
Abstract
Background:
Takotsubo cardiomyopathy affects between 1.7% and 2.2% of patients hospitalized with suspected acute coronary syndromes. Characterized by chest pain, electrocardiogram changes, and transient left ventricular apical wall motion abnormality, it is under-recognized and often misdiagnosed.
Objectives:
In order to better differentiate between St-segment myocardial infarction and Takotsubo cardiomyopathy, we developed a scoring system.
Methods:
Of the 82 patients enrolled with Takotsubo cardiomyopathy, 67 had ST-segment elevation on electrocardiogram and were compared with 79 ST-elevation myocardial infarction patients. A multi-variant logistic regression model was used to find factors independently associated with Takotsubo cardiomyopathy. The Platelets and Thrombosis in Sheba (PLATIS)-Takotsubo cardiomyopathy is based on a 10-point scoring system: stressful events (3), females (2), no history of diabetes mellitus (2), estimated left ventricular ejection fraction ≤ 40% on admission echo (1), positive troponin on admission (1), and no smoking (1). Patients with Takotsubo cardiomyopathy were older (66 ± 11 vs 60 ± 11 years, p < 0.001), predominantly female (90% vs 15%, p < 0.001), with a lower incidence of diabetes mellitus, dyslipidemia, and smoking. Nevertheless, in-hospital mortality was similar in both groups.
Results:
In a multivariate logistic regression analysis, the average Platelets and Thrombosis in Sheba-Takotsubo cardiomyopathy scoring was significantly higher in Takotsubo cardiomyopathy compared with ST-elevation myocardial infarction patients (8.35 ± 1.7 vs 3.42 ± 1.6, p < 0.001). With an overall score of ≥7, the receiver-operating characteristic curve was 0.82 with a sensitivity of 75% and a specificity of 89% (positive predictive value = 85% and negative predictive value = 80%).
Conclusion:
The Takotsubo cardiomyopathy scoring system is a simple, reliable tool that can assist in diagnosing and differentiating between patients with Takotsubo cardiomyopathy and those with ST-elevation myocardial infarction.
Introduction
Takotsubo cardiomyopathy (TTC), also known as transient apical ballooning syndrome or stress-induced cardiomyopathy, is a distinct and usually reversible condition often affecting post-menopausal women after a stressful event. It is characterized by sudden temporary systolic dysfunction of the apical and/or mid-segments of the left ventricle. 1 The prevalence of TTC is between 1.7% and 2.2% in patients admitted to hospital with suspected acute coronary syndromes (ACS), with an increased prevalence reported among Caucasian Americans.1 –3 The underlying mechanisms have not yet been elucidated, but several hypotheses, including catecholamine cardiotoxicity, microvascular dysfunction, and coronary artery spasm, have been suggested.1,4 –6 Its diagnosis should be considered in the differential diagnosis of any patient with suspected acute myocardial infarction. 7 However, it is more common in post-menopausal women presenting with chest pain or dyspnea that is temporally related to emotional or physical stress, with positive cardiac biomarkers or an abnormal electrocardiogram (ECG).7,8 Moreover, patients with disproportionally high catecholamine stress-related responses and increased cardiac sympathetic sensitivity, as observed in patients with depression and anxiety, are also more prone to TTC.1,9 Because this syndrome is characterized by chest pain, ECG changes, and transient left ventricular apical wall motion abnormality, distinguishing it from acute myocardial infarction is a challenging and difficult task. 10 As a result, TTC is both under-recognized and often misdiagnosed.10,11 We prospectively evaluated and followed 82 consecutive TTC patients admitted to our cardiac intensive care unit in order to develop a scoring system, which could facilitate diagnosis.
