
Abstract
Objectives:
Non-traumatic headache accounts for up to 4.5% of all patients presenting to the emergency department. Non-traumatic headache is generally classified into two categories: primary and secondary headache disorders. Differentiating secondary from primary headache disorders is essential. SNOOP4 is known as a mnemonic for suggesting clinicians send neuroimaging to rule out serious conditions. Yet, the benefit of using this mnemonic in the emergency department is not well established. This study aimed to assess the significance of SNOOP4 in detecting serious causes of non-traumatic headache in adults presenting to the emergency department.
Methods:
We conducted a prospective observational study of adult patients presenting to the emergency department of the single tertiary hospital over a period of 12 months. Patients with acute non-traumatic headache presented at the emergency department were included. A standard record form was used. Patients were investigated and treated following the pre-existing protocols. Results were interpreted by attending radiologists. Each factor, according to SNOOP4, was then evaluated for the ability to predict serious causes of non-traumatic headache.
Results:
A total of 90 patients were included in this study with complete details obtained on 83 (92.2%) patients. Of these, 63 (75.9%) were female. The mean age was 44.5 years (inter-quartile range: 27–58.5). The duration of the headache ranged from 10 min to 7 days. Out of 83, 27 (32.5%) had at least one SNOOP4 criterion. In all, 25 patients (30.1%) underwent neuroimaging. The sensitivity, specificity, positive predictive value, and negative predictive value of SNOOP4 were 77.8%, 73.0%, 25.9%, and 96.4% respectively.
Conclusion:
SNOOP4 criteria show very high negative predictive value for excluding serious causes of acute non-traumatic headache in adult patients presenting to the emergency department.
Introduction
Headache remains one of the most common chief complaints in the emergency department (ED).1,2 According to the World Health Organization (WHO) report in 2011, approximately 1.7%–4% of adults worldwide have headaches at least 15 days a month. 3 Non-traumatic headaches (NTHs) are well-known classified by the third edition of the International Classification of Headache Disorders (ICHD-3) into two main categories: primary and secondary headache disorders. The previous study demonstrated that the prevalence of secondary headache disorders in the ED ranged from 1% to 4.5%.2,4–7 Differentiating secondary headaches from primary headaches is an essential skill in order to prevent any morbidities and mortalities.1,8,9 Developing reproducible management strategies for headache in ED provides effective outcome. 8
International Headache Society (IHS) first launched criteria to guide physicians to send imaging in 1988. Eleven years later, Fabbrini et al. 10 reported that there were no differences in the number of imaging sent before and after IHS criteria launching. SNOOP4, which stands for systematic symptoms and secondary risk factors like cancer and HIV, neurological deficit, onset, old age, symptoms starting with P-papilledema, postural, precipitated by Valsalva and progressive, is a mnemonic for suggesting clinicians decide whether neuroimaging should be done in headache patients or not.11,12 Yet, the benefit of using this mnemonic in ED is not well established.13–15
The aim of this study was to evaluate the significance of SNOOP4 in detecting serious causes of NTH in adults presenting to ED.
Methods
Study design and setting
We conducted a prospective observational study over a period of a year between August 2017 and July 2018 in a single university tertiary hospital in the northern of Thailand which consists of 1400 patients’ bed, 151 intensive care unit (ICU) and sub-ICU beds, and 28 operating rooms with approximately 30,000 ED visits annually and provides all subspecialties including experienced neurologists and radiologists.
Study population
Eligible patients were adults who presented at the ED with a chief complaint of acute headache, which defined by the duration of headache less than 7 days prior to arrival were included in the study. Note that this was not a consecutive case recruitment in the study because, first, we do not have an official protocol to enroll case at the triage area; second, some cases who were elected into the study were not included. Both problems are due to a lack of ED personnel.
