
Abstract
Objective
To identify significant risk factors associated with repeat emergency department (ED). Visits for violent injuries in youth firearm victims.
Methods
The study subjects of this retrospective cohort study were firearm victims aged 18 and younger presenting to a Pediatric Emergency Department/Trauma Center at Children's Hospital of Wisconsin between 1990 and 1995. The primary outcome was subsequent Emergency Department visits (REDV) at any emergency department in Milwaukee for a violent injury.
Results
A total of 495 subjects were eligible for the present study in the pediatric firearm victim's ED visit database. Eighty-five percent (n = 420) were males and 82% were African-Americans. Mean age was 15 years old (s.d = ±3.6). A majority of them had a single-parent family. Eighty-eight subjects (17.8%) had a prior history of ED visit due to violence. During the study time, 201 subjects had at least one REDV. In the multivariable model, a subject without a social worker consulting at the hospital were more likely to have REDV compared to subjects with a social worker consulting (O.R = 1.749; p-value = 0.047), controlling for guardian and disposition. Subjects disposed to detention center or police custody were more likely to have REDV compared to subjects disposed to home or a hospital (O.R = 5.351; p-value = 0.003).
Conclusion
Our analysis indicates that individuals with guardians, those who did not receive social worker intervention on their initial visit, and those discharged in police custody were associated with increased repeat ED visits due to a violent injury.
Introduction
Fatal and nonfatal firearm-related injuries remain an important public health issue in the U.S. 1 2 The pediatric and adolescent age group has the fastest rate of increase in incidence of fatal gunshot wounds. 3 In 2002, more than 877,700 young people ages 10 to 24 were injured from violent acts and approximately 1 in 13 required hospitalizations in the U.S. 4
Studies of intentionally injured adults and youth presenting to emergency departments noted a high rate of repeat intentional injury. Those initially admitted for treatment of assault were found to be at greater risk of subsequent treatment for assault than those admitted for noninjuries.5–9 In addition to direct medical cost by the government, insurance companies, and other private sources, impact on family work and finances is costly.10,11 Cutting and piercing wound survivors were 7 times more likely to be recidivists than were gunshot survivors. 7 The incidence of recurrent trauma was highest in men, blacks and the uninsured 8 and positive blood alcohol levels, and longer hospital stays were also significantly associated with recidivism. 12 The recurrent rate of urban trauma as a chronic disease was estimated 35%–44%3,8 with a 20% 5-year mortality rate. 9
Medical, public health, and legal professionals as well as policy-makers are aware of the personal and environmental factors related to adolescent victims of interpersonal violence. Injury literature enumerates victimization risk and protective factors and some compare socioeconomic, familial and individual influences to each other.13–15 Cheng et al. found that fighting was common among all groups that she studied: unintentional injury, violent injury and noninjured youth, but that youth who had endured past fights, past fight injuries, and seeing someone else shot were markers associated with assault injury. 12
In order to develop strategies to prevent repeat violent injuries among youth, it is important to understand the risk factors for another violent injury. However, little is known about these characteristics among pediatric firearm victims. This analysis was undertaken to investigate significant individual and environmental risk factors associated with repeat ED visits for violence among adolescents. Understanding and addressing these factors will enable practitioners and health systems to develop targeted strategies to prevent repeat visits for intentional injuries.
Materials and Methods
This is a retrospective cohort study utilizing a firearm victim database. Milwaukee is a large American city with a population of approximately 700,000. The trauma center at Children's Hospital serves all youth firearm victims in Milwaukee, regardless of insurance status or location of injury. The study population was subjects aged 18 and younger who were presenting to a Pediatric Emergency Department/Trauma Center at Children's Hospital of Wisconsin between 1990 and 1995 who presented with firearm injuries. Patient information was obtained by (i) medical record review of sentinel event; (ii) ED records from Children's Hospital of Wisconsin and all other hospitals reviewed for subsequent events through 1997; and (iii) records from Milwaukee Medical Examiner's Office for subsequent death through 2003.
