
Abstract
Objective
This study investigated medically unnecessary emergency medical services (EMS) transportation by comparing non-intoxicated versus intoxicated patients who did not receive emergency department (ED) treatment but utilized EMS transport.
Methods
Patients who used EMS but did not receive ED treatment were classified into non-intoxicated and intoxicated groups. Reasons for not receiving ED treatment were categorized according to whether the decision was made by the patient against medical advice or if the decision was based on a physician’s evaluation and their recommendations.
Results
There were 212 patients reviewed; 120 in the non-intoxicated group and 92 in the intoxicated group. The intoxicated group had a higher proportion of males than the non-intoxicated group. The most common cause of non-disease symptoms in the intoxicated group was assault. In the non-intoxicated group, the most common reason for the lack of ED treatment was that treatment could take place on an outpatient basis, while in the intoxicated group, the reason was lack of patient cooperation.
Conclusions
The intoxicated group was older, male and more likely to present with symptoms not related to a disease process than those in the non-intoxicated group when using unnecessary EMS transport.
Introduction
Emergency medical services (EMS) are critical for patients who are in need of emergency care and transport to the hospital. When reviewing all patients who first arrive into the emergency department (ED), the proportion of EMS transport is about 10%. 1 Unfortunately, there are times when EMS and the ED are used unnecessarily, which leads to wasted socioeconomic resources. Ideally, emergency medicine would match ‘the right source to the right patient at the right place at the right time’.2,3 Medically unnecessary EMS transportation has been investigated in several studies that were based on the hospital diagnosis and results of ED treatment.4–16 However, to date there is little evidence focusing on the patients who receive no ED treatment after the use of EMS transport. Therefore, the objective of this preliminary study was to investigate medically unnecessary EMS transports by comparing the differences between patients who on arrival were found to be non-intoxicated versus intoxicated. The study focused on individuals who did not receive treatment at the ED although they utilized EMS transport.
Patients and methods
Patient population
A retrospective review was conducted for patients who were transported to the ED via EMS, yet did not subsequently receive treatment at the ED. Data were collected for 6 months from September 2014 to February 2015 at a single academic university hospital in Ulsan (Department of Emergency Medicine, University of Ulsan College of Medicine, Ulsan University Hospital, Ulsan, Republic of Korea), which is located on the southeast coast of South Korea. In this region of South Korea, the local fire departments are responsible for 119 (emergency contact number in South Korea) responses and transportation from each scene to hospital. As an alternative to seeking an ED, some outpatient clinics are operating during the weekday night-times and the afternoons at the weekends. However, most patients using EMS transport in South Korea are transported to the ED and not to the outpatient clinics.
This study was approved by the relevant institutional review board (no. UUH-IRB-2015-04-001) at Ulsan University Hospital, Ulsan, South Korea. Written or verbal informed consent were exempted due to the retrospective nature of the study.
Data collection
The EMS run sheets that were submitted to the hospital after transportation were retrospectively reviewed. Data were excluded if the run sheet was not submitted to the hospital, the run sheet was unreadable, or the patient was treated at the ED after transportation. All the EMS run sheets had the same format. Data were collected and several different categories were analysed: general demographics, clinical demographics, prehospital treatment and reason for lack of treatment in the ED. The general demographics that were collected included: agency who performed the prehospital treatment and transport, age, sex, time, day of EMS use, elapsed time from EMS call to scene and EMS call to hospital ED, occupation of patient, location from which the call was placed. Age and time of EMS use were classified later into subgroups. Clinical demographics that were recorded included: past medical history, list of symptoms (later categorized as disease or non-disease related), vital signs, level of consciousness, pupil light reflex and glucose level. Symptoms were recorded as disease or non-disease on the run sheet by the fire fighters, so the study used the classification of symptoms based on the information on the run sheet. Prehospital treatment data that were collected included airway intervention, oxygen, electrocardiogram cardiac monitor, intravenous line, drug use, immobilization, wound care, adjuvants to keep a patient warm or cool, automated external defibrillator monitor, direct medical control contact, number and qualifications of the riding fire fighters.
Reasons for no ED treatment
Reasons for not receiving ED treatment were further divided into two groups: (i) those patients who made this decision against medical advice; and (ii) patients who did not receive treatment based on a physician’s evaluation and their recommendations. Details of those patients that went against medical advice were classified into: (i) refusal to receive treatment; (ii) uncooperative; (iii) wanted to transfer to another hospital; (iv) received outpatient treatment. Details of the recommendations made after a physician’s evaluation were classified into: (i) no symptoms at ED arrival; (ii) intoxication without trauma or medical problems; (iii) can be treated by a primary care physician or at another hospital; (iv) repeated visits with the same symptoms. Patients were separated into those who were under the influence of alcohol versus those who were not.