Data collection and outcome measures
After giving the information and informed consent, patients were undergoing history taking and completed physical examination following the study record form by emergency medicine resident physicians or attending staff. Exclusion criteria were (1) life-threatening events: unconsciousness, respiratory failure, shock, altered mental status; (2) previous head trauma before headache; (3) cannot giving complete information such as language barrier, congenital deafness; and (4) no informed consent. Further investigations including laboratory and radiological study and treatments were sent and managed by the findings based on patients’ history, physical examination, and pre-existing protocol. Before the collecting data period, emergency medicine resident physicians and attending staff were taught about headache, acute headache diagnosis, and treatments by attending neurologists according to the ICHD-3.
Attending radiologists (a neuroradiologist or general radiologist who routinely reports head computed tomography (CT) images), who were blinded to the study and data form but had routine clinical information, interpreted all computed tomograms. The final official report was used, although it might be created on the next day, especially when the result was done during the evenings and weekends.
To clarify, there was no official clinical practice guideline regarding acute headache management in Thailand. Physicians who encounter patients with acute NTH normally use red flag signs that have been previously published in the literature.16–22 Thus, many patients with red flag signs did not undergo a radiological study. For these patients and those who had negative findings on the investigations, we appointed them to the headache clinic of our hospital 1 week later supervised by attending neurologists to confirm diagnosis diagnosed at the ED. Furthermore, we reviewed the hospital record at 6 months to identify any missed serious diagnosis.
Terms and definitions
Primary headache disorder refers to headache, or a headache disorder, not caused by or attributed to another disorder. It is distinguished from secondary headache disorder. 13
Secondary headache disorder refers to headache, or a headache disorder, caused by another underlying disorder. In ICHD-3, secondary headaches are attributed to the causative disorder. Secondary headaches are distinguished from primary headaches. A secondary headache may have the characteristics of a primary headache but still fulfill criteria for causation by another disorder. 13 Abnormal neurological examinations defined as any abnormal examinations of nervous system including motor powers, motor tones, sensations, reflexes, cranial nerves, meningeal signs, cerebellar, and coordinating signs.
In this study, we classified patients into two groups consisting of benign and malignant groups. Benign refers to a condition that is not a life-threatening event including primary headache disorder and parts of secondary headache disorder. Malignant refers to patients with life-threatening events or potential for major morbidities and mortalities, for example, intracerebral hemorrhage, cerebral infarction, meningitis, meningoencephalitis, neoplasms.
Sample size and statistical analysis
The sample size of the study was determined according to Buderer’s formula. 23 With anticipated sensitivity of 90%, anticipated specificity of 85%, we estimated we required a sample size of about 51 patients. We used Microsoft Office Excel version 16.20 and Statistical Package for Social Sciences (SPSS) version 20 for data entry, processing, and statistical analysis at the end of the study period. We used median and inter-quartile range (IQR) for non-normally distributed continuous variables and Mann–Whitney tests to test differences. We used frequency and percentage for categorical variables and likelihood ratio to test differences. We calculated sensitivity, specificity, positive predictive values (PPVs), negative predictive values (NPVs), accuracy, and likelihood ratio of SNOOP4 red flag signs for malignant headaches, with 95% confidence intervals (CIs).
Ethical considerations
Ethics approval was obtained from Research Ethics Committee, Faculty of Medicine, Chiang Mai University (EME-2560-04692). Written informed consent was obtained from the patients for their anonymized information to be published in this article.
