
Abstract
Introduction:
Patients with chest pain and concomitant ST-segment elevation on an electrocardiogram should be identified as having suspected ST-segment elevation myocardial infarction. However, various etiologies cause ST-segment elevation other than ST-segment elevation myocardial infarction, such as takotsubo cardiomyopathy.
Case presentation:
Here we report the case of a 77-year-old man who requested transport by helicopter emergency medical service for ST-segment elevation myocardial infarction but was consequently diagnosed with takotsubo cardiomyopathy due to spontaneous pneumothorax. En route, findings of electrocardiogram as well as focused cardiac point-of-care ultrasound could not distinguish takotsubo cardiomyopathy from ST-segment elevation myocardial infarction, but a subsequent point-of-care ultrasound could reveal occult pneumothorax, which ultimately revealed to be the culprit stress factor of takotsubo cardiomyopathy causing ST-segment elevation myocardial infarction–alike presentation. After treatment with a closed thoracostomy, he recovered from the takotsubo cardiomyopathy and pneumothorax and was discharged without any complications.
Discussion and conclusion:
We should consider takotsubo cardiomyopathy a disease with ST-segment elevation and spontaneous pneumothorax as one of its precipitating stressors. To clarify the diagnosis, point-of-care ultrasound using a systematic rather than region-of-interest approach may be a useful method in the emergency department.
Introduction
Patients with chest pain and concomitant ST-segment elevation on 12-lead electrocardiography (ECG) should be identified as having possible ST-segment elevation myocardial infarction (STEMI) because of the proven benefits of early reperfusion therapy. However, various etiologies can also cause ST-segment elevation, including takotsubo cardiomyopathy (TC) and spontaneous pneumothorax. 1
In the emergent setting, it may be difficult to distinguish other causes from STEMI by routinely used diagnostic modalities such as ECG, transthoracic echocardiography, and chest radiography. Moreover, it is important to diagnose rapidly as soon as possible because the time to treatment is one of the most important factors. Here we report the case of a 77-year-old man with presumed STEMI who was transported from a local hospital by helicopter emergency medical service (HEMS). Occult pneumothorax, which was considered as the stressor of TC causing STEMI-mimicking presentation, was ultimately diagnosed using point-of-care ultrasound (PoCUS).
Case report
A 77-year-old man presented to the emergency department (ED) of a rural hospital within an hour’s distance from our institution with ongoing chest pain for 50 min. He had mild chronic obstructive pulmonary disease, with pulmonary function studies showing an FEV1/FVC 47%, FEV1 1.73 L (73% predicted), inactive pulmonary tuberculosis, and stable rectal cancer after laparoscopic anterior resection, loop ileostomy, and repair. A 12-lead ECG revealed ST-segment elevation, but a chest radiograph (CXR) was not performed. The patient reported no improvement in the chest pain after sublingual nitroglycerin and intravenous morphine administration, and he was arranged for transfer to our institution by HEMS.
On presentation at the helicopter, the patient had normal blood pressure and body temperature, but tachypnea with a respiratory rate of 22/min was noted. Oxygen saturation was 95% on 10 L/min of oxygen delivered via a simple mask and measured by a pulse oximeter. A physical examination showed an alert mental status with no definite neurological deficits, but the lung and heart sounds were limited because of extensive ambient noise from the helicopter. Continuous cardiac monitoring using only limb leads revealed findings suggestive of ST-segment elevation. Cardiac PoCUS was performed to identify diagnostic evidence and complications of STEMI but was limited by poor echocardiographic windows consisting of only the subxiphoid view. A regional wall motion abnormality (RWMA) including akinesis of the left ventricle from the mid-cavity to apical segments appears to be consistent with STEMI with a culprit lesion of the mid-left anterior descending artery (LAD).