Statistical analyses
All statistical analyses were performed using the IBM SPSS® statistical package, version 20.0 (IBM, Armonk, NY, USA) for Windows®. To investigate whether alcohol intoxication affected the unnecessary EMS transport or not, comparison of general, clinical demographics, prehospital treatment and reasons for lack of ED treatment were performed between the non-intoxicated and intoxicated group using χ2-test, Fisher’s exact test and Student’s t-test. A P-value < 0.05 was considered statistically significant.
Results
General demographics of patients with or without alcohol intoxication who did not receive emergency department (ED) treatment although they were transported to the ED using emergency medical service (EMS) transport.

Data presented as mean ± SD or n of patients (%).
χ2-test, Fisher’s exact test and Student’s t-test.
NS, no significant between-group difference (P ≥ 0.05).

(a) Unnecessary emergency medical service (EMS) transport was provided by all the local fire departments. (b) Unnecessary EMS transport occurred most frequently from the two fire departments (arrows) nearest to the study hospital especially for intoxicated patients (black bar). The colour version of this figure is available at: http://imr.sagepub.com.
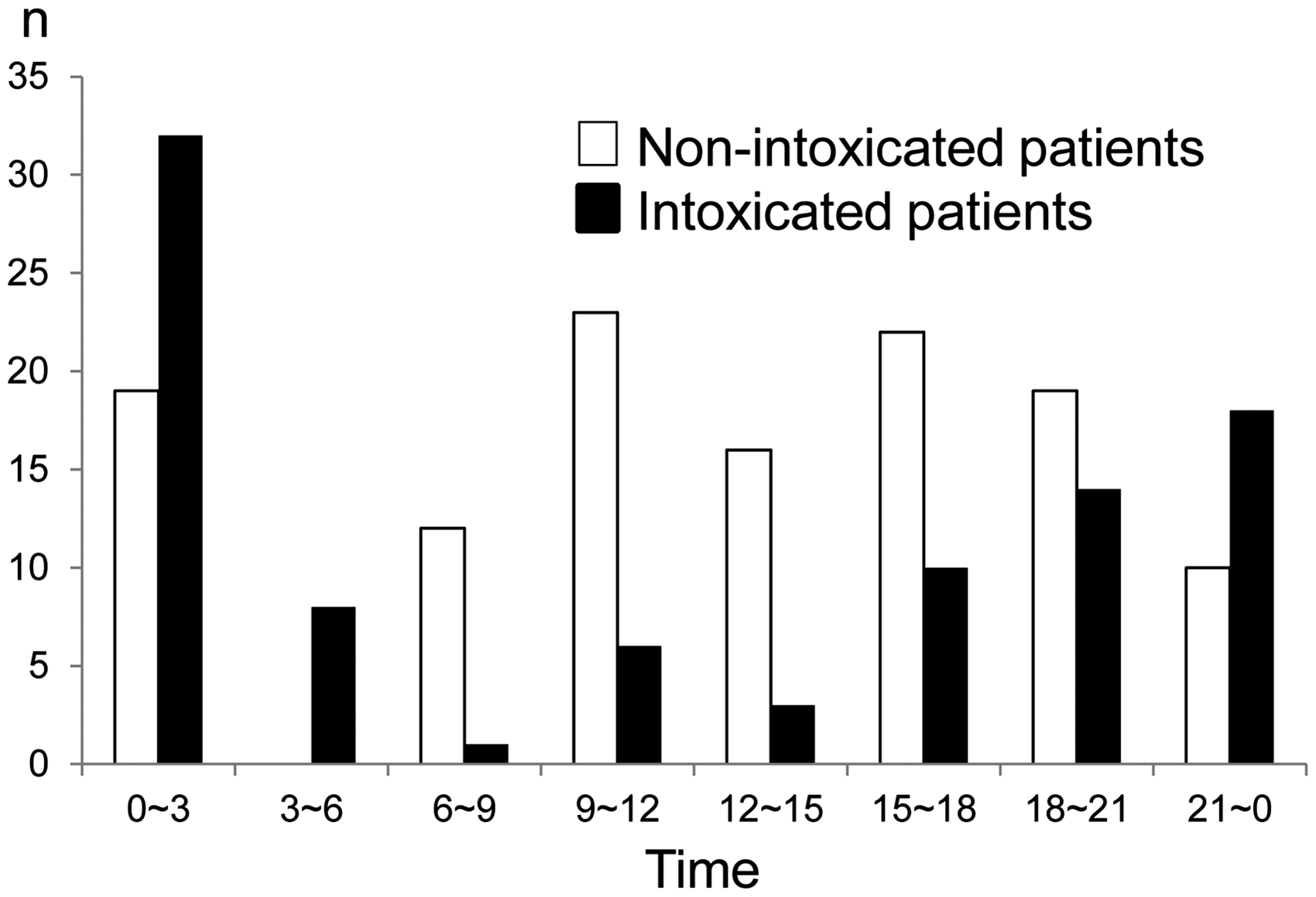
Time of day that the call for emergency medical service (EMS) transportation was made by non-intoxicated and intoxicated patients who used EMS transport but had no treatment at the emergency department.