Results
During the study, 35,798 patients were admitted to the ED. In all, 90 patients were eligible in this study. After exclusion, 83 (92.2%) were enrolled in the analysis, count as 0.3% of populations. The reasons for study exclusion and classification for benign and malignant are shown in Figure 1. A total of 25 patients underwent head radiological examination (CT and magnetic resonance imaging (MRI)) and 9 had positive findings. The remaining were appointed at the headache clinic. We found that only 15 (20.2%) out of 74 patients followed by appointment corresponding to the protocol and all of them were diagnosed the same as ED diagnosis. After a hospital record review at 6 months, we did not find any missed serious diagnosis. For this reason, we analyzed according to the diagnosis at the ED. In all, 74 patients were analyzed in the benign group and 9 were analyzed in the malignant group (Figure 1). Of these, 63 (75.9%) were female. The mean age was 44.5 years (IQR: 27–58.5). The duration of the headache ranged from 10 min to 7 days. The characteristics of patients were well balanced between two groups (Table 1). In all, 27 patients had at least one SNOOP4 criterion. The sensitivity of SNOOP4 was 77.8% (95% CI: 40.0%–97.2%), the specificity was 73.0% (61.4%–82.7%), the PPV was 25.9% (17.3% to 36.9%), the NPV was 96.4% (88.8%–98.9%), the accuracy was 73.5% (62.7%–82.6%), the positive likelihood ratio (LR+) of SNOOP4 ⩾1 was 2.88 (1.72–4.80), and the LR+ of SNOOP4 equal to 0 was 0.30 (0.03–1.57) (Table 2). Details and characteristics of patients defined as malignant secondary headache disorders are shown in Table 3.
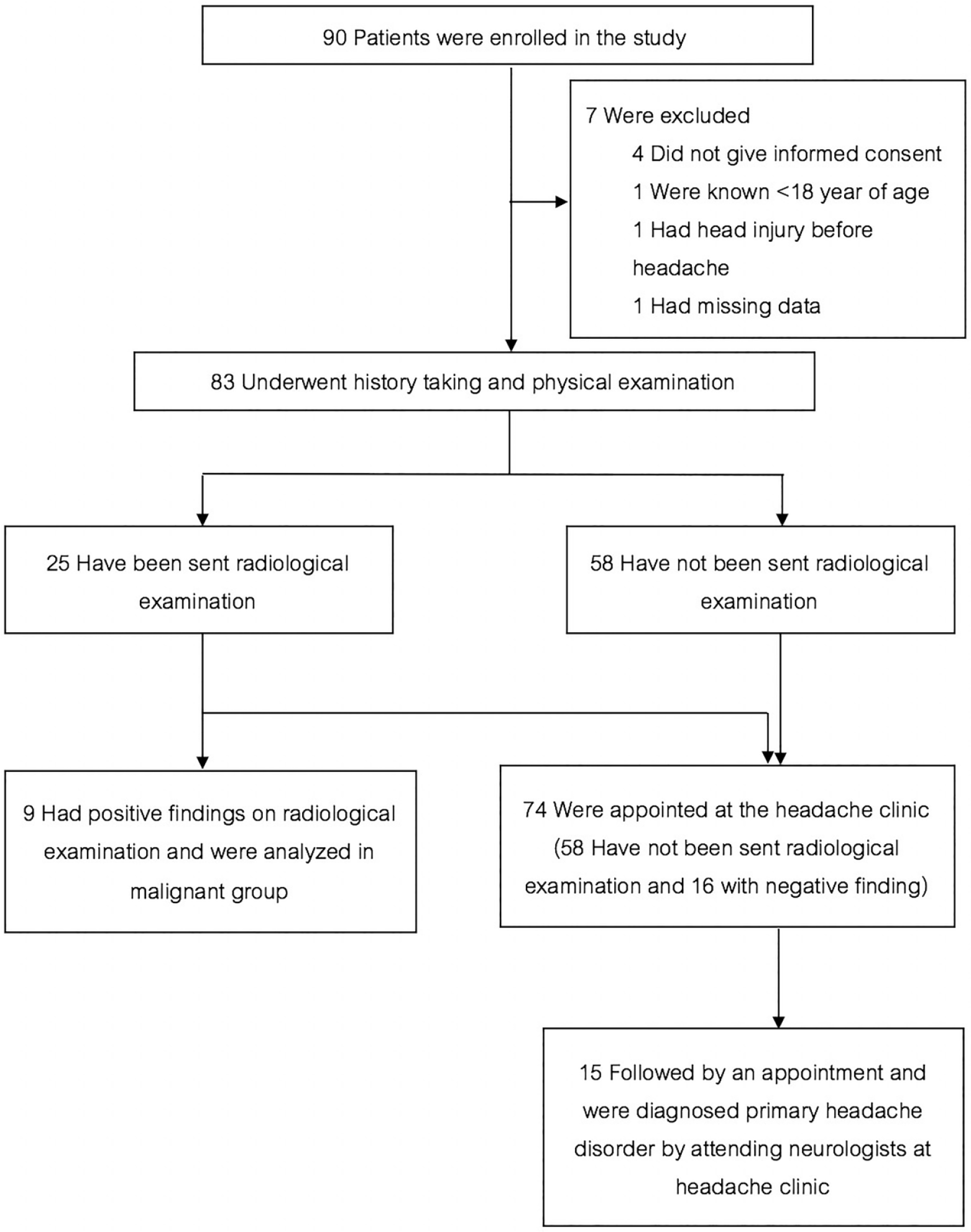
Enrollment and classifications.