Methods
A total of 82 consecutive patients admitted to the cardiac intensive care unit of the Sheba Medical Center with a diagnosis of TTC from 2004 to 2014 were prospectively enrolled. Of them, 67 patients had ST-segment elevation on ECG and hence comprised the TTC study population. We then developed a scoring system for the diagnosis of TTC (the Platelets and Thrombosis in Sheba (PLATIS)-TTC scoring system) and used it to compare these TTC patients with 79 other representative patients with acute ST-elevation myocardial infarction (STEMI) between 2004 and 2014. The Sheba Medical Center is a 1800-bed tertiary medical center with approximately 192,000 emergency department visits per year and more than 94,000 admissions annually.4,12
Inclusion criteria included (1) age > 18 years, (2) chest pain considered by the attending physician to be suggestive of cardiac origin or requiring admission in order to rule out STEMI/TTC, and (3) urgent heart catheterization within 24 h. Exclusion criteria included (1) any reason for chest pain other than ACS/TTC that was diagnosed in the emergency department, such as pneumonia, pulmonary embolism, pericarditis, or chest trauma; (2) patients under the age of 18; (3) left bundle branch block; (4) pregnancy; and (5) inability to sign a consent form.
Patients with a diagnosis of TTC (TTC group) were diagnosed according to the Mayo clinic criteria for diagnosis of TTC 5 and met the following criteria: sudden onset of chest pain with ECG changes, reversible balloon-like left ventricular wall motion abnormality at the apex with hypercontraction of the basal segments at left ventriculography or echocardiography, and troponin I changes mimicking acute myocardial infarction. Echocardiography was performed in all patients on day 1 and on days 3–5 of hospitalization. For the purpose of our study, we included only TTC patients who had ST-segment elevation on ECG.
All patients with the diagnosis of STEMI (STEMI group) met the following criteria according to the European Society of Cardiology/ACCF/AHA/World Heart Federation Task Force for the Universal Definition of Myocardial Infarction: 13 ECG ST-elevation in the absence of left ventricular hypertrophy or left bundle branch block; new ST-elevation at the J point in at least two contiguous leads of ≥2 mm (0.2 mV) in men, or ≥1.5 mm (0.15 mV) in women, in leads V2–V3 and/or of ≥1 mm (0.1 mV) in other contiguous chest leads or limb leads. The cardiologist who was in charge at the time of admission determined the diagnosis of STEMI.
Patient data were collected from interviews and medical charts, and 90 days after discharge patients were followed up by a phone interview. Data collected included demographics (age, gender, smoking, weight, body mass index); chronic illness (hypertension, diabetes mellitus, dyslipidemia, coronary artery disease, heart failure); previous percutaneous coronary intervention; and previous coronary artery bypass graft. Variables during hospitalization included ECG changes, troponin elevation, percutaneous coronary intervention, coronary artery bypass graft, discharge diagnoses, and discharge recommendations.
All patients were managed according to the discretion of the treating physician. Cardiac biomarkers were determined upon admission and after 3, 6, 12, 24, and 48 h, and after that every 24 h, and serial 12-lead electrocardiographic findings were recorded. Assessment of left ventricular ejection fraction (LVEF) by two-dimensional echo was performed upon admission and during day 3 or 5 after admission. All exams were analyzed by an echocardiography expert (cardiologist). Outcome measures during hospitalization and follow-up were mortality, stroke/transient ischemic attack, development of acute decompensated heart failure, cardiogenic shock, malignant arrhythmias, acute myocardial infarction, urgent revascularization, and TTC recurrence. Patients who were found to be eligible and who agreed to participate in the study signed a consent form. The study was approved by the Institutional Review Board.
Candidate risk factors were identified based on univariate differences between both groups. All factors with a p value of <0.1 for the difference between groups were further evaluated. Univariate relationships between candidate risk factors and the diagnosis of apical ballooning were assessed with logistic regression. Risk factors with an odds ratio of >1.3 and a p value of <0.20 were further evaluated by conducting a multi-variant logistic regression model using a forward stepwise approach. Factors found to be independently associated with the diagnosis of apical ballooning were carried to a second model. A simple risk score was constructed based on a Wald score in the final multivariable model. The weight assigned to each risk factor was calculated using a penalty of 4.3 on the Wald score. Hence, the PLATIS-TTC scoring system was based on a total of 10 points: a stressful event—3; female gender—2; no history of diabetes mellitus—2; estimated LVEF on echo on admission ≤40%—1; positive troponin I on admission (i.e. >0.06 ng/L)—1; and no smoking—1 point.
