
Abstract
Introduction:
Patients with ST-elevation myocardial infarction are at risk of developing cardiac arrest. A validated tool for predicting cardiac arrest would help physicians recognize these high-risk patients earlier. This study assessed the usefulness of various score systems in predicting cardiac arrest in patients hospitalized for ST-elevation myocardial infarction.
Methods:
Patients’ data were retrieved from the hospital’s ST-elevation myocardial infarction registry records. Patients aged 18 years or older seen at the emergency department with a diagnosis of ST-elevation myocardial infarction between 1 July 2013 and 30 June 2014 were enrolled. The Thrombolysis in Myocardial Infarction score, the 6-month Global Registry of Acute Coronary Event risk score, CHADS2 score, and HEART score were calculated and compared.
Results:
A total of 249 patients were recruited. The Thrombolysis in Myocardial Infarction score, 6-month Global Registry of Acute Coronary Event risk score, CHADS2 score, and HEART scores were calculated. In total, 41 (16.5%) patients had cardiac arrest at emergency department or during hospitalization and 12 (29.3%) of them survived. The 6-month Global Registry of Acute Coronary Event risk score had the biggest area under the receiver-operating characteristic curve (0.72).
Conclusion:
The 6-month Global Registry of Acute Coronary Event risk score is more useful in predicting cardiac arrest in patients hospitalized for ST-elevation myocardial infarction than the other three scores. It is recommended that the 6-month Global Registry of Acute Coronary Event risk score be calculated for identifying emergency department patients hospitalized for ST-elevation myocardial infarction who are at risk of cardiac arrest during their hospital stay.
Introduction
Timely reperfusion by thrombolytics or percutaneous coronary intervention (PCI) is essential for patients with ST-elevation myocardial infarction (STEMI). 1 These patients are at risk of heart failure and death. 2 Cardiac arrest during emergency department (ED) boarding or hospital stay is probably the worst outcome among STEMI patients. 3 Identification of STEMI patients at high risk of cardiac arrest during hospital stay is thus important. It is not surprising that surveillance is the first link of the chain of survival for in-hospital cardiac arrest (IHCA). 4
There are several score systems used to risk-stratify STEMI patients. Examples include the Thrombolysis in Myocardial Infarction (TIMI) score,5,6 Global Registry of Acute Coronary Event (GRACE) score,7–9 Platelet glycoprotein IIb/IIIa in unstable angina: Receptor Suppression Using Integrilin (PURSUIT) score, 10 Fast Revascularization in Instability in Coronary disease (FRISC) score, HEART score, and CHADS2 score.11–13 These scores are mostly used for predicting mortality and morbidity during follow-up. A way to predict IHCA among STEMI patients remains unavailable. This study aimed at evaluating the usefulness of various score systems in predicting IHCA in ED patients hospitalized for STEMI.
Methods
This retrospective cohort study was conducted at a university-affiliated teaching hospital in Taiwan with approval by the Hospital Ethics Committee on Human Research (103-3638B). During the study period, all STEMI patients were managed according to the guidelines of the American College of Cardiology Foundation/American Heart Association (2009). 14
Patients aged 18 years or older admitted to the hospital via the ED with a definitive diagnosis of STEMI between 1 July 2013 and 30 June 2014 were enrolled. Patient data were retrieved from the hospital-based STEMI registry records. We reviewed the de-identified records and abstracted data using a standardized reporting template. Data required for calculating the TIMI score, CHADS2 score, 6-month GRACE score, and the HEART score were collected. Patient characteristics, medical history, electrocardiogram (ECG) findings, laboratory tests, Killip classes, medications, PCI, and door-to-balloon times were also recorded. The primary outcome was an IHCA during the index episode of STEMI.
The TIMI score, CHADS2 score, 6-month GRACE score, and the HEART score were calculated for all patients. The area under the curve (AUC) was abstracted using the receiver-operating characteristic (ROC) curve. The curve of the different scores, which were used to predict an IHCA, were compared. Further comparison of the AUC was made by the non-parametric method described by DeLong et al. 15 A cut-off point of optimum sensitivity and specificity were abstracted for the fit scale according to the AUC. Data were analyzed by SPSS 13.0 for Windows (SPSS, Chicago, IL, USA). Categorical variables were presented as numbers and percentages and compared using the chi-square or Fisher’s exact test, as appropriate. Continuous variables were presented as the median and interquartile range (IQR). The Mann–Whitney U test was used for non-normally distributed continuous variables. p < 0.05 was considered significant.