Demographic and baseline characteristics of patients enrolled in the study.
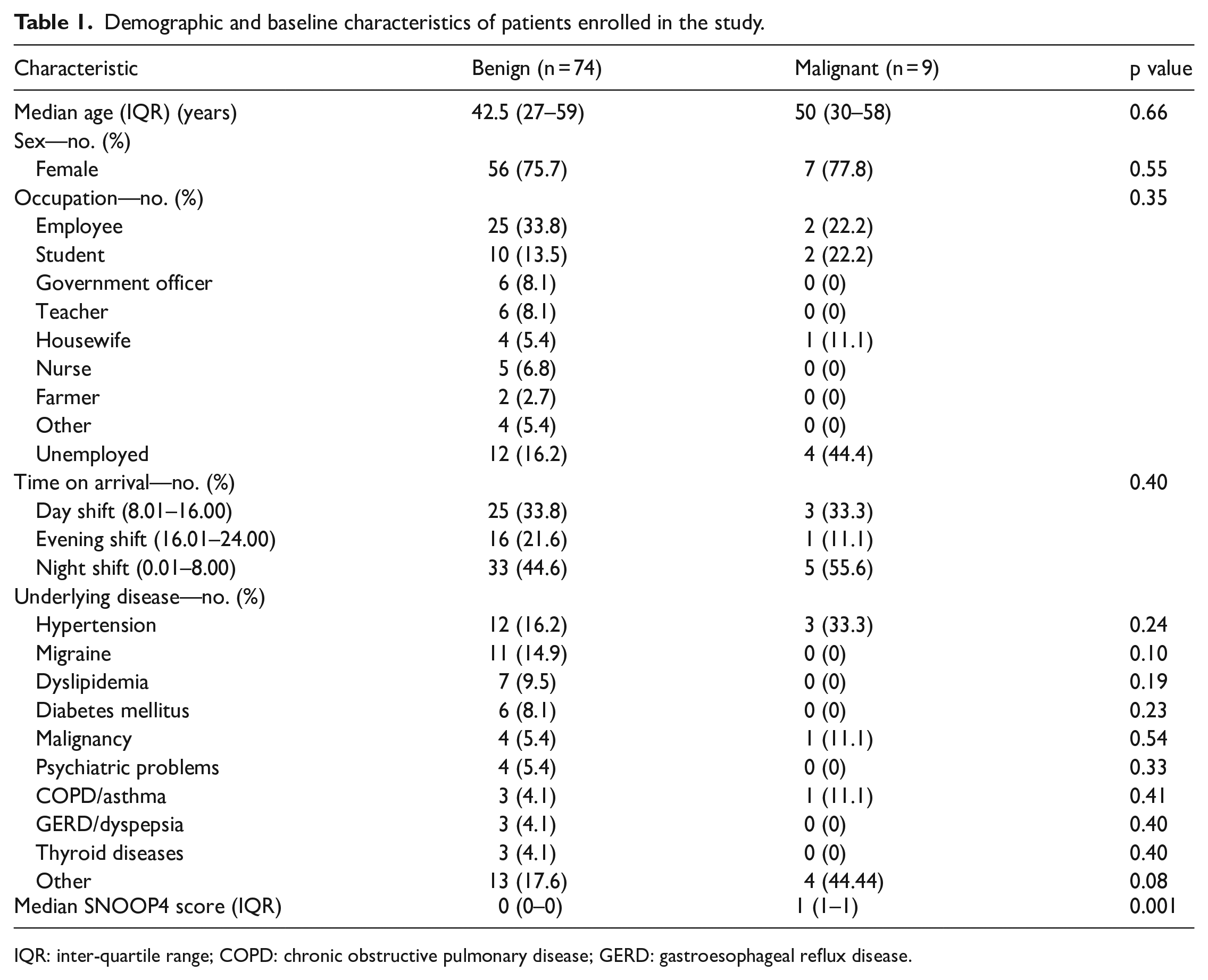
IQR: inter-quartile range; COPD: chronic obstructive pulmonary disease; GERD: gastroesophageal reflux disease.
