
Abstract
An extra-adrenal retroperitoneal paraganglioma was observed in a 10.5-year-old male Boxer dog. Additionally, the dog had an aortic base tumor, multiple thyroid adenomas, multiple testicular interstitial cell tumors, bilateral nodular adrenal cortical hyperplasia, and parathyroid gland hyperplasia. The hypothesis that the retroperitoneal mass represents a primary extra-adrenal paraganglioma rather than metastatic mass from the aortic body tumor is considered. Either primary or metastatic extra-adrenal retroperitoneal paragangliomas are rarely reported in dogs.
Paragangliomas are neuroendocrine tumors that arise from paraganglia, which are organs composed of cells derived from the neural crest that are associated with the autonomic nervous system throughout the body. 11 The paraganglionic system consists of adrenal medulla, chemoreceptors, vagal body, and small groups of cells associated with thoracic, intra-abdominal, and retroperitoneal ganglia. 11 Paragangliomas in dogs occur mainly in the aortic and carotid bodies 4 ; these bodies are chemoreceptor organs, and paragangliomas arising in these organs are also called chemodectomas or aortic body tumor and carotid body tumor, respectively. 4 Other sites for primary paragangliomas include intrathoracic (mediastinal) 11 and left atrial. 3 Metastatic sites usually include liver, myocardium, intracardiac, lung, kidney, lymph nodes, pancreas, adrenal cortex, brain, and bone.4,5,10,16 Invasion of adjacent tissues has been reported for malignant tumors with invasion of atria, pericardium, large adjacent blood vessels, and spinal cord.4,11 Rarely, retroperitoneal or abdominal paravertebral tumors, either primary or metastatic, have been reported in dogs. 6
A 10.5-year-old, 33.5-kg, male, Boxer dog was presented for postmortem examination to the Tifton Veterinary Diagnostic and Investigational Laboratory, University of Georgia (Tifton, Georgia). The dog had a short clinical history of sudden collapse and death within a few hours. At postmortem examination, the dog was in good nutritional condition with minimal postmortem decomposition. The membranous mucosa of the oral cavity and conjunctiva were pale. There were approximately 1.8 liters of free blood within the abdomen. Large blood clots were observed within the dorsal middle abdomen, cranial to the kidneys, between visceral surface of the liver, stomach, and mesenteric roots. An abdominal, 5-cm × 4.5-cm × 3-cm, soft mass was observed within the adipose tissue of the retroperitoneum at the origin of the cranial mesenteric artery and celiac artery, in close association with the mesenteric aorta. On cut section, the mass was soft and white and had multifocal dark red areas (Fig. 1A). A blood vessel on the capsular surface of the mass appeared to be ruptured and was implicated as the cause of the hemoabdomen. Adrenal glands were not attached to the mass and were easily dissected and removed. Both adrenal glands had multifocal, a few millimeters in diameter, cortical nodules. Kidneys, liver, and the serosa of the gastrointestinal tract were diffusely pale. A 3-cm × 2-cm × 1-cm mass was observed at the base of the heart, adjacent to the left auricle and pulmonary artery, near the origin of the aorta (Fig. 1B). On cut section, the mass had firm white areas intermingled with soft dark red areas. The right thyroid gland had multifocal to coalescing dark red nodules of approximately 1 cm in diameter. One testicle had a single, 1.5 cm in diameter, light to dark red mass. The other testicle had multifocal, 3–5-mm, gray to light red masses. The dog had a heart base tumor that was grossly interpreted as a paraganglioma (chemodectoma) or aortic body tumor. Differential diagnoses for the thyroid nodules included thyroid nodular hyperplasia, multiple adenomas, or carcinoma. The adrenal cortical nodules were interpreted as cortical nodular hyperplastic areas. The testicular tumors had a gross appearance of interstitial cell tumors. The cause of death was hypovolemic shock due to the hemoabdomen. Gross differential diagnoses for the retroperitoneal tumor included hemangiosarcoma, liposarcoma, other sarcomas, metastatic mass from aortic base tumor, or thyroid tumor.