From medical records patient demographic information, prior injury history, type of injury, and cause of subsequent injuries and death if applicable, were obtained. Type of injury was acquired upon registration at the Emergency Department. The primary outcome was the event of recurrent ED visit for intentional injury. Intentional injury included firearm injuries, stabbing, injuries sustained in a fight and physical or sexual assault. Age in years at the sentinel event was categorized into four categories: < 12, 12-14, 15–16, and 17–18. Insurance type was categorized into three categories: Private (private, HMO), Public (public, HMO/public), and None. Disposition was categorized into three categories: Home, Hospital, and Other (detention center, police station). Guardian was categorized into four categories: Single mother/Single father, Two parents, Self, and Other. A prior history of ED visit due to violence and a social worker consulting at hospital were also obtained from the database. This study was approved by the Children's Hospital of Wisconsin Institutional Review Board (CHW, HRRC#159-95) and Medical College of Wisconsin Institutional Review Board (MCW, HRRC#283-05).
Descriptive statistics were used to summarize data. A Student t-test was used for continuous variables and Chi-squared test was used to compare categorical variables. Correlation analysis was conducted between covariates. The primary outcome, the REDV for intentional injury, was modeled by univariate and multivariable logit models. 16 To identify potential predictors for the final model, the variables were first examined at individually using univariate analysis. Variables were identified as significant using a 0.1 alpha level in the univariate model, and only these were included in a stepwise method to determine a final model. For the final multivariable model, a 0.05 alpha level was used. For each effect from the models the odds ratio and 95% confidence intervals were calculated. The goodness of fit was assessed using the Hosmer-Lemeshow (HL) statistic. 17 Univariate and multivariable logit models were performed by PROC LOGISTIC and PROC GENMOD procedures using SAS Version 9.
Results
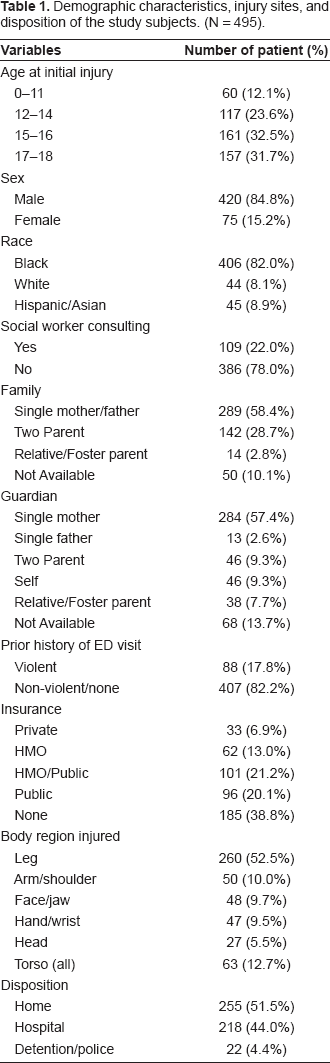
A total of 516 subjects were available in the pediatric firearm victim's ED visit database. Twenty-one subjects were dead (17 died of initial injuries and 4 died after the study period) and not eligible for this study. Of 495 subjects, 85% (n = 420) were males and 82% were African-Americans. Mean age was 15.1 years old (s.d = ±3.6). A majority of them (58%) were from single-parent family and 29% from two-parent family. Forty-one percent had public insurance and 39% had no insurance. Eighty-eight subjects (17.8%) had a prior history of ED visit due to violence. At initial injury, social workers were present for only 22% of the total subjects. About 52% were discharged to home, 44% to a hospital, and 4.4% to a detention center or police station. Table 1 showed the demographic characteristics, injury sites, and disposition of the study subjects.
Demographic characteristics, injury sites, and disposition of the study subjects. (N = 495).
Of 495 eligible subjects, 201 (41%) subjects had at least one REDV for violent injuries during the follow-up time (median follow-up time = 3.2 years). A total of 305 subsequent ED visits by 201 subjects were observed, with having multiple revisits (15%) and some persons a rather large number (5 revisits). Major causes of the REDV were due to another firearm injury (n = 62, 20.3%), laceration (n = 61, 20%), contusion (n = 45, 14.7%), and fight/brawl (n = 44, 14.4%). Comparing to the non-African-American, African-American subjects were more likely having REDV in age younger than 15 (p-value = 0.005), but that difference was not observed in age 15 or older group (p-value = 0.63). The REDV proportion of race by age group is shown in Figure 1 (Fig. 1: Proportion of repeat Emergency Department visits for violent injuries by age group and race). There was no difference in REDV between genders (p-value = 0.89).