Results
A total of 417 patients were retrieved from hospital-based STEMI registry. In total, 168 were excluded because they were found to have diagnosis other than STEMI. In total, 249 patients with STEMI were enrolled for the analysis. Three patients who had return of spontaneous circulation after an out-of-hospital cardiac arrest were also included.
Table 1 shows the baseline characteristics of the enrolled patients. There was male predominance. The median age was 61 years. Most patients had a medical history of hyperlipidemia (60.6%) and hypertension (55.8%). Anterior lead ST segment elevation was observed on the ECG of 127 (51.0%) patients. The median serum Troponin I level was 0.43 ng/mL at ED. In all, 73.9% of the enrolled patients presented with Killip Class I status. Most patients received aspirin with clopidogrel or ticagrelor. Emergent PCI was done in 79.5% of patients with a median door-to-balloon time of 69 min. In total, 41 (16.5%) of 249 patients had an IHCA in ED or during hospitalization. Only 12 (29.3%) of them survived to discharge. Moreover, 32 (78.0%) of the patients with an IHCA had received PCI and 6 (18.8%) of them had IHCA before PCI.
Baseline characteristics of the enrolled patients.
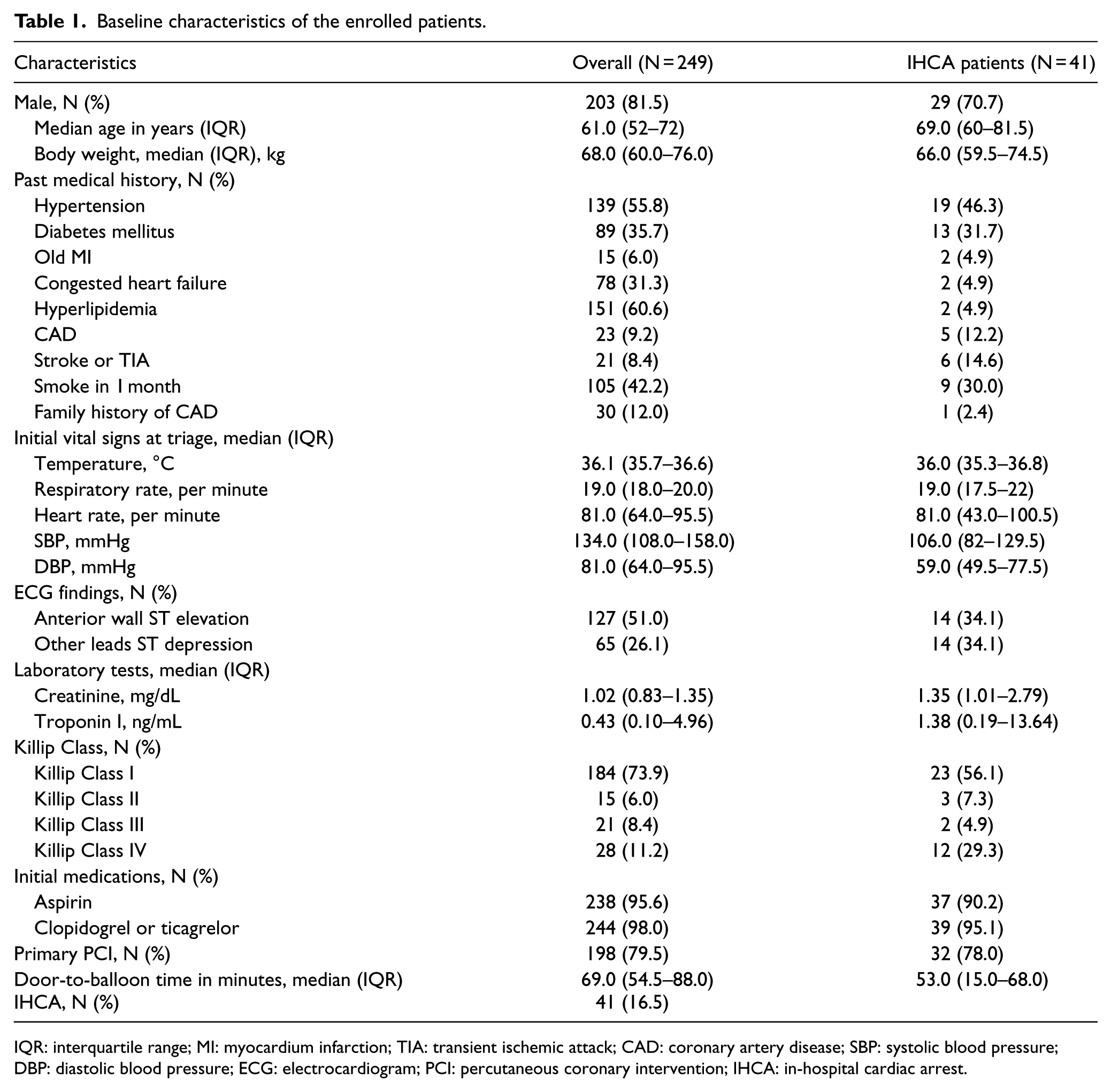
IQR: interquartile range; MI: myocardium infarction; TIA: transient ischemic attack; CAD: coronary artery disease; SBP: systolic blood pressure; DBP: diastolic blood pressure; ECG: electrocardiogram; PCI: percutaneous coronary intervention; IHCA: in-hospital cardiac arrest.
