
Abstract
Objectives:
Endotracheal intubation is an essential skill of every emergency department clinician. The current practice of emergency intubation in the emergency departments in China and its safety is largely unknown. This study aimed at evaluating the practice and the safety profile of emergency intubation in an emergency department in Shenzhen.
Methods:
This study was of retrospective design. It was conducted in the emergency department of a university affiliated hospital. All patients requiring emergency intubation from 1 January 2017 to 30 June 2018 were recruited. Data on demographic and clinical characteristics of patients and characteristics of intubations were collected and analyzed.
Results:
A total of 128 patients were analyzed. Patients with spontaneous intracerebral hemorrhage were most common. Airway protection for patency was the most common indication of intubation. Most intubations were performed by emergency department staff with direct laryngoscopy. The first attempt success rate was 93.8%. Serious adverse events were rare.
Conclusion:
The practice of endotracheal intubation in the emergency department is in line with international ones. The safety profile is good. A national registry of emergency airway management is recommended.
Keywords
Introduction
Endotracheal intubation is a skill that should be mastered by every clinician working in the emergency departments (EDs). Studies on the practice of endotracheal intubation in the ED have been published from around the world.1–3 It was found that endotracheal intubation was most commonly done for medical patients. Emergency physicians performed most of them, and with a high first-attempt success rate. Over the years, the use of videolaryngoscopy has been rising. In China, despite the publication of airway management guidelines or consensus on emergency airway management,4,5 there is no study that describes the practice of endotracheal intubation in the ED in the country. This study thus aimed to investigate the practice and safety profile of emergency endotracheal intubation in an ED. It is hoped that the findings of this study can inform ED leaders in China on the current practice of emergency intubation and provide benchmark data for audit purpose.
Methods
This was a retrospective observational study conducted in the ED of the University of Hong Kong—Shenzhen Hospital (HKUSZH). Its ED has an annual census of about 170,000, of which 23% are critical or emergent patients. The ED is distinct from other ED in China in that it is an accredited training center of the Hong Kong College of Emergency Medicine and adopts the Hong Kong system of practice and training. All patients would be first managed by the ED staff who are trained or being trained in Emergency Medicine. Airway management workshops are conducted regularly. Departmental guidelines on airway management and rapid sequence induction (RSI) are in place.
The study period was from 1 January 2017 to 30 June 2018. Patients of all ages, who required emergency endotracheal intubation in the ED, were recruited. Patients transferred from other hospitals or who had been intubated before ED arrival were excluded. Data were collected from the ED and hospital records and included demographic variables of patients, their chief complaints to ED, and the principal diagnostic categories on discharge, indication for intubation, whether patients had a difficult airway, number of attempts of intubation, specialty of staff doing the intubation, type of laryngoscopy, medications used for intubation, mean arterial pressure (MAP) and pulse rate just before and 5 min after intubation, and complications in terms of equipment failure, wrong placement of endotracheal tube as confirmed clinically and by end-tidal CO2 measurement, mechanical trauma during intubation, barotrauma (pneumothorax), and hemodynamic disturbance. The indication of intubation was determined by two investigators on the basis of the clinical notes. The most important one was chosen. Judgment of difficult airway was also by two investigators who independently reviewed the clinical records or interviewed the attending doctor. An airway would be considered difficult if there was anatomical obstruction of the airway or restriction of neck mobility from whatever cause. There might be more than one causes of difficult airway in one patient. The diagnostic category was based on the International Classification of Diseases, 10th Revision (ICD-10).
Descriptive statistics were used for analysis. Significant testing was by chi-square test for comparison between categorical variables and dependent t-test for paired samples. A p-value less than 0.05 was considered significant. Statistical analysis was performed by SPSS (Version 23; SPSS, Chicago, IL, USA). Ethical approval had been obtained from the local institutional review board. Patient consent was waived because no patient identifiers were disclosed and the diagnosis and management of patients would not be affected.