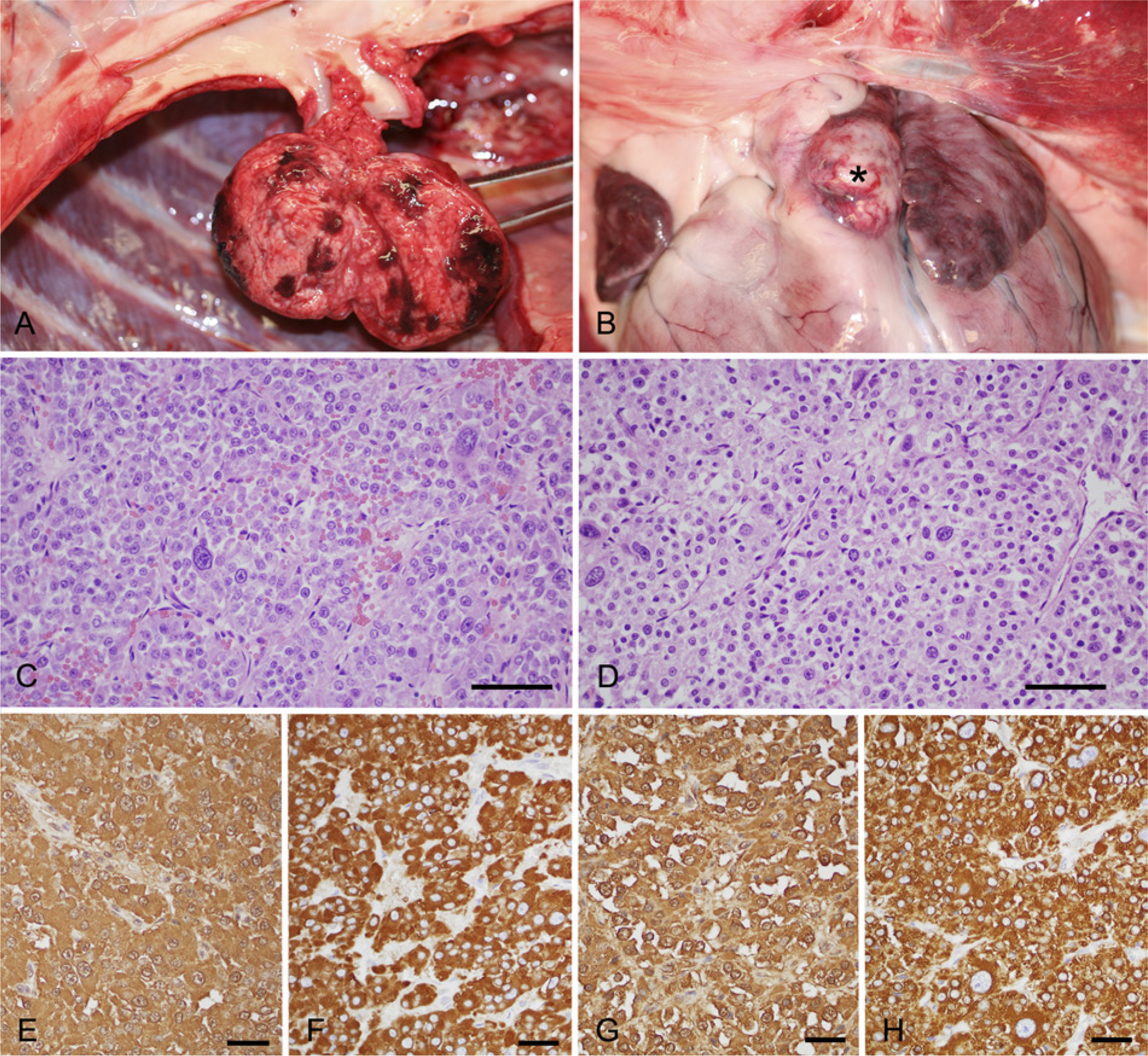
Paragangliomas in a dog.
Tissues collected during necropsy were formalin-fixed. For histology, tissue samples were trimmed, embedded in paraffin, sectioned at 5-µm thickness, and stained with hematoxylin and eosin. The retroperitoneal mass was composed of lobules of polyhedral cells separated by fine fibrovascular stroma. Neoplastic cells had distinct cell borders, moderate amounts of eosinophilic granular to vacuolated cytoplasm, and round to oval nuclei with predominantly single central nucleoli and coarsely stippled chromatin. Anisocytosis and anisokaryosis were marked, and cells with karyomegalic and bizarre nuclei were frequently observed (Fig. 1C). Mitoses were 17 per 10 high-power fields (400×) examined. Multifocal areas of necrosis and hemorrhage were seen. A section of a ganglion was seen at the periphery of the retroperitoneal mass; this ganglion was interpreted as part of the celiac and cranial mesenteric ganglia and plexus based on the gross location of the mass. Histological sections of the heart base mass revealed a neoplasm with similar histological features of the retroperitoneal mass (Fig. 1D). Mitoses were 15 per 10 high-power fields (400×) examined.
The left thyroid gland had multifocal nodular proliferations of well-differentiated follicular cells with well-defined cystic follicles. Throughout the gland, cystic dilation of scattered follicles was observed. The section of right thyroid gland had attached parathyroid glands that were mildly hyperplastic. Sections of adrenal glands had multifocal cortical nodular hyperplastic areas. Sections of the testicles had marked atrophy and multifocal areas of proliferation of polyhedral cells with vacuolated to eosinophilic cytoplasm and round to oval nuclei with mild anisokaryosis consistent with interstitial cell tumor.