On presentation to the ED of our institution, the patient’s mental status had deteriorated into drowsiness with a blood pressure of 101/78, heart rate of 113 beats per minute, respiratory rate of 24 per minute, and body temperature of 37.0°C. Lung auscultation revealed bilateral coarse lung sounds with crackles. Oxygen saturation was 90% on 15 L/min with a reservoir mask; hence, he was intubated just after arrival at the ED to secure the airway. Twelve-lead ECG showed ST-segment elevation in precordial leads V1–5, a Q wave in precordial leads V1–4, and findings consistent with STEMI in the anteroseptal and anterior walls (Figure 1(a)). Cardiac biomarkers were elevated; in particular, high-sensitivity troponin I was 0.829 ng/mL (reference range, 0.00–0.02 ng/mL). Based on the clinical scenario and these findings, acute STEMI was strongly suspected. The emergent coronary angiography team was activated to prepare for early reperfusion therapy, and the patient was administered oral aspirin 300 mg, oral ticagrelor 180 mg through nasogastric tube, and intravenous heparin 4000 unit. Simultaneously, anteroposterior CXR and PoCUS on a supine position were performed to evaluate desaturation. Lung PoCUS in accordance with the BLUE protocol revealed abolition of the sliding on left lung and a few B lines with the sliding on right lung. 2 Lung points could not be identified on the anterior or lateral thorax (Figure 2(a)). Cardiac PoCUS showed reduced global left ventricular systolic function by visual estimation with the RWMA visible as reported by the HEMS (Figure 1(b)). Supine anteroposterior CXR revealed cardiomegaly, diffuse pulmonary congestion, and “deep sulcus” sign, showing slight radiolucency on the left lower lung field (Figure 2(b)). We strongly suspected that the patient had pneumothorax based on PoCUS findings, but due to the anti-ischemic agents, the patient’s bleeding risk was too high to allow an immediate thoracostomy or a similar procedure. Chest computed tomography performed to clarify the diagnosis of pneumothorax revealed moderate pneumothorax of the left lung. The patient was treated with closed thoracostomy and subsequently transferred to a cardiac catheterization facility. Coronary angiography showed minimal coronary artery disease, with 30%–40% stenosis of the diameters of both coronary artery systems. As a result, the clinical diagnosis was TC precipitated by spontaneous pneumothorax mimicking acute STEMI. After being admitted to the intensive care unit, the patient was treated conservatively for spontaneous pneumothorax and exacerbation of chronic obstructive pulmonary disease, after which his condition rapidly improved. He was extubated on hospitalization day 2, and the chest tube was removed on hospitalization day 7. Comprehensive transthoracic echocardiography performed on hospitalization day 11 revealed disappearance of the previous RWMA and restoration of the left ventricular global systolic function. The patient was discharged on hospitalization day 11 without any complaints.
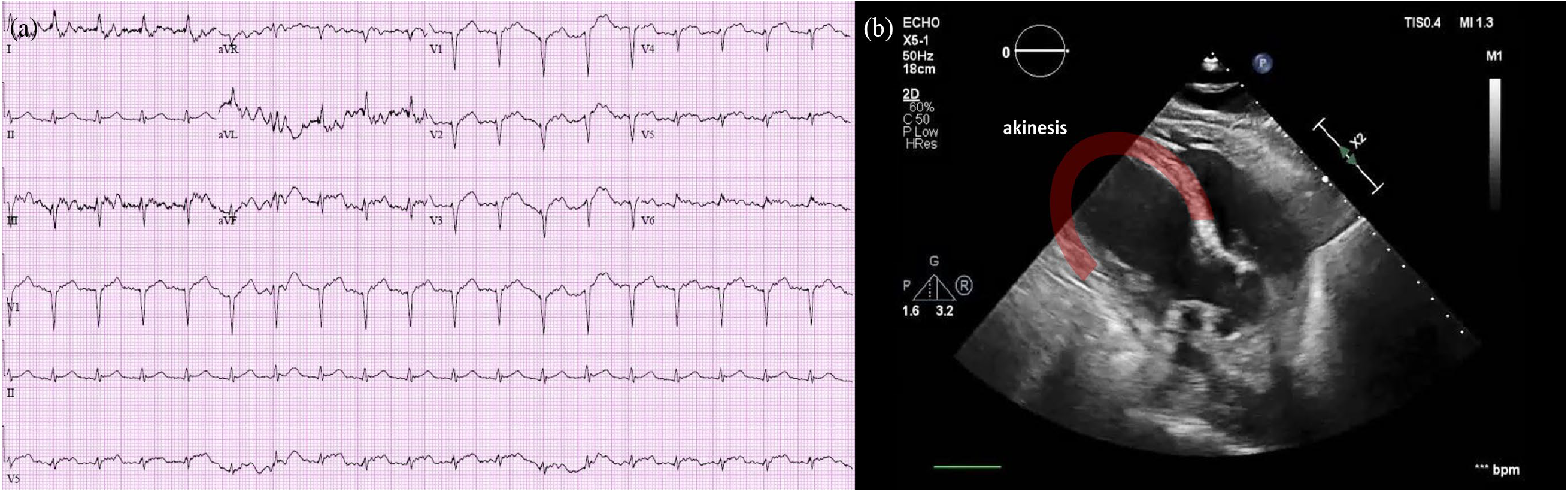
(a) Findings of 12-lead electrocardiography showing ST-segment elevation in precordial leads V1-5, consistent with STEMI in the anteroseptal and anterior walls. (b) Finding of focused cardiac point-of-care ultrasound showing regional wall motion abnormality including akinesis of the left ventricle from the mid-cavity to apical segments.