Results
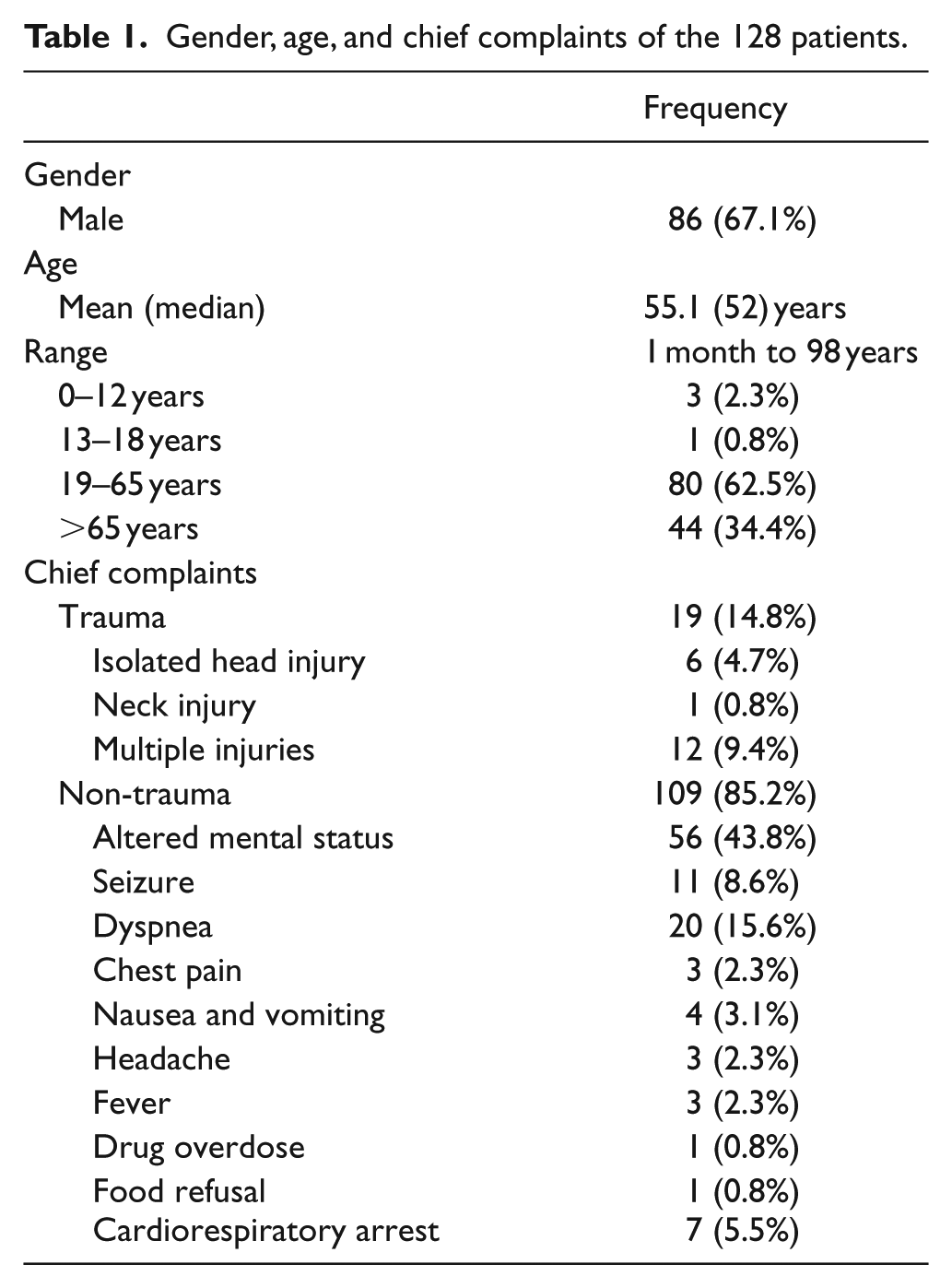
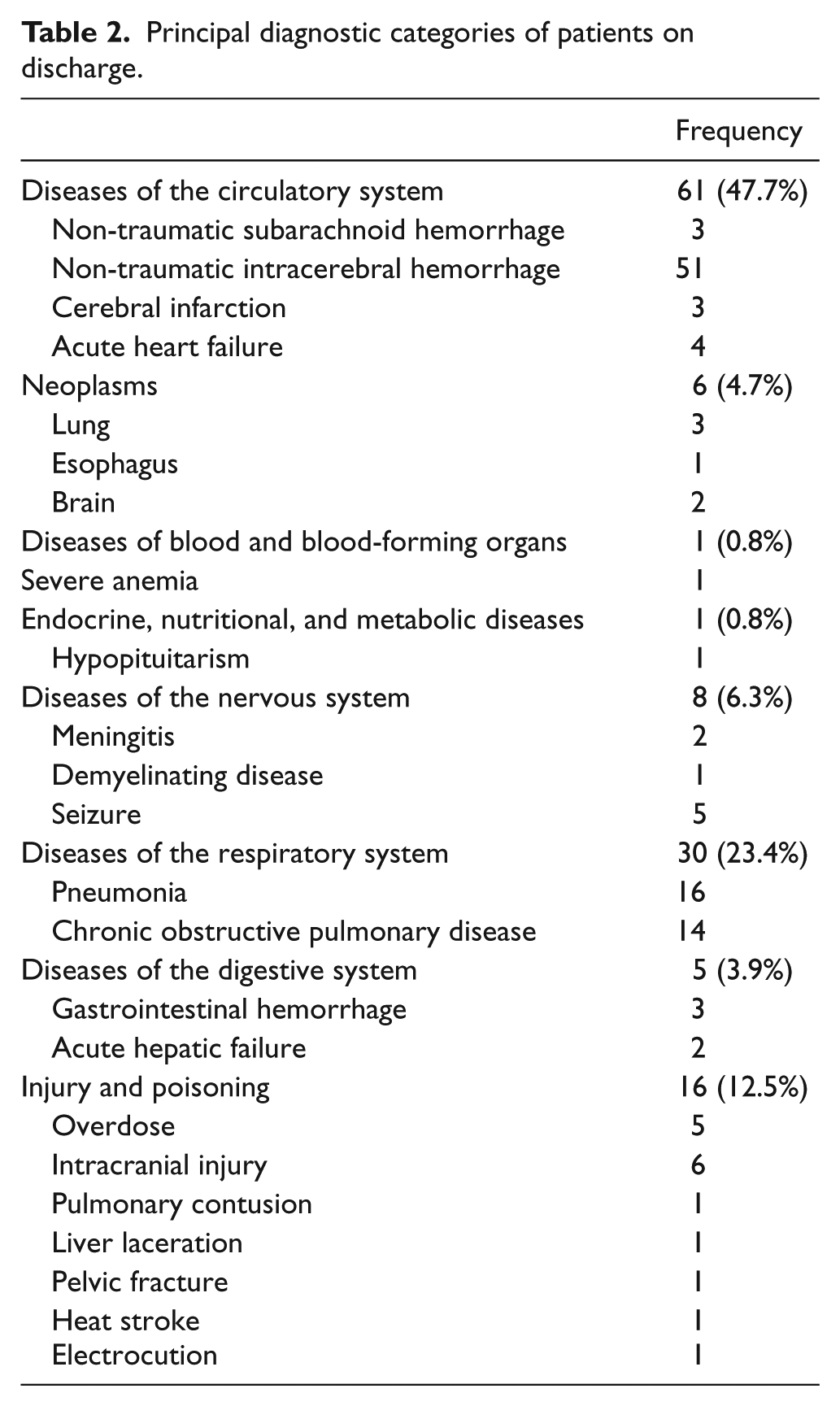
During the study period, 137 patients required emergency intubation in the ED. There were nine cases with incomplete record. Thus, 128 patients were included for analysis. Their age ranged from 1 month to 98 years. Of these 128 patients, 19 (14.8%) attended the ED for traumatic causes. Their chief complaints are shown in Table 1. The top three diagnostic categories of patients requiring emergency intubation were diseases of the circulatory system (47.7%), diseases of the respiratory system (23.4%), and injury and poisoning (12.5%). The most common diagnosis was non-traumatic intracerebral hemorrhage (Table 2).
Gender, age, and chief complaints of the 128 patients.
Principal diagnostic categories of patients on discharge.