Comparison between benign and malignant groups with SNOOP4 criteria.
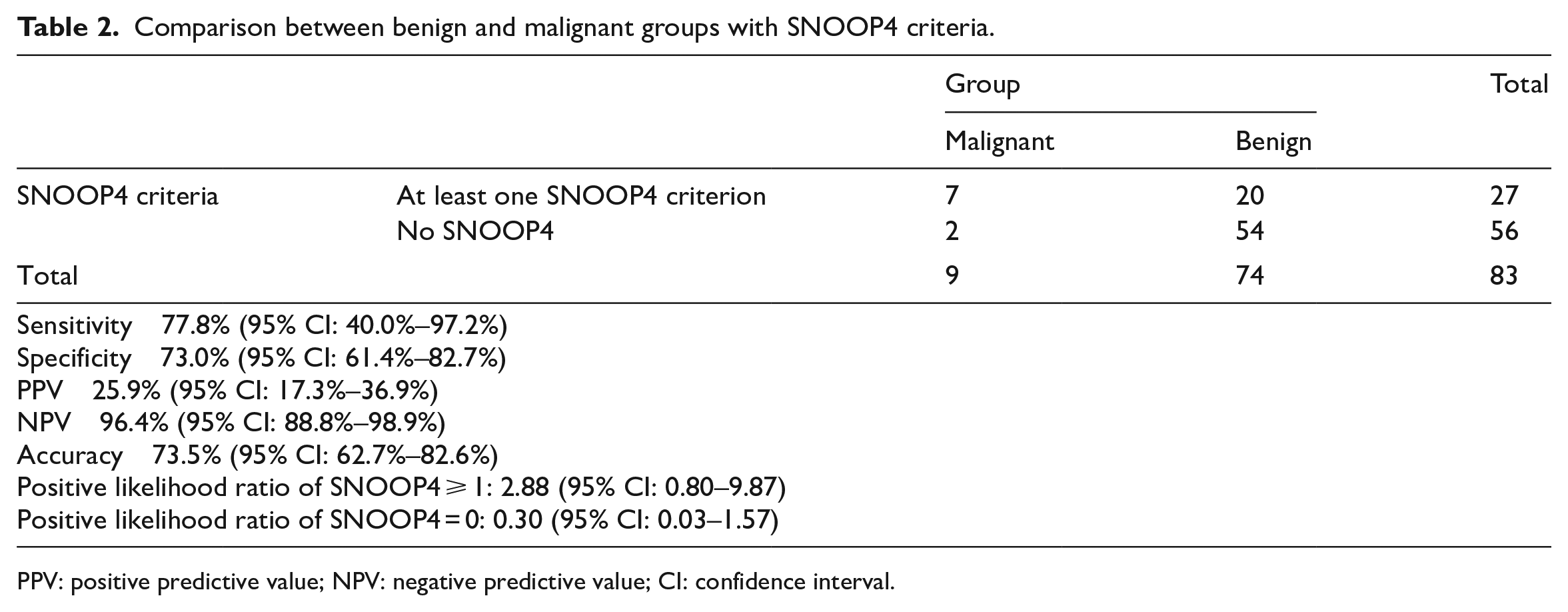
PPV: positive predictive value; NPV: negative predictive value; CI: confidence interval.
