympathetic chain. 10 Paragangliomas are usually soft, well-circumscribed, encapsulated masses that can be locally invasive. 7 Chemodectomas are the most common type of paraganglioma in dogs arising from the anterior mediastinum. 10 Affected dogs are usually older (average of 10 years), male, and of the brachiocephalic breeds, and Boxers and Boston Terriers are overrepresented in this group. 5 The tumor pathogenesis and breed predisposition has been suggested to be due to chronic hypoxemia and is often found in association with other primary endocrine neoplasias. 5
Posterior mediastinal paragangliomas arising from the sympathetic paraganglia appear to be less common. 10 In 1993, a study reported a 4-case series of metastatic extra-adrenal paragangliomas in dogs that caused neurologic signs. 6 Primary paragangliomas arising from the sympathetic paraganglia and invading into spinal cord have also been reported in horses, cats, and cows. 7 To the authors' knowledge, spinal cord invasion of a primary mediastinal paraganglioma in a dog has only been described in 2 previous reports. 9,10
Histologically, paraganglioma cells are usually arranged in packets or lobules of varying size surrounded by well-vascularized stroma. 7 The nuclei have finely stippled chromatin with small nucleoli, and the mitotic index may be high. 7 Synaptophysin and chromogranin A staining are usually positive. and expression of NSE is variable. 7 In contrast, chemodectomas do not usually demonstrate chromaffin granules, and the tumor cells do not stain for chromogranin A. 2
In the current case, Churukian-Schenk staining revealed positive granules (chromaffin reaction) within the neoplastic cell cytoplasm, thereby confirming the argyrophilic nature of the cells and hence their catecholamine-producing potential (chromaffin or sympathetic nervous system origin). 4 The argyrophilic reaction is caused by the silver affinity of the chromogranin molecule, seen in cells of neuroendocrine origin. 12 Substances known to be argyrophilic and argentaffin-expressing include tryptophan, tyrosine, dopamine, norepinephrine, 5-hydroxytryptamine, and 5-hydroxyindole. 12 Epinephrine, 5-hydroxyindole-3-acetic acid, and 5-hydroxytryptophan are argentaffin only. 12 Interestingly, Fontana-Masson staining, an argentaffin stain, was negative within the mass, suggesting a non-chromaffin tumor origin.
The tumor cells also revealed expression for cytoplasmic NSE and synaptophysin, whereas S100 and chromogranin A expression was found to be negative. An IHC study of 25 chemodectomas found that 68% (17/25) were positive for both NSE and synaptophysin, whereas only 4% (1/25) were positive for S100 expression. 1 It was also noted that 56% (14/25) of the chemodectomas showed positive expression of chromogranin A. 1 The conclusion that IHC did not aid in recognition of less well-differentiated tumors was based on this information. 1
Mediastinal extra-adrenal paragangliomas are rare neoplasms, especially in young dogs, but should be included as a possible differential diagnosis for intrathoracic neoplasms as well as possible causes for progressive paraparesis. Diagnosis is based on a combination of historical, physical, and radiographic examination. Immunohistochemical analysis, although useful in confirming whether the tumor is of neuroendocrine origin, may not allow for further subclassification in cases of malignant undifferentiated neoplasias. Prognosis is based on the clinical signs, location, and possibility of surgical removal of the primary tumor.