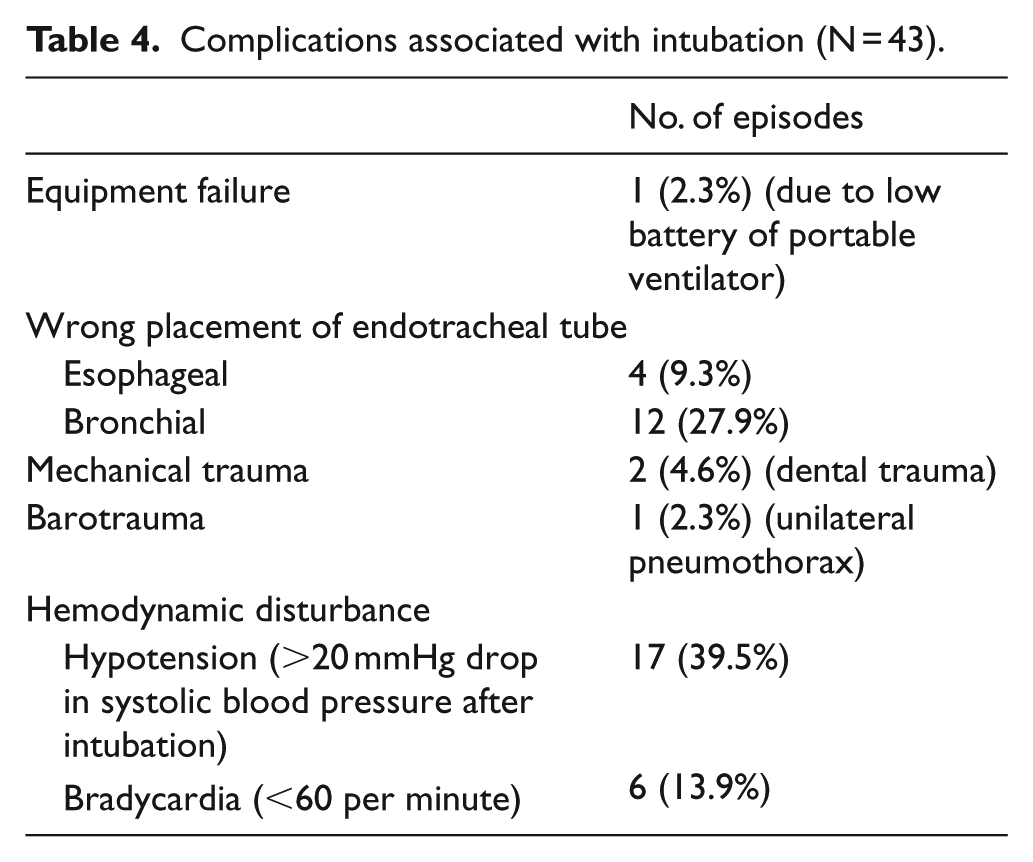
Excluding the cases of cardiorespiratory arrest, endotracheal intubation was mainly performed for maintaining airway patency (N = 87, 68%). Patients judged to have a difficult airway were not common (12.5%). The most common cause leading to a difficult airway was restriction of neck movement. The success rate of first attempt was high (93.8%). The majority of intubations were done by ED staff. Most (93%) were done with conventional, direct laryngoscopy. There was no significant difference in first-attempt success rate between direct and videolaryngoscopy. RSI was used in all patients except the seven patients in cardiorespiratory arrest. Etomidate and suxamethonium were the most commonly used induction agent and paralytic agent, respectively (Table 3). Concerning complications, there were 43 episodes of adverse events among the 136 intubations. Most adverse events were mild (Table 4). The most common adverse event was a drop in blood pressure after intubation. However, no statistically significant difference in MAP and pulse rate before and after intubation was observed (Table 5).
Characteristics of the intubation attempts.