Details and characteristics of patients defined as malignant secondary headache disorders.
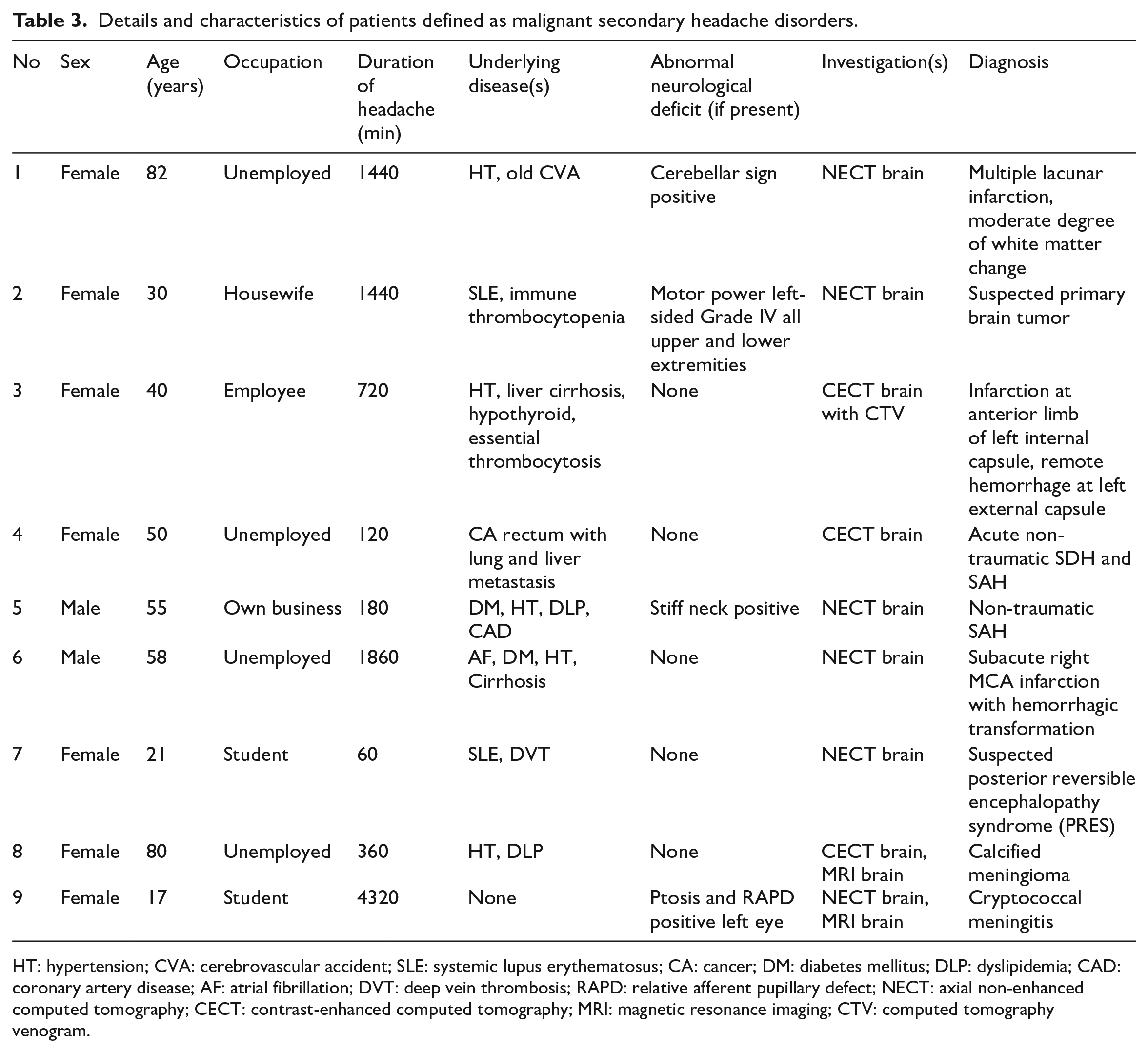
HT: hypertension; CVA: cerebrovascular accident; SLE: systemic lupus erythematosus; CA: cancer; DM: diabetes mellitus; DLP: dyslipidemia; CAD: coronary artery disease; AF: atrial fibrillation; DVT: deep vein thrombosis; RAPD: relative afferent pupillary defect; NECT: axial non-enhanced computed tomography; CECT: contrast-enhanced computed tomography; MRI: magnetic resonance imaging; CTV: computed tomography venogram.