The different scores for STEMI patients with and without an IHCA were compared in Table 2. Significant differences were observed in all but the HEART score. The 6-month GRACE score had the highest AUC of 0.727 (95% confidence interval (CI), 0.645–0.809; p < 0.001) (Figure 1). In comparing the four AUCs, the AUC of 6-month GRACE score was significantly better than that of HEART score (p = 0.012) and CHADS2 score (p = 0.018) and showed a non-significant superiority over that of TIMI score (p = 0.624). A cut-off value of the total 6-month GRACE score of 121 was abstracted using the ROC curve, which yielded optimum sensitivity and specificity of IHCA with an odds ratio of 5.493 (95% CI, 2.64–11.22) (Table 3).
Differences between IHCA and non-IHCA groups for different scoring systems.
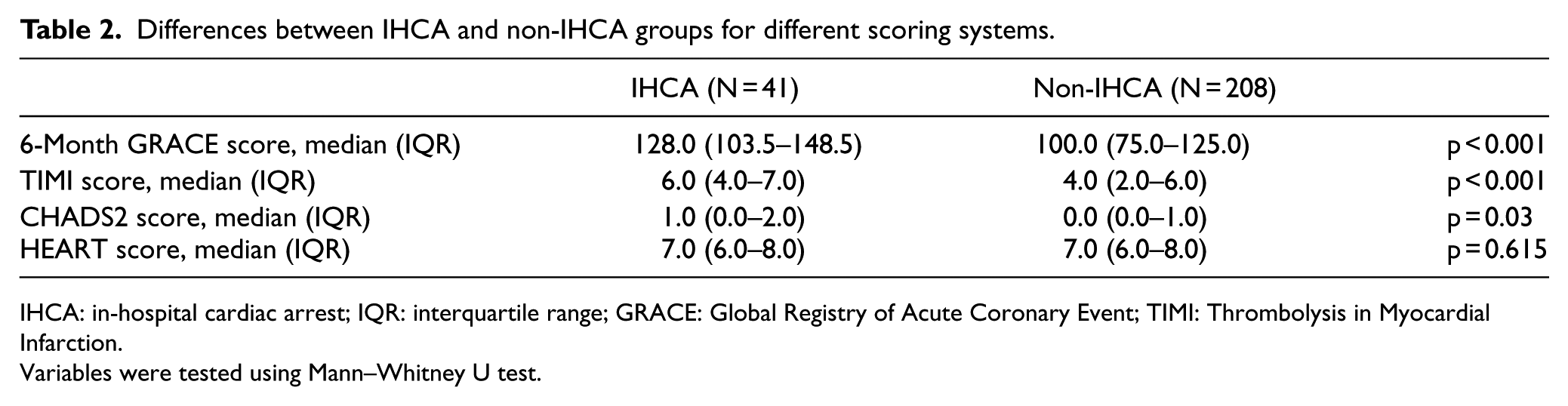
IHCA: in-hospital cardiac arrest; IQR: interquartile range; GRACE: Global Registry of Acute Coronary Event; TIMI: Thrombolysis in Myocardial Infarction.
Variables were tested using Mann–Whitney U test.
