
Abstract
A 9-y-old, spayed female, non-brachycephalic mixed-breed dog was presented with progressive abdominal distension and diarrhea of <24 h duration. An echocardiogram revealed nodular masses in the pericardium and myocardium, particularly near the auricles. Diagnostic and therapeutic pericardiocentesis failed to improve the dog’s status, and the owner elected euthanasia. The autopsy revealed numerous nodules within the pericardium, heart base, and myocardium of the left and right ventricles. Histopathology revealed the presence of a neuroendocrine tumor, immunopositive for chromogranin A and negative for synaptophysin and calcitonin, supporting the diagnosis of aortic body tumor with intracardiac metastasis.
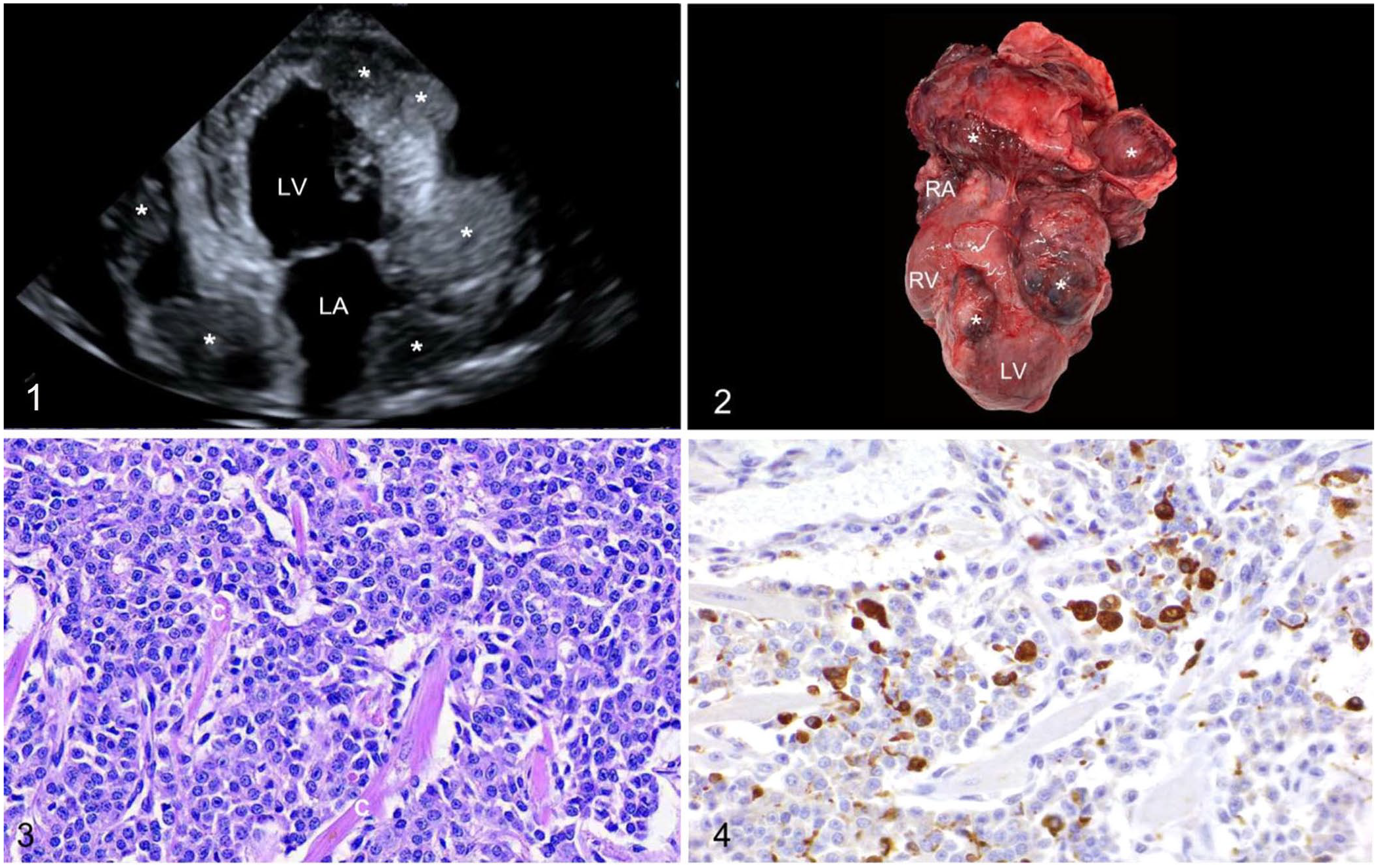
A 9-y-old, 21-kg, spayed female, non-brachycephalic mixed-breed dog was presented to the Virginia-Maryland College of Veterinary Medicine, Veterinary Teaching Hospital (VMCVM-VTH; Blacksburg, VA, USA), with progressive abdominal distension and diarrhea of <24 h duration. A dry, unproductive, non-progressive cough was first noted approximately one month prior. Physical examination yielded bilateral muffled heart sounds, a grade 3 of 6 left apical systolic heart murmur, paradoxic pulse, increased inspiratory effort, and a moderately fluid-distended abdomen. Other findings included a body condition score of 7 of 9 and moderate dental disease. The dog underwent an echocardiogram with the VMCVM-VTH Cardiology Service. Upon imaging, the patient had a heart rate of 150 bpm, and no arrhythmia was noted, although the electrocardiogram displayed beat-to-beat alteration of amplitude of QRS complexes (interpreted as electrical alternans). Imaging confirmed the presence of subjectively moderate amounts of pericardial effusion. However, several nodular and infiltrative masses were noted on the pericardium and epicardium and closely associated with the left and right atria. Additionally, a mass infiltrating the apical left ventricular free wall was noted (Fig. 1). The largest mass at the left atrioventricular groove was ~3.5-cm diameter. The disseminated distribution of nodules on both sides of the heart raised concern for malignant neoplasia.
Aortic body tumor with intracardiac metastasis in a dog.