Discussion
SNOOP4 was known as a mnemonic for detecting serious causes of NTH since 2003. 24 However, to our knowledge, there was no previous study documented any clinical applications or significance of SNOOP4. Clarke C. E. et al. conducted a prospective study over a period of 5 years at the neurology outpatient consultation service. They used red flags to determine whether a patient should undergo imaging or not and found that only 11 (2.1%) out of 530 patients who had red flag signs and underwent imaging had positive findings. 25 They concluded that even with the use of red flags, most of the results still reveal no findings. 25 Thus, assessing the predictive value of red flags is needed.
In our study, we found that SNOOP4 criteria show very high NPV in order to detect serious problems in patients presenting to the ED with NTH, despite the level of sensitivity and specificity were not high as we anticipate at the beginning. Moreover, PPV we calculated in the study was just 25.9% (95% CI: 17.3%–36.9%) corresponding to result in the previous study. 25 The sensitivity and specificity of SNOOP4 were 77.8% and 73.0%, respectively, which were quite lower than we expected. This may result from the number of patients enrolled in the study. We used 0.009 for prevalence in the formula based on the data in the first half of 2017 that 146 out of 14,051 patients presenting to the ED were diagnosed as either primary headache disorders or headache, unspecified. But, in our study, the prevalence was 0.003 which was three times lower than we calculated. Moreover, since the PPV and NPV are vulnerable to the prevalence, we calculate the likelihood ratio instead to determine whether the patient is more like to have a serious condition or not. Patients with SNOOP4 of greater than or equal to 1 were 2.88 times more likely to have serious conditions (95% CI: 0.80–9.87) (Table 2). SNOOP4 could also predict serious condition or malignant headache with a receiver operating characteristic (ROC) area of 0.75 (95% CI: 0.60–0.91) (Figure 2).