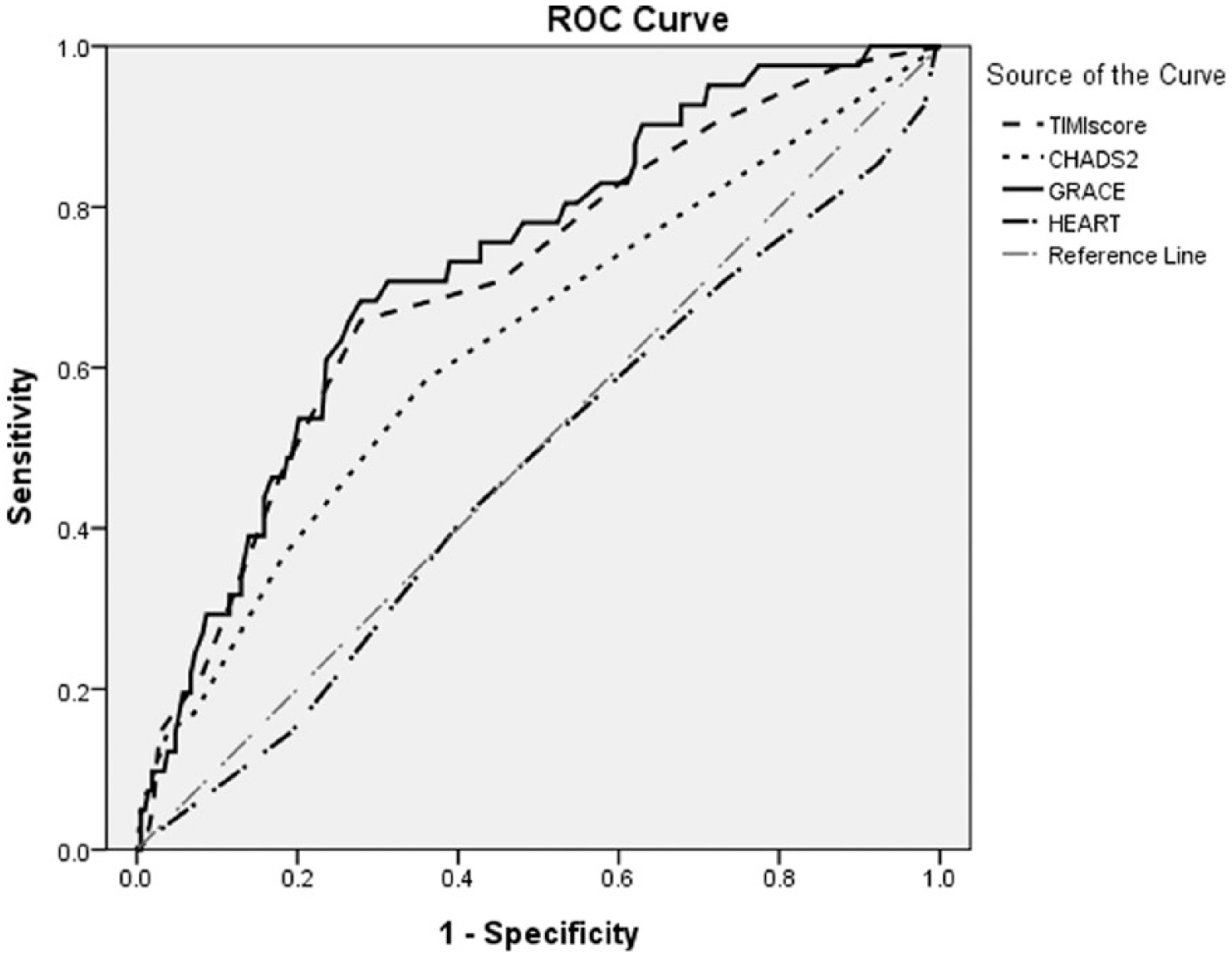
ROC curve of different scoring systems for predicting IHCA in patients with STEMI. TIMI score (AUC, 0.705; 95% CI, 0.618–0.793), CHADS2 score (AUC, 0.630; 95% CI, 0.532–0.728), 6-month GRACE score (AUC, 0.727; 95% CI, 0.645–0.809), and HEART score (AUC, 0.476; 95% CI, 0.377–0.575).
A cut-off optimum of the 6-month GRACE score.
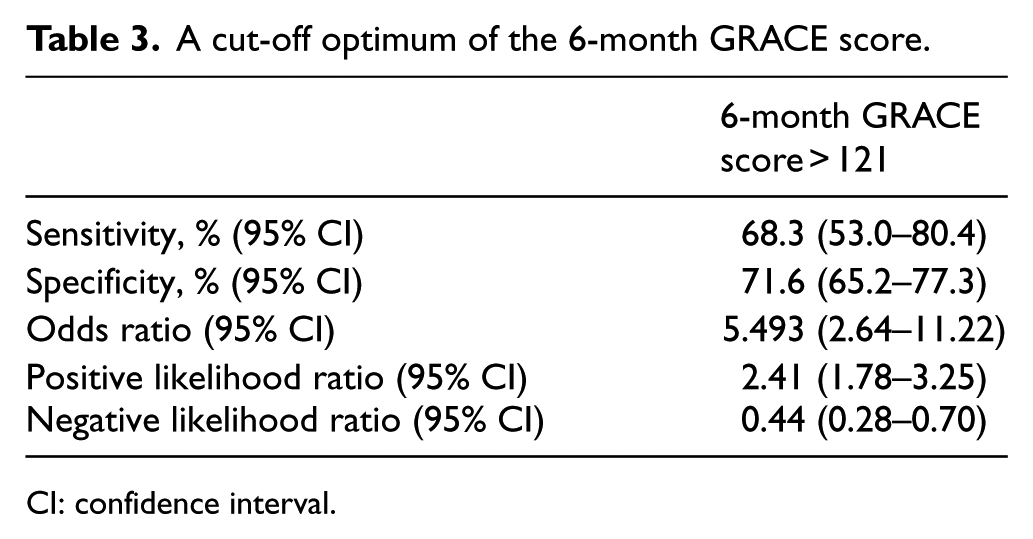
CI: confidence interval.