Following the echocardiogram, a therapeutic pericardiocentesis was performed with a 16-ga, 8.23-cm over-the-needle catheter at the left and right fourth intercostal spaces. A diagnostic and therapeutic thoracocentesis was performed with an 18-ga, 4.78-cm over-the-needle catheter in the right seventh intercostal space. The obtained serosanguineous fluid had a PCV of 0.13 L/L. An abdominocentesis was also performed with identical materials as for the thoracocentesis, revealing serous fluid with a PCV of 0.08 L/L. The patient received a 10-mL/kg intravenous bolus of lactated Ringer solution over 10 min in an attempt to improve hemodynamic stability and prevent further cardiac tamponade of the right heart. The dog went into respiratory distress shortly after being placed in its cage and the owner elected in-hospital euthanasia. The dog was sedated with fentanyl citrate (2.5 µg/kg, 1 mL IV; Hospira), and euthanized with pentobarbital sodium (Euthasol, 6 mL IV; Virbac).
On postmortem examination, the subcutis of the thorax and abdomen was expanded by transparent, gelatinous edema. The thoracic cavity contained ~100 mL of serosanguineous fluid. The lungs were multifocally red and slightly firm; some sections of the lung sank in formalin, interpreted as compression atelectasis. The pericardial sac was markedly dilated with ~50 mL of serosanguineous fluid and fibrin. Upon opening the pericardial sac, numerous 0.3–1-cm, pale-gray to pale-red nodules were identified dispersed throughout the wall of the sac. Similar 1–3.5-cm masses were present in the heart base and myocardium, compressing the pulmonary trunk and both auricles, and multifocally infiltrating the myocardium of the left ventricle (Fig. 2). The abdomen was filled with red-tinged fluid. The liver was dark-red with an irregular surface, and the mucosa of the gallbladder had small, 1–2-mm cysts. The spleen had several red, raised, 1–1.5-cm nodules dispersed throughout the parenchyma. No significant findings were identified in the other internal organs, including the brain. Sections of the lungs, heart (including the masses in the pericardium, myocardium, and heart base), diaphragm, liver, gallbladder, spleen, kidneys, urinary bladder, adrenal glands, esophagus, stomach, small intestine, pancreas, cecum, colon, and brain were analyzed with routine H&E stain.