Clinical demographics of patients with or without alcohol intoxication who did not receive emergency department (ED) treatment although they were transported to the ED using emergency medical service transport.

Data presented as n of patients (%).
χ2-test.
NS, no significant between-group difference (P ≥ 0.05).
Clinical characteristics of patients with or without alcohol intoxication who did not receive emergency department (ED) treatment although they were transported to the ED using emergency medical service transport.

Data presented as mean ± SD or n of patients (%).
No significant between-group difference (P ≥ 0.05).
Prehospital treatment of patients with or without alcohol intoxication who did not receive emergency department (ED) treatment although they were transported to the ED using emergency medical service transport.

Data presented as n of patients (%).
P < 0.001 compared with the non-intoxicated group; χ2-test.
AED, automated external defibrillator; EMT, emergency medical technician.
Causes of no emergency department (ED) treatment in patients with or without alcohol intoxication who did not receive ED treatment although they were transported to the ED using emergency medical service transport.
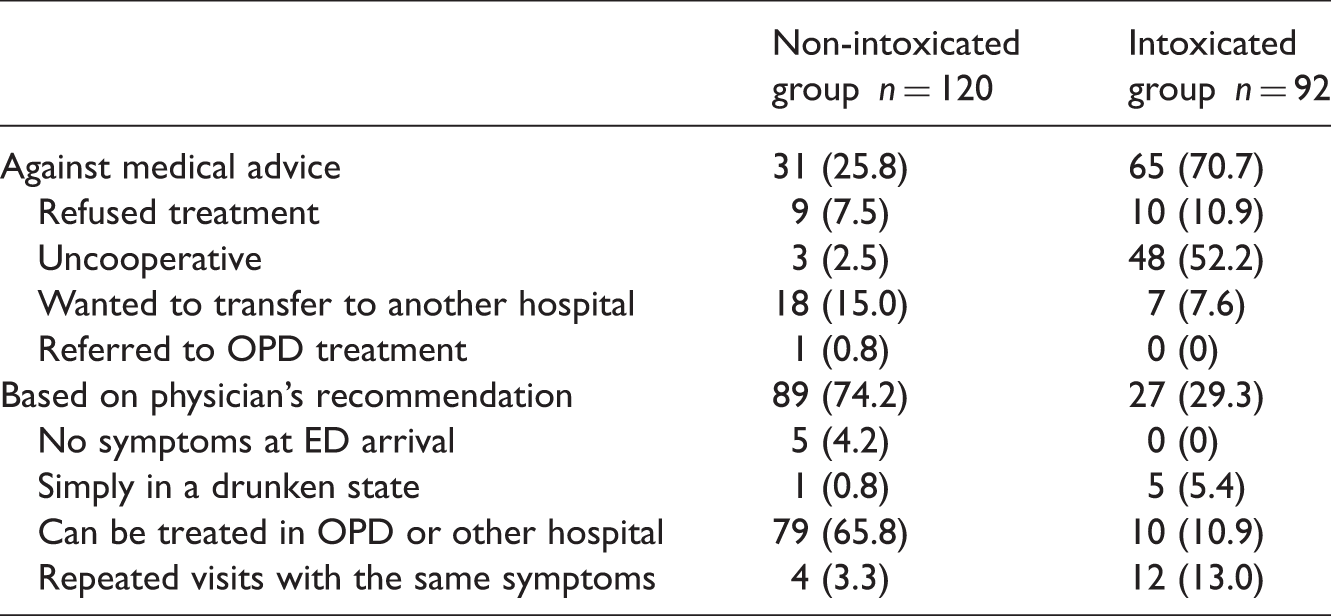
Data presented as n of patients (%).
The main reason for the lack of ED treatment was significantly different between the two groups (P < 0.001); χ2-test.
OPD, outpatient department.
Discussion
To the best of our knowledge, this is the first study that has investigated patients who get transported by EMS to the ED, but then do not receive treatment. There are several studies that have investigated unnecessary EMS transportation,4–16 but most of them were based on the ED diagnosis or the results of the ED treatment. One study showed that the ED diagnosis was inappropriate as a criterion for evaluating the medical necessity of EMS transport. 12 By using an ED diagnosis to identify patients for a study of medically appropriate EMS use you may be missing a significant amount of important data. For example, some patients leave prior to being seen by a physician and therefore do not receive a diagnosis, while others do not receive treatment due to their personal choice to leave against medical advice prior to full evaluation and testing.