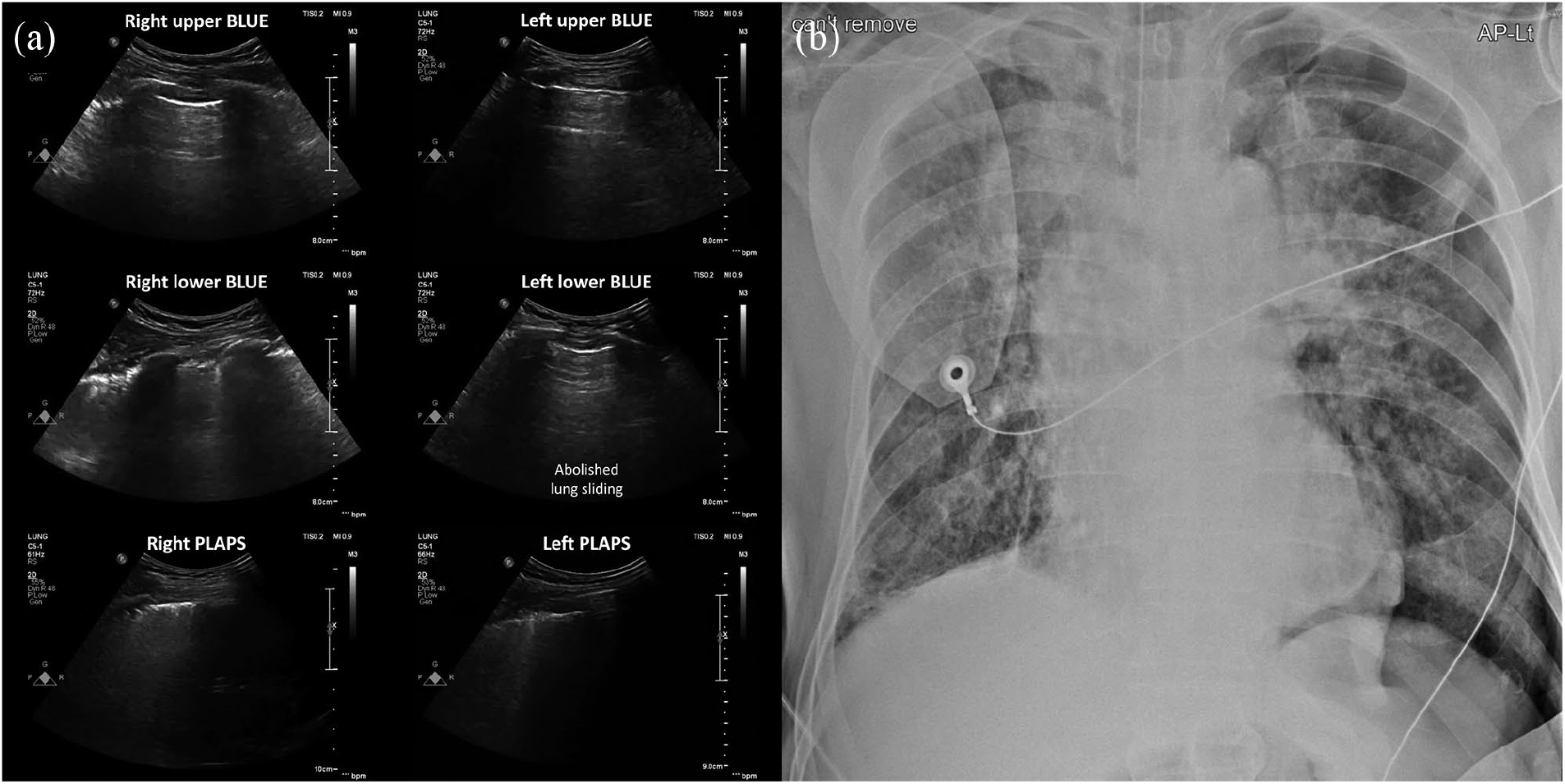
(a) Findings of lung ultrasound at the emergency department. There was abolished lung sliding at the left lower BLUE point without any identified lung point. (b) Findings of supine anteroposterior chest radiography at the emergency department. “Deep sulcus” sign of left lung was noted.