All histologic sections obtained from the heart had similar findings. Numerous fairly well-demarcated, non-encapsulated, densely cellular masses infiltrated the myocardium and pericardial sac, and were composed of packets of moderately pleomorphic polyhedral cells sustained in fine trabeculae of fibrovascular tissue. Individual cells palisaded along the trabeculae, and had small-to-moderate amounts of eosinophilic cytoplasm and conspicuous cell margins. Nuclei were round, with mild anisokaryosis, finely stippled chromatin, and zero or one prominent nucleolus. There were 2 mitotic figures in 2.37 mm2. The mass multifocally infiltrated, dissected, and individualized myofibers (Fig. 3). Occasional clusters of neoplastic cells were noted in thin-walled vessels. Numerous hemosiderin-laden macrophages were within the supporting fibrous stroma. Findings in other organs included moderate centrilobular congestion with vacuolar degeneration of hepatocytes in this area, mucinous hyperplasia of the gallbladder, and multifocal lymphoid hyperplasia in the spleen.
Immunohistochemistry (IHC) was performed for synaptophysin, chromogranin A, and calcitonin on heart sections following the standard procedures of the Animal Disease Diagnostic Laboratory, Purdue University (West Lafayette, IN, USA; Table 1). Sections were counterstained with Mayer hematoxylin and coverslipped. Neoplastic cells were positive for chromogranin A (Fig. 4), and negative for synaptophysin and calcitonin. With these findings, our case was diagnosed as a metastatic intracardiac chemodectoma.
Immunohistochemical markers utilized in tumor identification.
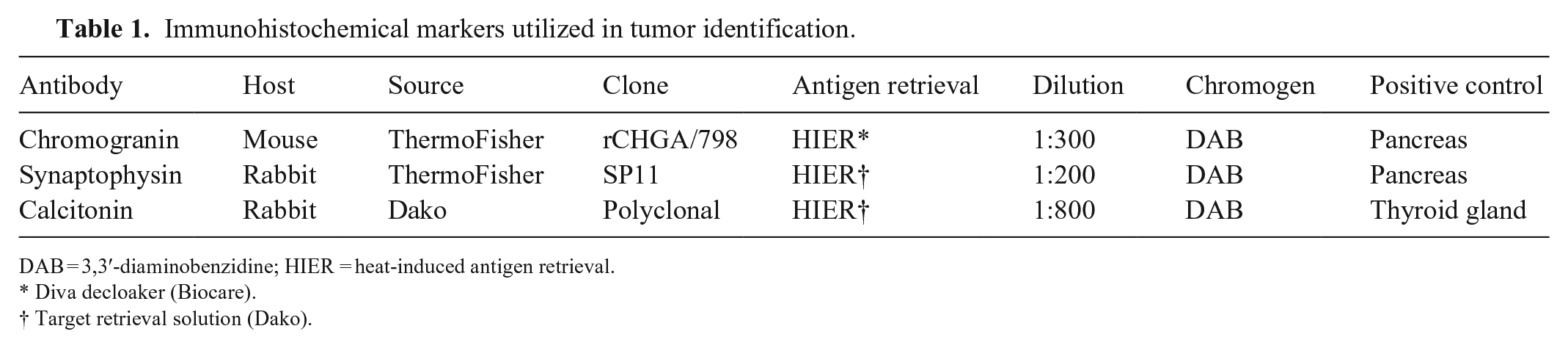
DAB = 3,3′-diaminobenzidine; HIER = heat-induced antigen retrieval.
Diva decloaker (Biocare).
Target retrieval solution (Dako).
Common heart-base tumors include hemangiosarcoma (HSA), lymphoma, ectopic thyroid tumors, and chemodectomas. These tumors often appear similar grossly and require histology or IHC for differentiation. 14
Primary cardiac HSA of the right auricle is the most common cardiac tumor of dogs. These highly malignant tumors, arising from vascular endothelial cells, most commonly affect Golden Retrievers, German Shepherd dogs, Maltese dogs, and Miniature Dachshunds. 17 Clinical signs associated with HSA are lethargy, collapse, abdominal distension, exercise intolerance, and dyspnea and cough. Neutrophilia and mild regenerative anemia are often present in affected dogs.14,16 HSA often occurs as a single mass involving the right auricle, right atrium, or right atrioventricular junction, but has been found concurrently with a splenic mass in up to 29% of cases. These cardiac masses tend to be dark-red, poorly circumscribed, lobulated, and widely ranging in both size and weight. Histologic features can vary but typically include spindle-shaped cells organized to form blood-filled cavities and networks and an overall cavernous structure. 17
Lymphoma affecting the heart in dogs is uncommon but can cause diffuse or nodular lesions. Ectopic thyroid tumors, adenomas, and carcinomas can occur at the heart base and can invade surrounding structures. Ectopic thyroid tumors can appear histologically similar to aortic body tumors, displaying a solid “endocrinoid” pattern, but will not express chromogranin A or synaptophysin. IHC may be needed to test for the presence of thyroglobulin or thyroid transcription factor-1 to completely rule out a thyroid tumor.7,16 Medullary thyroid carcinomas can express chromogranin and also calcitonin in the cytoplasm. 15 In our case, calcitonin IHC was negative, ruling out the possibility of a medullary thyroid carcinoma.