Stressful events were subjective according to the patients’ own experience.
Results
Patient characteristics are presented in Table 1. TTC patients were older (66 ± 11 vs 60 ± 11 years, p < 0.001), predominantly female (90% vs 15%, p < 0.001), and had a lower incidence of diabetes mellitus, dyslipidemia, and smoking, compared with the STEMI group.
Patient characteristics.
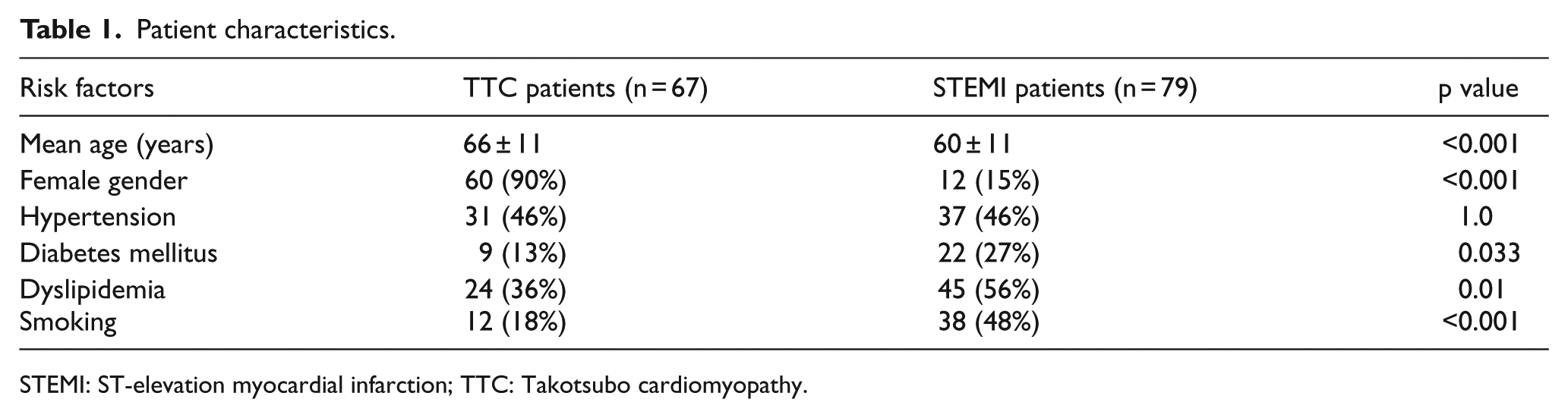
STEMI: ST-elevation myocardial infarction; TTC: Takotsubo cardiomyopathy.
At presentation, the TTC group suffered more than the STEMI group from stressful events that led to their admission (53 (79%) vs 6 (8%), respectively, p < 0.001), presented with an elevated troponin on admission (61 (91%) vs 30 (37%), p < 0.001), and ejection fraction ≤40% (54 (80%) vs 25 (31%), p < 0.001). On the other hand, the STEMI group had a higher rate of chest pain at presentation compared with the TTC group (79 (100%) vs 49 (73%), respectively, p < 0.001) as presented in Table 2.
Symptoms and echocardiography on admission.