This present study demonstrated that the proportion of the patients who did not receive ED treatment against medical advice was 45% (96/212) overall. When comparing those who were not intoxicated with those who were intoxicated, it was 26% versus 71%, respectively. In South Korea, all intoxicated patients must not be discharged if the attending physician believes that the patient needs to be treated urgently. However, if a patient appears to present with intoxication alone or they have a minor complaint that does not necessitate immediate treatment, then medical providers do not need to enforce this rule. In South Korea, the decision as to whether or not an intoxicated patient needs to be treated in the ED is not based on obtaining a blood alcohol level, but on the physician’s judgement. It should be noted that when reviewing patients who did not receive ED treatment due to a decision they made against medical advice, in South Korea, there is a general policy that they would not be discharged if the physician feels that the patient has an urgent need to be treated. Therefore, all of the causes of no ED treatment that were classified into the ‘against medical advice’ category in this study can be defined as unnecessary EMS transport.
Drinking alcohol can cause medical problems as well as many socioeconomic losses.15,17–19 Patients who are intoxicated tend to use EMS transport and visit the ED more frequently than the general population.20,21 Many people utilized the EMS resources unnecessarily in an intoxicated state, with the intoxicated group accounting for 43% of all patients (92/212) in this study. Intoxicated patients who have been assaulted have an even higher utilization of EMS resources overall. 22 Among those patients considered to have symptoms not associated with a disease process, 40% in the intoxicated-group and 5% in the non-intoxicated group presented as a result of assault in the present study. This previous evidence, along with the current findings, lead us to believe that alcohol intoxication and assault play a key role in the overuse of EMS transport.20–22
Individual patients are not charged for EMS transportation and prehospital treatment provided by the local fire departments in South Korea, as is the case in many other countries.23,24 This may lead to excessive use of EMS and unnecessary EMS transportation. In South Korea, the 119 dispatcher or the emergency medical technician has the right to refuse to transport a patient if they believe that the patient does not need EMS transportation, but in reality many providers are afraid to make the wrong decision and EMS transportation is deployed. This is one of the many obstacles in the attempt to reduce unnecessary EMS transportation, as well as the large proportion of the population who consume alcohol in excess. Ideally in the future, prehospital patients found to be intoxicated alone without any medical or traumatic problems may be considered not suitable for EMS transportation if guidelines can be clearly outlined and EMS providers are given appropriate training.
This present study had several limitations. First, it was conducted retrospectively in a single university academic hospital. Therefore, the findings might not be generalizable to a larger population. Secondly, the data collected were based on fire fighters’ run sheets alone and not from a direct interview with the patient in the ED. Also, the reasons for the lack of ED treatment was investigated only by analysing the information on the run sheets, therefore data may have been misclassified. However, the study attempted to decrease this error based on prior experience of treating patients in the study hospital. Direct follow-up interviews with the EMS provider who wrote the report would have improved the accuracy of the data, but was not performed. Thirdly, a review of all of the run sheets was not performed, so the study was not able to compare the characteristics of patients who did receive ED treatment with those who did not receive ED treatment. Larger prospective multi-centre studies that complement the above findings will be helpful to evaluate the accuracy of this present description of unnecessary EMS transport.
In conclusion, this is the first study to investigate the unnecessary utilization of EMS transport based on patients who did not receive treatment in the ED. The intoxicated group was typically older males who presented with symptoms not related to a disease process when compared with those in the non-intoxicated group. The most frequent cause for not receiving ED treatment in patients transported by EMS was the physician’s recommendation in the non-intoxicated group and the patient’s decision to leave against medical advice in the intoxicated group. This present study has identified a need for education of the community surrounding Ulsan, South Korea. Two programmes will need to be created and delivered: (i) one should include education surrounding alcohol abuse, covering the dangers, and recognition and identification of avenues for assistance in alcohol control; and (ii) a second that is targeted at the general population regarding the appropriate use of EMS and ED for medical care. Applying a charge for EMS transportation might need to be considered as a way to reduce unnecessary EMS transportation in South Korea. EMS systems outside of South Korea might also be able to reduce unnecessary EMS transportation by adopting comprehensive guidelines for EMS transport and having well-trained EMS personnel, as well as by providing the aforementioned public educational initiatives.
Footnotes
Acknowledgements
All the authors would like to acknowledge the review of Dr Donna Carden, professor, Department of Emergency Medicine, University of Florida, Gainesville, FL, USA.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.