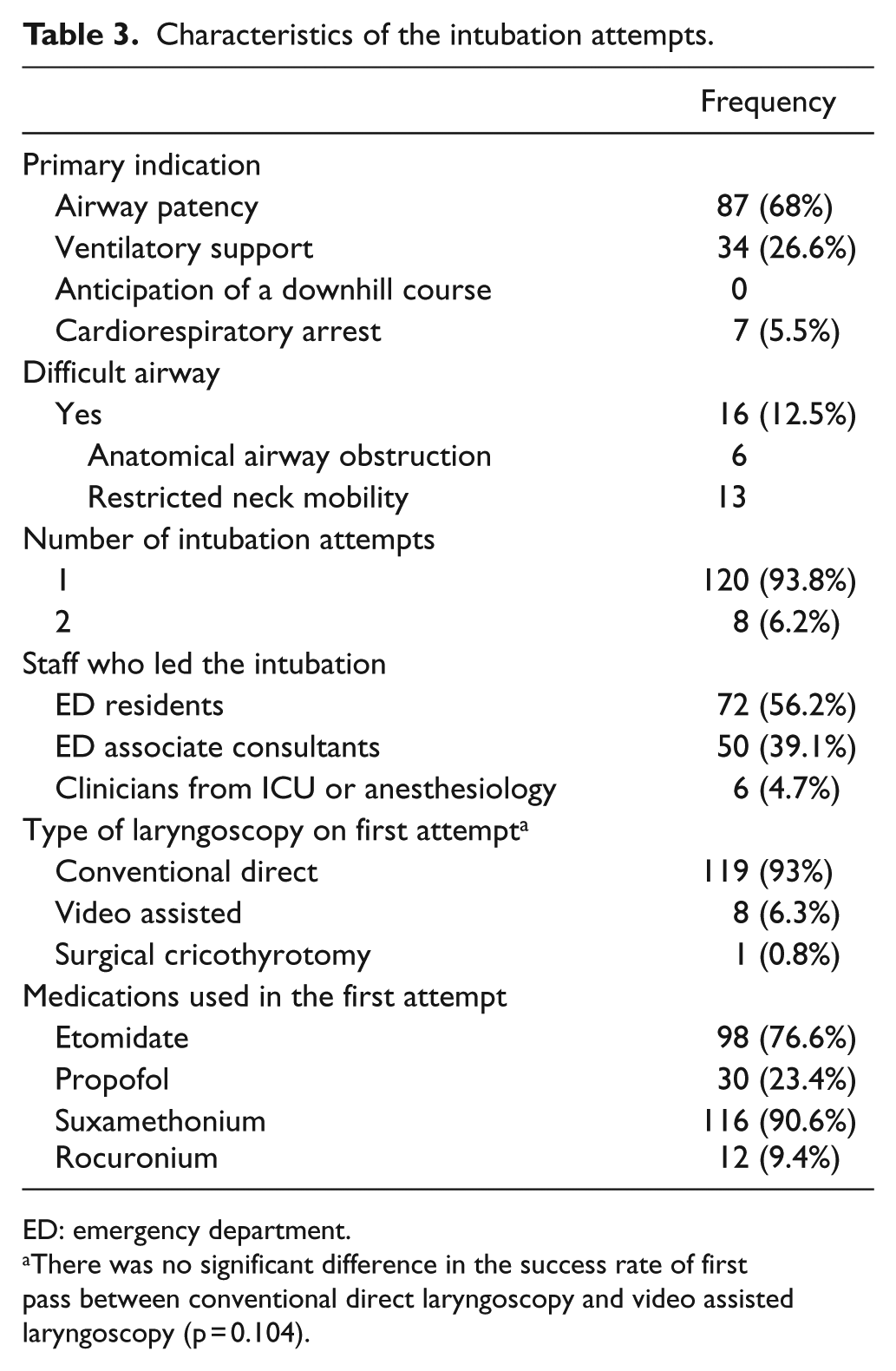
ED: emergency department.
There was no significant difference in the success rate of first pass between conventional direct laryngoscopy and video assisted laryngoscopy (p = 0.104).
Complications associated with intubation (N = 43).
MAP and pulse rate before and after intubation.

MAP: mean arterial pressure; CI: confidence interval.
Discussion
This study provides an overview of the practice and safety profile of emergency intubation in an ED in China. The findings show that the ED staff had to manage the airway of patients of the whole age spectrum, from neonates to the elderly. Because of the unique anatomical and physiological characteristics of children, management of the pediatric airway requires skills different from those of adults. In this study, there were only four patients below the age of 19. This highlights the importance of regular in-service training regarding pediatric airway management lest drop in competence due to rarity of the pediatric presentation. Most patients in need of emergency intubation had a medical complaint. This is in line with studies elsewhere.1,6 During the study period, there were only 19 trauma patients requiring emergency airway management in the ED that is about one patient per month. Similar to pediatric patients, the airway of a trauma patient should be considered a difficult one by default. The importance of regular training cannot be overemphasized.