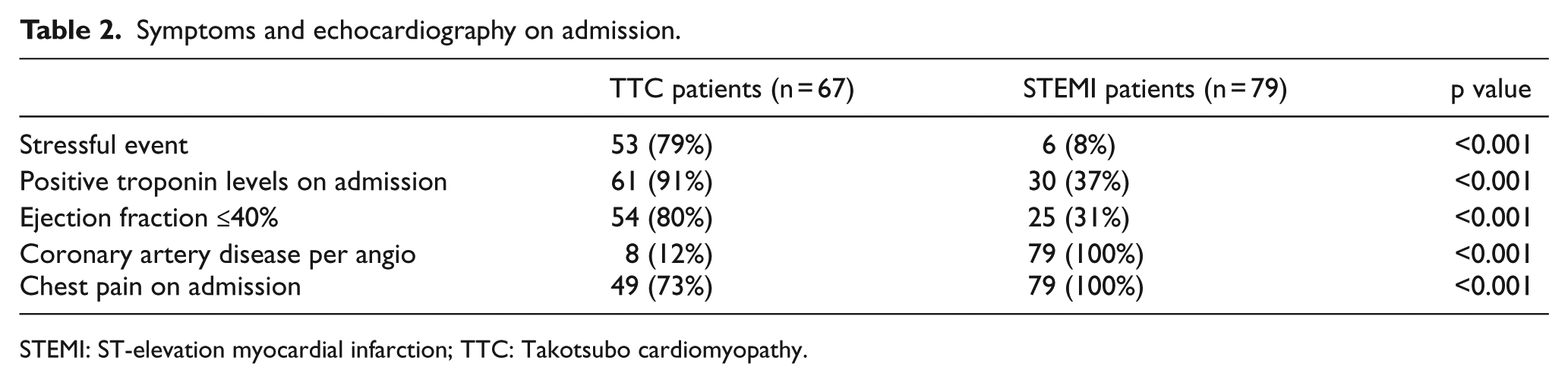
STEMI: ST-elevation myocardial infarction; TTC: Takotsubo cardiomyopathy.
Distribution of the ST-segment elevation on ECG is presented in Table 3. Of note, one-third of the TTC patients presented with ST-segment elevation on ECG in the lateral leads (LI, AVL, V5, and V6).
ST-segment elevation distribution on ECG at presentation.

ECG: electrocardiogram; STEMI: ST-elevation myocardial infarction; TTC: Takotsubo cardiomyopathy.
During admission, peak troponin level was lower in the TTC group compared with the STEMI group (4.9 ± 3 ng/L vs 48.6 ± 20 ng/L, respectively, p < 0.001). On angiography, coronary artery disease (>50% stenosis) was more prominent in the STEMI group compared with the TTC group (79 (100%) vs 10 (15%), respectively, p < 0.001). The in-hospital mortality rate was similar in both the TTC and STEMI groups (3 (3.6%) vs 1 (1.3%), respectively, p < 0.62).