Discussion
Here we described the case of an elderly man with presumed acute STEMI that was consequently diagnosed as TC triggered by a spontaneous pneumothorax. His initial clinical presentation was consistent with acute STEMI, and the following assessments including ECG and cardiac PoCUS during HEMS supported the diagnosis. Afterward, a lung PoCUS assessment revealed that a secondary spontaneous pneumothorax had resulted in TC.
A preceding stressful event plays an important role in the occurrence of TC. A stressor usually consists of a physical or emotional factor; the latter triggers TC more frequently than the former.3–5 A diverse disease spectrum can induce physical stressors that cause TC, but only a few case reports to date have described pneumothorax.6,7 In the present patient, the subclinical spontaneous pneumothorax detected on PoCUS was a predominant preceding factor. TC, also known as stress-induced cardiomyopathy and apical ballooning syndrome, is a reversible cardiomyopathy with characteristic regional systolic dysfunction of the left ventricle by severe stressful events. 8 It is strenuous to differentiate TC from acute coronary syndrome (ACS) due to their similar clinical presentations including symptoms, ECG, cardiac biomarkers, and ultrasonography findings. Among the various ECG findings of TC, ST-segment elevation in anterior precordial leads is the most common finding that can mimic acute anterior STEMI. 9 TC typically involves hypokinesis or apical ballooning with hyperkinesis of the basal segments; thus, it is suitable that the term “takotsubo” comes from the Japanese word for “octopus pot.”3,8 In addition, the left ventricular ejection fraction is usually significantly reduced. There are some theoretical points to discriminate TC from ACS using ultrasonography. 10 In TC patients, the wall motion abnormality usually extends beyond the distribution of a single coronary artery, in which cases a reduced left ventricular ejection fraction can be restored. However, in the emergency setting such as HEMS, it can be difficult to differentiate between diagnoses, so the following clinical decisions are challenging. 11 In addition, TC cannot be distinguished in ACS patients with occlusion of the middle segments of a long LAD that extends past the apex of the left ventricle (wrap-around LAD). 12 In conclusion, RWMA alone should not be used as a key diagnostic feature.
PoCUS is gaining attention in emergency and critical care medicine. There are many reports about the usefulness of lung PoCUS as an important modality to diagnose pneumothorax in the emergency setting. Moreover, some studies revealed that ultrasonography can be superior to other conventional modalities, including CXR. 13 During aeromedical transport by helicopter, ultrasonography is one of the most useful assessment tools because other modalities are limited due to loud sound and confined space. In the present case, cardiac PoCUS alone was performed during HEMS based on the presumption of acute STEMI; later, investigation of the thorax at the ED disclosed the possibility of spontaneous pneumothorax. Emergency physicians need a systematic approach to simultaneous lung and cardiac PoCUS when evaluating patients with chest pain to ensure that the diagnosis is not missed. Repeated ultrasonography assessment may be needed to clarify occult pneumothorax.
Conclusion
Spontaneous pneumothorax can be a rare precipitator of TC. In the emergency setting, the use of a systematic approach including PoCUS and CXR should be considered to ensure prompt recognition of subclinical diseases.
Supplemental Material
informed_consent – Supplemental material for The importance of systematic point-of-care ultrasound for chest pain with ST-segment elevation: A case report of takotsubo cardiomyopathy precipitated by spontaneous pneumothorax
Supplemental material, informed_consent for The importance of systematic point-of-care ultrasound for chest pain with ST-segment elevation: A case report of takotsubo cardiomyopathy precipitated by spontaneous pneumothorax by Yoon-Seop Kim and Yong Sung Cha in Hong Kong Journal of Emergency Medicine
Footnotes
Author contributions
Study concept and design: Y.S.K. and Y.S.C. Writing – original draft preparation: Y.S.K. and Y.S.C. Writing – review and editing: Y.S.K. and Y.S.C. Approval of final manuscript: Y.S.C.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent was obtained from patient who agreed to the publication of images.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.