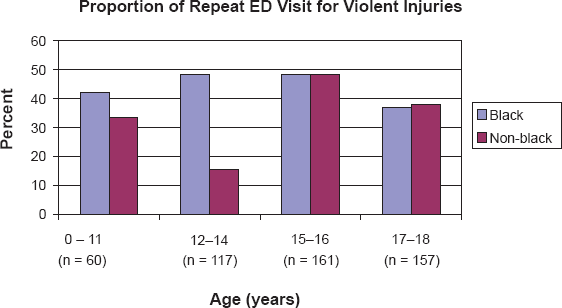
Proportion of repeat Emergency Department visits for violent injuries by age group and race.
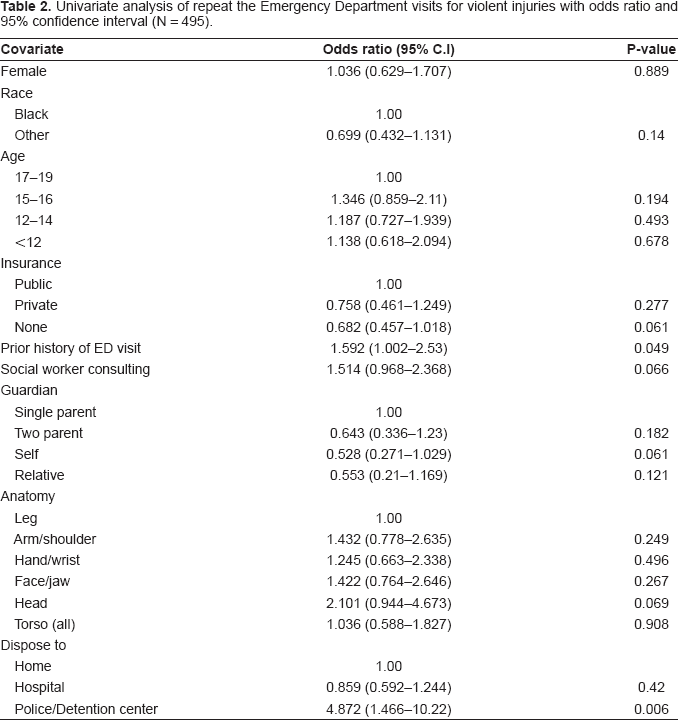
The analysis showed that four factors were associated with REDV for violent injuries in the univariate logit models (Table 2): guardian, prior histories of ED visit for violence, social worker consulting at the hospital, and disposition. Compared to a subject who did not have a prior history of ED visit due to violence, a subject who had a prior history of ED visit was more likely to have REDV (OR = 1.59, 95% C.I: 1.002–2.53, p = 0.049) in the univariate analysis. However, this association was not significant in the multivariable analysis.
Univariate analysis of repeat the Emergency Department visits for violent injuries with odds ratio and 95% confidence interval (N = 495).
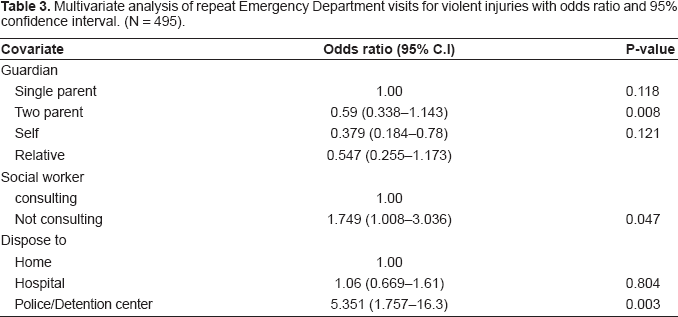
The multivariable logit model (Table 3) showed that guardian, social worker consulting at the hospital, and disposition were significantly associated with REDV for violent injuries. In the multivariable model, a subject without a social worker consulting at the hospital were more likely to have REDV compared to subjects with a social worker consulting (O.R = 1.749; 95% C.I: 1.008–3.036; p-value = 0.047), controlling for other significant predictors. Subjects disposed to a detention center or police custody were more likely to have REDV compared to subjects disposed to home or a hospital (O.R = 5.351; 95% C.I: 1.757–16.3; p-value = 0.003), controlling for guardian and social worker present at hospital. For a subject reporting self as a guardian, the odds of REDV to no REDV were decreased by 62%, compared to a subject who had a single parent as guardian. The analysis showed no difference in REDV among other guardians. There was no interaction among factors in the multivariable model. A sensitivity analyses was also performed to investigate the influence of death cases. When the analyses were extended to data when death cases were included as an event, the findings from our study remained unchanged.