The receiver-operating characteristic curve for the PLATIS-TTC scoring was 0.82. In a multivariate logistic regression analysis, the average PLATIS-TTC scoring was significantly higher in the TTC group compared with the STEMI group (8.35 ± 1.7 vs 3.42 ± 1.6, respectively, p < 0.001). With a scoring ≥7, the receiver-operating characteristic curve was 0.83 with a sensitivity of 74.6% and a specificity of 88.6% (positive predictive value = 84.7% and negative predictive value = 80.7%; Figures 1 to 3).
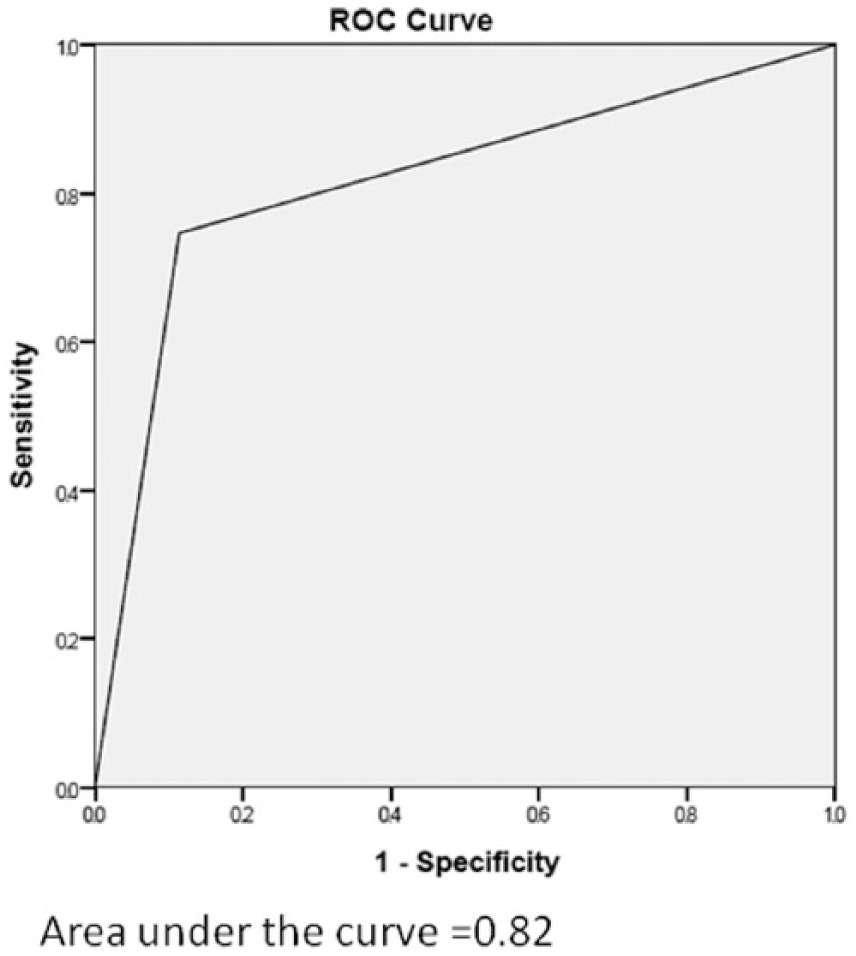
The receiver-operating characteristic curve with a scoring of ≥7.
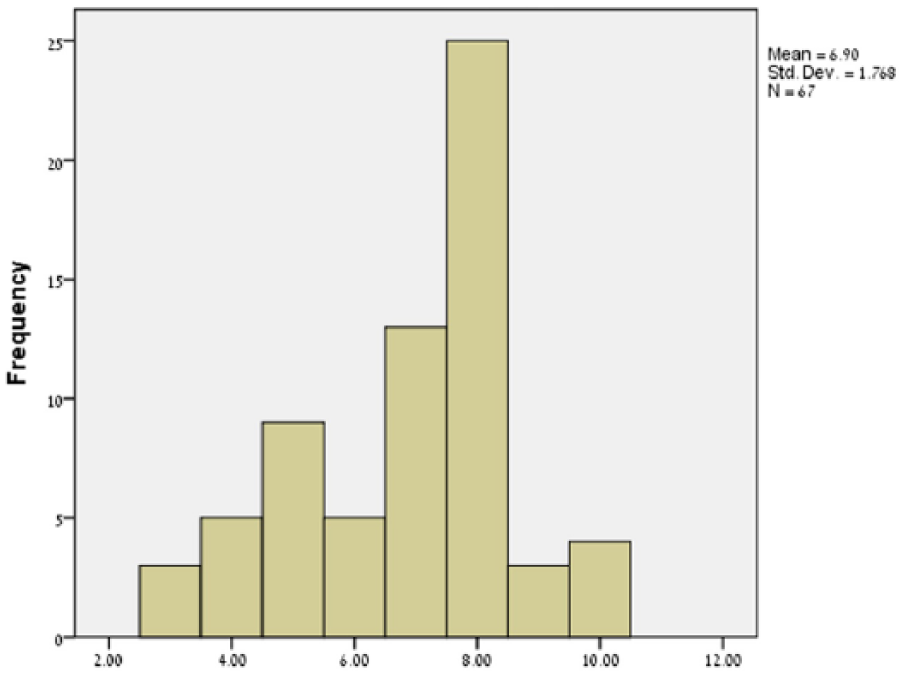
TTC histogram of the 10-point scoring system.