Among the 128 patients in this study, 51 of them had spontaneous intracerebral hemorrhage. Very often these patients would have impaired consciousness, thus putting them at risk of loss of airway patency. This is reflected by the finding that the most frequent primary indication for intubation was protection for airway patency. The other common indication for endotracheal intubation found in this study was for ventilatory support. With the increasing use of non-invasive ventilation in the ED, invasive means of ventilatory support like endotracheal intubation is expected to decrease. 7 It needs a study of longer duration to prove it, nonetheless.
Management of difficult airway is always a challenge to the ED clinicians. In this study, two criteria were used to define a difficult airway. In fact, there are many contributory factors. For example, lack of past medical data, which is not uncommon among critical ED patients, may make airway assessment difficult. The incidence of difficult airway of 12.5% in this study is probably an underestimate if all factors, staff, patients, and environment, are considered.
The first-attempt success rate of endotracheal intubation of 93.8% was high. This study was not designed to examine the causes of success rate. In general, there is evidence that prior experience of intubation is a more important factor of first-attempt success rate than simply seniority of ED staff. 6 Further study is required to elucidate factors affecting the success rate of intubation in the local ED setting.
ED clinicians intubated 122 out of 128 patients in this study. This implies that the ED clinicians in this hospital have been playing a key role in emergency airway management. In the past, emergency airway management was thought to be the expertise of anesthesiologists or intensivists. This study suggests that ED clinicians, who specialize in Emergency Medicine, should and can take a leading role in taking care of their own patients’ airway.
Use of videolaryngoscopy was not common as revealed in this study. Most studies about the usefulness of videolaryngoscopy were from anesthesia practice, and the findings may not be applicable for ED patients. A systematic review published in 2016 suggested that videolaryngoscopy provide a better view of the glottis and has a lower failure rate. But it also emphasized the importance of training before promoting the use of videolaryngoscopy. 8 This study did not show an advantage of using videolaryngoscopy over direct one in first-attempt success rate. A bigger sample, while controlling patient and disease characteristics, is necessary to elucidate whether there would be any real difference.
Every ED medical staff of HKUSZH is required to be familiar with RSI. It is therefore not surprising to find that RSI was a common procedure in intubation. Most used the combination of etomidate and suxamethonium. For critically ill patients, however, there is an increasing trend of using ketamine instead of etomidate, and rocuronium instead of suxamethonium. 9 Revision of practice guidelines may be needed when more evidence appear.
The safety profile of emergency endotracheal intubation in the ED of HKUSZH was good. Except the case of unilateral pneumothorax that required immediate tube thoracostomy, most of the 43 episodes of adverse events were easily recognizable and reversible. This is likely a result of regular airway management training for the ED staff.
Limitations
This is a single-center study. The findings may not be generalizable to other ED in China. The study is retrospective in design, and data were not entered contemporaneously. Despite efforts to ensure data accuracy, there may be recall bias affecting data entry and interpretation. To overcome these limitations, a national registry of emergency airway management with prospective data collection is recommended.
Conclusion
ED clinicians are able to manage emergency intubation with a high first-attempt success rate. Most patients requiring intubation are adults with non-trauma presentations. Direct laryngoscopy and RSI are commonly used. The safety profile is good with few serious adverse events. Overall, the local practice of emergency intubation in the ED is in line with international ones. To get a better understanding of ED airway management, a national registry is recommended.
Footnotes
Author contributions
All authors are responsible for conception and design of the study. W.X.Y. is responsible for data collection and assembly. K.L.F. and L.P.L. are responsible for data analysis. The manuscript was written and approved by all authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The dataset for this study is available from the corresponding author.
Ethical approval
Approval had been obtained from the local institutional review board.
Human rights
There is no concern of human right issue as the study is a retrospective observational study only.
Informed consent
Informed consent from patients had been waived by the institutional review board because there was no change in patient management and patient identifiers were delinked from analysis.
Patient consent
Patient consent was waived because no patient identifiers were disclosed and the diagnosis and management of patients would not be affected.