Aortic body tumors are relatively rare cardiac tumors in small animals; however, they are the most common type of chemodectoma. They arise from chemoreceptor cells located within the aortic body, carotid body, or glomus pulmonale. Dogs most frequently develop tumors of the aortic body in contrast to humans, who tend to develop them in the carotid body. 16 Central chemoreceptors are located throughout the brain; chemoreceptors serve to detect alterations of specific chemicals, such as carbon dioxide and hydrogen ions in the blood. When the partial pressure of carbon dioxide rises above a threshold, the chemoreceptors stimulate the respiratory centers to reduce the hypercapnia.
Aortic body tumors are often benign, nonfunctional, and have a low metastatic rate; however, they can be locally invasive. 3 Reports of chemodectoma metastasis in the dog are limited, but include bone, vertebrae, lung, liver, and brain.8–10 The most common clinical presentation in dogs is syncope, exercise intolerance, lethargy, and sudden death. 10 In brachycephalic breeds, particularly in Boxers, chronic hypoxia due to brachycephalic obstructive airway syndrome is postulated to be the catalyst for neoplastic transformation of the chemoreceptor cells.1,10 This is similar to a documented association of chemodectoma and high-altitude hypoxia in humans. 13 Increased incidence of chemodectomas in other brachycephalic breeds, including Boston Terriers, indicates the possibility of a familial predisposition. 18 Transthoracic echocardiography commonly reveals a discrete heart-base mass; specificity and sensitivity in dogs have been reported to be 100% and 82%, respectively. 6 Aortic body tumors tend to be unilateral, slow-growing, encapsulated masses that can form a solitary mass or multiple nodules near the base of the heart. Chromogranin A and synaptophysin have been used as important immunohistochemical markers in the diagnosis of chemodectomas.1,4,7,14
Uniquely, in our case, several nodular and infiltrative masses were noted on the pericardium and myocardium, closely associated with the left and right auricles, and infiltrating the apical left ventricular free wall. This contrasts with the usual distribution of chemodectoma, a solitary mass or multiple nodules located near the base of the heart. The presentation of multiple masses in the heart is more consistent with metastasis from another organ. 6 Routes that allow the metastases of tumors to the heart include hematogenous, lymphatic, transvenous, and direct. 5 Overall, cardiac metastases are considered rare, with rates in humans of 2.3–18.3%; a study in dogs with solid tumors suggested 4.7%.2,11 In our case, metastasis from a distant site was ruled out, as no masses were identified grossly or histologically in other organs.
Immunohistochemically, the neoplastic cells identified in our case were positive for chromogranin A and negative for synaptophysin and calcitonin. Various cases have been reported in which the expression of chromogranin A, and other proteins, has an inverse relationship with the level of malignancy.1,10,12 Chromogranin A is contained within secretory granules, which often decrease in number in malignant chemodectomas; therefore, IHC staining for chromogranin A and other proteins may be less evident in malignant tumors. 12 Therefore, the wide and infiltrative distribution of the tumors in our case may explain why the IHC was negative for synaptophysin. Further studies are required to examine the metastatic potential of aortic body tumors and factors that may affect the expression of diagnostic biomarkers.
Footnotes
Acknowledgements
We thank Dr. Hyeon Jeong for performing the echocardiogram and the Animal Disease Diagnostic Laboratory at Purdue University for assistance with immunohistochemistry.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for their research and/or authorship of this article.