Immunohistochemical staining for chromogranin A and synaptophysin was performed in sections of the retroperitoneal tumor and the heart base tumor. For chromogranin A, the primary antibody used was polyclonal rabbit anti-human chromogranin A a at a dilution 1:8,000 with an incubation period of 60 min. Positive tissue control was canine pancreas. For synaptophysin, the primary antibody used was monoclonal mouse anti-synaptophysin b at a dilution of 1:400 with an incubation time of 60 min. Positive tissue control was canine spinal cord. Expression of chromogranin A and synaptophysin was observed in neoplastic cells of the retroperitoneal mass and heart base tumor (Fig. 1E–1H). Chromogranin was observed in nearly 100% of the cells, and the cytoplasm of these cells had medium to high intensity stain in both tumors. Intracytoplasmic expression of synaptophysin was diffuse, and approximately 95% of the cells showed high-intensity stain in both tumors.
Based on the cell morphology, mitotic index (<2 mitoses per single high-power field), and immunohistochemical staining pattern for chromogranin A, the heart base tumor and the retroperitoneal tumor would be classified as grade II paragangliomas based on a previous study. 1 However, a study published in 2013 has demonstrated that there is no practical value or difference in immunohistochemical staining, mitotic index, and cell morphology between tumors with presence or absence of metastases, 15 making the grading system for these tumors a questionable factor to predict metastatic disease.
For electron microscopy, a paraffin block of the retroperitoneal mass was used. One-millimeter cubes were removed from the paraffin block, deparaffinized, and routinely processed for electron microscopy. Neoplastic cells contained numerous small intracytoplasmic electron dense bodies that were interpreted as neurosecretory granules (Fig. 2).
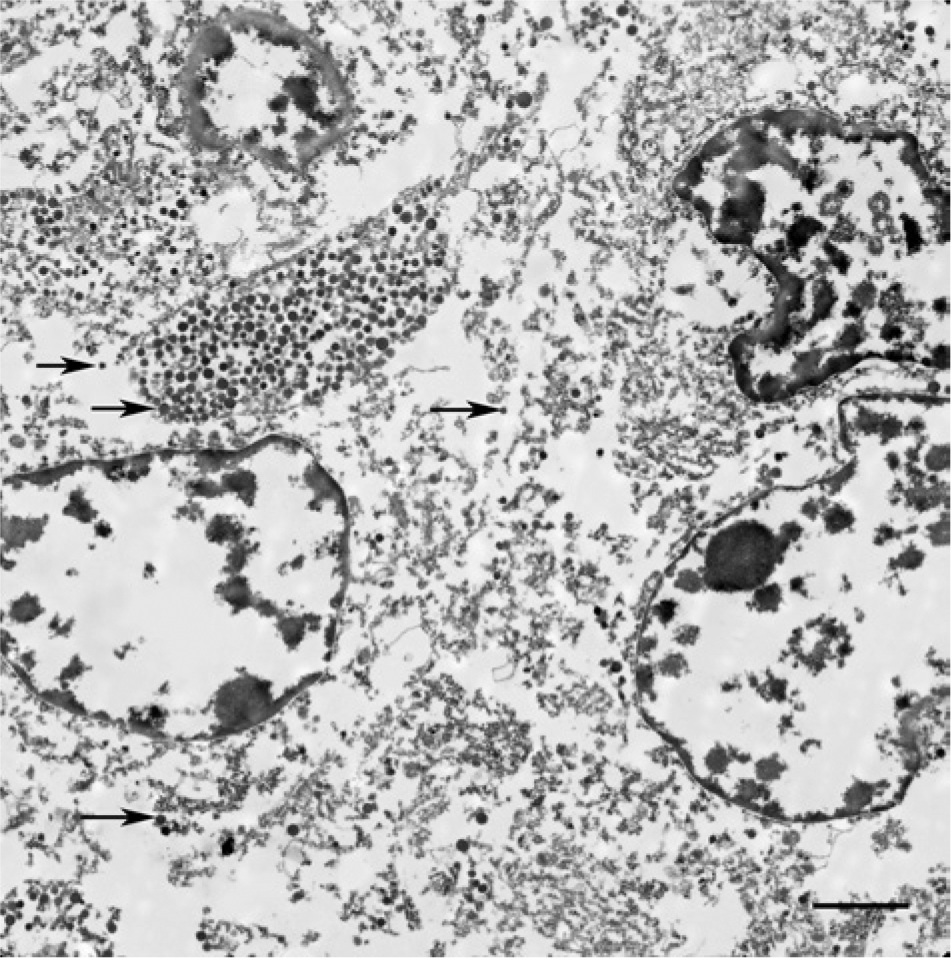
Retroperitoneal extra-adrenal mass; dog. Neoplastic cells contain intracytoplasmic electron dense neurosecretory granules (arrows). Electron microscopy. Bar = 2.5 µm.