Multivariate analysis of repeat Emergency Department visits for violent injuries with odds ratio and 95% confidence interval. (N = 495).
Discussion
This study demonstrates the burden of ED visits for repeat violent injury for a cohort of youth firearm victims and delineates particular protective and risk factors for these repeat emergency department visits. Having a social worker consult at the initial visit and being 18 years of age were significantly associated with decreased repeat emergency department visits for violence; disposition to police custody was associated with an increased risk for a repeat injury. These factors represent individual, social, and environmental aspects of urban adolescents. In order to develop interventions to prevent youth violence recidivism, it is important to understand the scope of the problem as well as the likelihood for repeat injury from violent behavior.
Our study showed a self-guardian, a youth who has reached the age of 18 and can thus consent for himself, was the least likely to have a recurrent ED visit. Perhaps younger firearm victims may be at increased risk for a repeat violent injury as compared to youth who have reached at eighteen years. Also, youth who reached age 18 may have moved from our community, became incarcerated, or died in another community and thus were unavailable to make repeat emergency department visits in our surveillance area. No statistical difference was observed in REDV between self-guardian subjects to two parents or relatives guardian subjects, but a trend that a youth with a single parent guardian was more likely to have REDV was observed. This result may suggest lower socioeconomic status, parental ability to supervise, or family instability.16–18 Family instability may be one of the most important reasons for increased repeat adolescent assault victimization.
Our study showed that social worker support at the sentinel ED visit was associated with decreased repeat visits for violence. The American Academy of Pediatrics and the Society of Adolescent Medicine both recommend psychosocial support for youth firearm victims at the time of their injury. 19 Wilkinson et al. noted that although emergency department staff counsel victims of violence, only 17% of hospitals had any formal training on youth violence. 22 The U.S. Department of Justice recommends timely support of “promising multi-service programs to reach families and gun victims within 24 hours of the shooting.” Other professionals have recommended increasing violence prevention/intervention support and training for physicians, nurses and crime victim specialists in the emergency setting.23–27 Our results further support these recommendations.
Disposition to police custody was associated with 5-fold increased risk for repeat emergency department visits for violence. Rivara et al. 28 found that young assault patients were significantly more likely to have had legal warnings or convictions as compared to youth presenting for unintentional injuries to an emergency department. Conversely, Borowsky and Ireland 29 found no difference in police contact for a group of adolescents between those suffering a subsequent fight-related injury and those who had not. Our results indicate that youth discharged in police custody are a high-risk group requiring intensive violence prevention services.
Our study has several limitations. First, our study examined repeat emergency department visits in Milwaukee hospitals and the death records in Milwaukee County; any ED visits or deaths outside of our community would not been captured. In addition, since the data were created from the medical records and the study subjects were not actively followed, it is not possible to estimate lost to follow-up component of this study. Second, accurate socioeconomic information, such as family income or neighborhood income, and neighborhood characteristics for the study subjects were not available, and thus the relationship between REDV for violent injuries and such variables limits us to infer causality in this study A future study direction would be to focus on more specific individual and environmental factors.
The young firearm victims in this cohort are at high risk to visit the emergency department for repeat violent injuries. Psychosocial support provided by social workers and other health care professionals at the time of the emergency department visit may provide a significant contribution in diminishing these repeat injuries. Youth discharged to the detention center following their emergency department visit are in particular need for these services. This is a cohort of urban adolescents at higher risk for subsequent REDV. By increasing the understanding of risk factors for recidivism of ED visit due to risky behavior or violence, our study findings will help practitioners developing interventions and new strategies to prevent youth violence in similar settings.
Footnotes
The authors report no conflicts of interest.