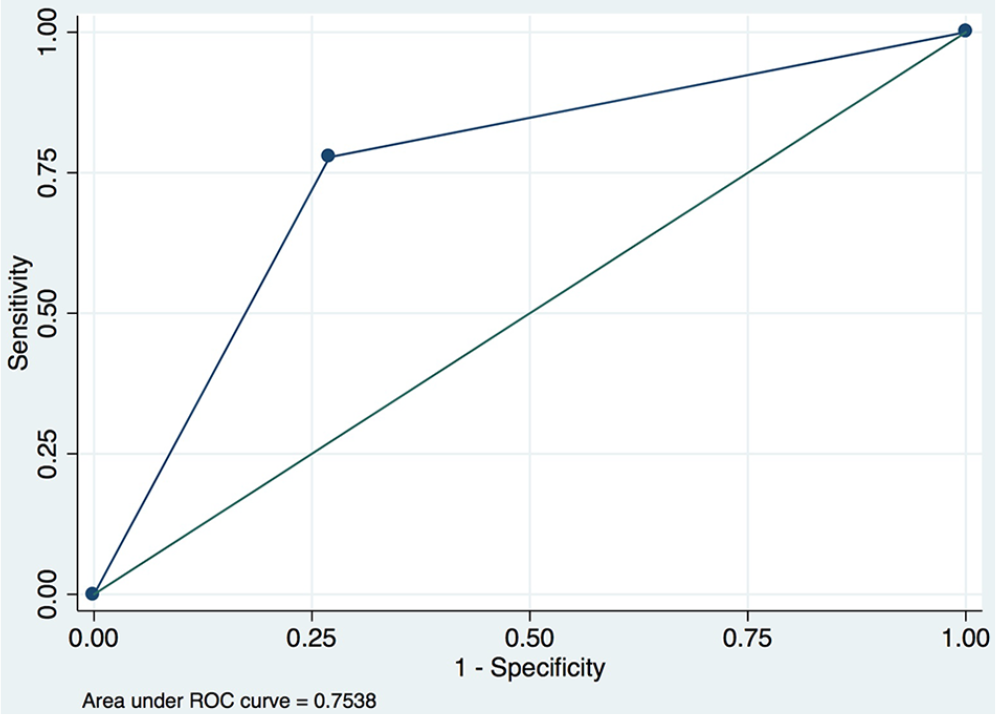
Area under receiver operating characteristic (ROC) curve of SNOOP4 with patients with malignant headache.
Clinical implications
With very high NPV and satisfactory positive likelihood ratio of SNOOP4 calculated in this study, we encourage clinicians, especially emergency physicians, to use SNOOP4 as a warning or “red flag” sign. If you encounter patients complain of headaches in the ED but had no SNOOP4 criterion, so they are less likely to have serious problems and may not necessary to send imaging. Unlike PPV, which was just 25.9%, patients who had at least one SNOOP4 criterion may not be necessary to undergo imaging; however, this may not implicate and cannot apply to all patients with NTH. Overall, the area under ROC curve was 0.75 which were in an acceptable range; thus, SNOOP4 was highly recommended to use to determine whether patients present with NTH essential for imaging or not.
Limitations
Limitations of this study were, first, this study was conducted in a single university hospital in the northern region which may not represent the whole population in the country. Second, although we designed patients who were diagnosed with primary headache disorders to follow by appointment at the headache clinic to confirm the diagnosis, only 20% of them came to the clinic. Thus, there might have been parts of patients who were in the benign group exactly were in the malignant group. However, we went further than this in that we reviewed medical records at 6 months to ensure that we did not miss any patients with serious problems. These could raise the issue of verification bias. Patients might seek alternative care or private care instead of follow-up by appointment. Third, some eligible patients were not included in this study because we did not conduct a consecutive case recruitment protocol. Finally, this study was just an initial study focused on the significance of SNOOP4 as a red flag sign; therefore, further study with a large and multicenter population is needed.
Conclusion
In summary, SNOOP4 criteria show very high NPV for excluding serious causes of acute NTH in adult patients presenting to the ED. We encourage every physician to encounter patients with NTH to use this mnemonic as much as possible.
Footnotes
Acknowledgements
We wish to thank Faculty of Medicine, Chiang Mai University, for supporting grants to present at the 18th International Conference on Emergency Medicine (ICEM).
Author contributions
W.W. proposed the study, wrote the first draft, and collected the data. W.W. and B.W. analyzed the data, read, and finally revised the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We received grants from Faculty of Medicine, Chiang Mai University, for presenting abstract at the 18th International Conference of Emergency Medicine.
Human rights
This study was performed according to the Helsinki Declaration.
Presentation(s) or awards at a meeting
Abstract was presented in the 18th International Conference on Emergency Medicine (oral presentation) on 12–15 June 2019 at Seoul, South Korea.