Based on the histologic, immunohistochemical, and electron microscopy findings, the heart base tumor and the abdominal retroperitoneal mass were diagnosed as paragangliomas. The heart base mass was consistent with an aortic body tumor (chemodectoma) and the intra-abdominal mass was considered an extra-adrenal paraganglioma. Other lesions observed were multiple thyroid gland adenomas, multiple testicular interstitial cell tumors, bilateral adrenal cortical nodular hyperplasia, and parathyroid gland hyperplasia, suggesting possible multiple endocrine neoplasia syndrome in this dog.
The dog had 2 tumors from different locations consistent with paragangliomas. These 2 tumors could represent multicentric origin of paragangliomas or the retroperitoneal mass could represent a metastatic site of a primary aortic body tumor. Brachycephalic breeds of dogs such as Boxer and Boston Terrier are highly predisposed to develop paragangliomas, 4 and multicentric neoplastic transformation of chemoreceptor tissue occurs frequently in brachycephalic dogs. Approximately two thirds of brachycephalic dogs with carotid body tumors also develop aortic body tumors. 4
Paragangliomas in dogs are reported to occur mainly in the aortic and carotid bodies. 4 Retroperitoneal location of paragangliomas is rare in dogs; there is a single case report of a paraganglioma originating in the periglandular connective tissue of the adrenal gland in a dog. 6 In human beings, extra-adrenal retroperitoneal or paravertebral paragangliomas arise from specialized neural crest cells symmetrically distributed along the aorta in close association with the sympathetic chain.8,13 These tumors are closely related to the abdominal aorta and can develop as suprarenal, renal hilar, or infrarenal tumors. 8 The most common location is usually infrarenal, in the area known as the organ of Zuckerkandl. 8 In human beings, these groups of retroperitoneal paraganglionic cells can be observed as 1–3 mm in diameter organs distributed in the retroperitoneal fat; such cells have been previously misdiagnosed as metastatic carcinoma cells. 14 Although paragangliomas of retroperitoneal location are uncommon in dogs, the possibility of a primary origin as described in human beings has to be considered. Similarly to human beings, paraganglionic tissue has been identified in the retroperitoneum of dogs. 9 The largest group of paraganglionic cells in the retroperitoneum of dogs consistently occurs ventrally and laterally to the abdominal aorta in the mid-retroperitoneum, with smaller aggregates distributed around the adrenal gland and around the origin of the caudal mesenteric artery. The aggregates localized around the caudal mesenteric artery are comparable with the organ of Zuckerkandl described in human beings. 9
Most of the canine paragangliomas usually express neuron-specific enolase, synaptophysin, and chromogranin A.1,2 Expression of S100 is variable and usually absent in most tumors. 2 It seems that chromogranin A is less expressed in higher grade paragangliomas 2 and, in a previous study, chromogranin A was not expressed in high-grade (grade III) paragangliomas that usually have higher metastatic potential. 1
The dog from the present report had multiple hyperplastic and neoplastic lesions of endocrine origin. Whether this represents multiple endocrine neoplasia syndrome is debatable. Extra-adrenal paragangliomas of retroperitoneum have been associated with multiple endocrine neoplasia syndromes in human beings. 13 In dogs, tumors in several different endocrine organs have been occasionally reported. Multiple endocrine neoplasia syndromes have been previously described in dogs.7,12 Whether these dogs may have familial or genetic predisposition similar to multiple endocrine neoplasia described in human beings or the occurrence of multiple endocrine neoplasms is simply coincidental is unknown. 7
In conclusion, based on the fact that 1) a large percentage of paragangliomas in brachycephalic dogs involve multicentric origin, 2) the retroperitoneal location is not a common metastatic site of paragangliomas in dogs, 3) metastases in other organs were not observed in this dog, 4) a previous report described a para-adrenal paraganglioma in a dog, and 5) paraganglionic cells are found in the retroperitoneum of dogs, it is plausible that the extra-adrenal paraganglioma observed in the dog from the present report may represent a local primary tumor and that the current report is a case of multicentric paragangliomas in a dog.
Footnotes
Acknowledgements
The authors thank the histology staff (Diane Rousey, Kim Bridges, and Mellisa Gandy) and the electron microscopy technician (Debby Blakey) from the Tifton Veterinary and Investigation Laboratory (UGA) for their invaluable technical assistance, and Abby Butler from the Athens Veterinary Diagnostic Laboratory (UGA) for immunohistochemical staining.
a.
A0430, Dako North America Inc., Carpinteria, CA.
b.
Snp88, MU363-UC; BioGenex Laboratories Inc., San Ramon, CA.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.