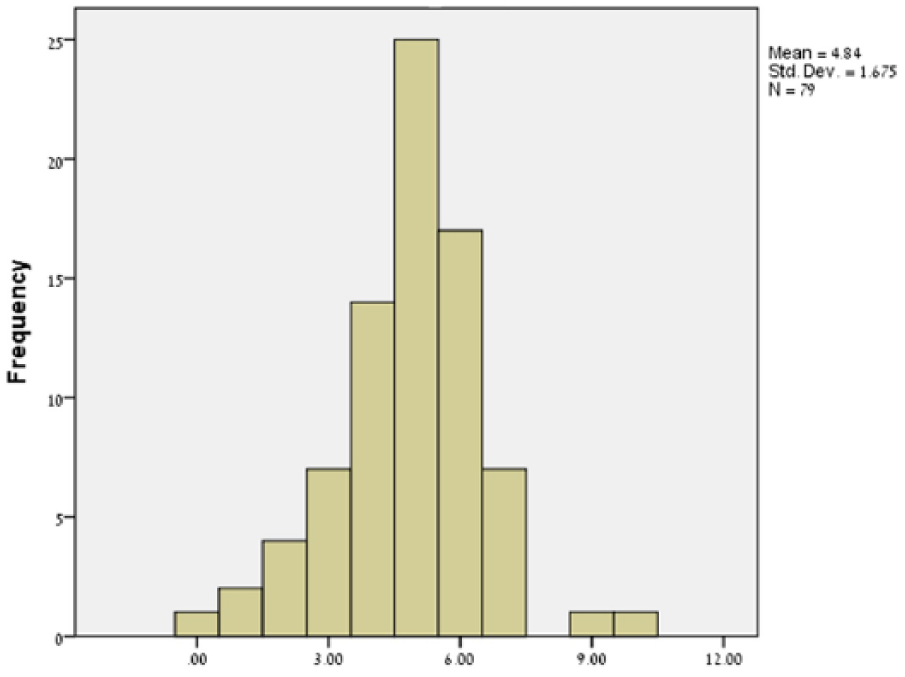
STEMI histogram of the 10-point scoring system.
Discussion
Our study is the first to demonstrate that TTC can be distinguished from STEMI by a relatively simple scoring system. Given its presentation and clinical outcome of acute heart failure with substantial morbidity and mortality, 14 it is important to promptly diagnose TTC and even more important to differentiate it from an acute myocardial infarction. Hence, we developed a simple scoring system, which facilitated distinction between TTC and STEMI patients. As in previous studies, our TTC group comprised predominantly elderly women and there was often a preceding emotional or physical trigger.15,16 In accord with other trials, the presence of positive troponin levels on admission was much more frequent in the TTC compared with the STEMI group, 14 while peak troponin levels were lower in the TTC compared with the STEMI group.14,17
Some studies have suggested that the prevalence of ST-segment elevation on ECG is less than half in TTC patients.18,19 Although we included only ST-segment elevation TTC patients in our study, more than half of all TTC patients enrolled during the study period had ST-segment elevation on admission ECG, with leads I and AVL being the most common leads with ST-segment elevation. Of note, only a minority of patients with TTC had diabetes mellitus or were active smokers. Notably, 12% of the TTC patients had evidence of coexisting coronary artery disease on angiography. Nevertheless, the lesions were far from being occlusive and had no correlation with the distribution of the ST-segment elevation on the ECG. In line with previous studies, this finding shows that the presence of coronary artery disease is not an exclusion criterion for the diagnosis of TTC.5,14,20 Our findings demonstrate a sensitivity of 75% and a specificity of 89% for an overall score ≥7; if we take into account the low prevalence of TTC (1%–2% in patients presenting with ST-segment elevation21,22), then the negative predictive value in this population should be as high as 99%. Moreover, other criteria such as the Duke criteria, which are commonly used for the diagnosis of endocarditis, have a collective sensitivity in numerous studies of only ≥80%.23 –25 In line with our findings, another recent trial, which aims to differentiate TTC from ACS using a clinical scoring, found sensitivity was 89% and specificity 91% for the diagnosis of TTC depending on the patients scoring number. 26 Notwithstanding, our findings and scoring system need to be further validated in future studies, and thus at this time the PLATIS-TTC scoring system should be used only as a tool to assist in the diagnosis of TTC. Limitations of our study include its single-center nature, its relatively small sample size, and the lack of long-term follow-up.
In conclusion, the PLATIS-TTC scoring system is a simple and reliable score, which can assist in the diagnosis of TTC and its differentiation from ACS.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The data are available with the authors.
Informed consent
The study was approved by the Institutional Review Board.
Ethical approval
The study was approved by the Institutional Review Board.