Discussion
The 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care had revised a specific chain of survival for IHCA. Cardiac arrest ever occurred during hospital stay are significantly related to poor outcomes and mortality. 3 Therefore, the new guidelines put surveillance and prevention of cardiac arrest as the first link. 4 According to the study results, 6-month GRACE score could be an appropriate choice for surveillance compared to TIMI score, HEART score, and CHADS2 score. A high 6-month GRACE score could indicate the need for more intensive management strategies. Although over half of the enrolled patients were in their middle age, presented with Killip Class I, had a serum Troponin I level below 0.5 ng/mL at ED, and the median door-to-balloon time was 69 min, the rate of an IHCA was high (16.5%). To improve the outcome for these high-risk patients, timely intensive treatment with close monitoring should be considered. Stronger coordination between the PCI and cardiac surgery teams for rescuing coronary bypass surgery should also be considered.
Regarding the different performance in predicting an IHCA post-STEMI by the various scores, the CHADS2 and HEART scores were initially developed for other purposes. The HEART score was developed to discriminate the cardiac factor of chest pain so as to facilitate diagnosis and treatment. 12 The CHADS2 score was initially designed to evaluate stroke risk for patients who have atrial fibrillation and helps selecting an antithrombotic therapy. 13 The 6-month GRACE score and TIMI score are used to evaluate the severity and prognosis of acute coronary syndrome (ACS). The TIMI score predicts 30-day mortality for patients with STEMI, and the 6-month GRACE score is for predicting mortality in patients with ACS.5,9 The 6-month GRACE score observes the entire spectrum of age as a continuous prognostic value while the TIMI score includes age as a categorical variable. A relation between old age and high mortality or morbidity rate in patients with ACS has been reported.16,17 In addition, the 6-month GRACE score includes patients’ history of heart failure and myocardial infarction (MI), whereas TIMI score includes patients’ history of diabetes, angina, and hypertension. A history of heart failure and MI may indicate poorer baseline heart function, which leads to inferior outcomes.16–20 The 6-month GRACE score considers serum creatinine which is a powerful independent prognosticator for long-term mortality.21,22 Moreover, GRACE score is adapted with an elevation in initial serum cardiac enzyme level, which is indicative of a large infarction size or a longer duration. A large infarct may suggest poorer condition of the coronary vessels, and a higher risk of PCI failure, which leads to fatal dysrhythmia and cardiac arrest. The aforementioned factors may contribute to the superiority of the 6-month GRACE score in predicting an IHCA post-STEMI.
Although the 6-month GRACE score was shown to have better performance in predicting IHCA in patients suffering from a STEMI, it was not designed for this purpose originally. A scoring system specifically for the purpose should be developed. This is because the mortality of IHCA in ED patients hospitalized for STEMI is not low, as shown in this study. The new scoring system perhaps can be developed on the basis of the 6-month GRACE score.
Limitation
This study should be interpreted in the context of the following limitations. First, although the diagnosis of all enrolled patients are retrieved from the hospital-based STEMI registry records, selection bias might be present for the retrospective study design and a high number of excluded patients. Second, there might be unmeasurable confounders, such as treatment strategy selection based on clinical judgment. However, we attempted to collect complete patient data from a computer database and the medical records using a standard template, which fulfills the criteria for all score systems. Third, this study was conducted in one hospital only. It might limit the generalizability of the results.
Conclusion
The 6-month GRACE score was shown to be more useful in predicting IHCA in patients with STEMI during the hospital stay compared to the TIMI score, HEART score, and CHADS2 score. Since the mortality rate of IHCA patients is not low, the 6-month GRACE score should be regarded as a surveillance guide for identifying patients at risk of IHCA. Further intensive care strategy and monitoring should be based on the evidence of GRACE score for risk stratification.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.