At the Plaza de Mulas medical tent, located at 4300 m (14,100 ft) along the Normal Route to the 6960 m (22,837 ft) summit of Aconcagua in Argentina, a Korean male in his 50s with no known medical conditions presented with lightheadedness and shortness of breath. He had taken sildenafil and acetazolamide that morning without improvement. Vital signs on arrival were notable for oxygen saturations in the high 60s with basilar crackles on lung auscultation, concerning for high altitude pulmonary edema. The patient was started on oxygen via nasal cannula and given dexamethasone. History was limited secondary to language barriers, but on review of systems the patient noted mild chest pressure. Bedside cardiac echocardiogram was performed, which revealed a septal wall motion abnormality. The patient was therefore given aspirin and clopidogrel and was flown to a lower trailhead, where he was met by local Emergency Medical Services. A 12-lead electrocardiogram revealed an anterior ST-elevation myocardial infarction, and the patient was taken emergently to the catheterization lab in Mendoza and underwent stent placement with a full recovery.
Dr. Chance Sullivan: At the Plaza de Mulas medical tent, located at 4300 m (14,100 ft) along the Normal Route to the 6960 m (22,837 ft) summit of Aconcagua in Argentina, a male climber in his 50s with no known medical conditions presented with light-headedness and shortness of breath. He reported that his symptoms started that morning while he was attempting an acclimatization hike to Plaza Canada at 5050 m (16,568 ft) and had not improved with rest or descent back to Plaza de Mulas. He self-administered 50 mg sildenafil and 250 mg acetazolamide without improvement in his symptoms. Vital signs on arrival at the clinic were notable for an oxygen saturation of 68%, blood pressure of 100/64 mm Hg, and a heart rate of 84 beats/min. The patient appeared diaphoretic and mildly tachypneic, and his exam was notable for faint bibasilar crackles on lung auscultation. No peripheral edema was noted.
Dr. Ellen Stein: A common mantra at altitude is “When at altitude, all illness is related to altitude until proven otherwise.” Was there anything in this patient's history or presentation that made you consider other disease processes as a cause of his symptoms?
Dr. Chance Sullivan: High altitude pulmonary edema (HAPE) was the leading diagnosis for a patient presenting to a high altitude clinic with shortness of breath and hypoxia. However, his overall appearance, with diaphoresis and dyspnea at rest, was notably more concerning in comparison with the many other HAPE cases we had seen in the clinic. History taking was limited due to language barriers; the patient was from Korea and spoke very minimal English and no Spanish. When asked directly on review of systems, the patient did endorse mild chest pressure. He denied any cardiac history. He was answering questions appropriately and following commands, with no evidence of altered mental status. He denied infectious symptoms to suggest pneumonia or upper respiratory infection. On exam, he had no evidence of peripheral edema or jugular venous distension to suggest congestive heart failure. His endorsed chest pressure was worrisome for acute coronary syndrome (ACS), but an electrocardiogram (ECG) was not available. Point-of-care ultrasound was performed, and it showed scattered B-lines in the bilateral lower lung fields. The patient had no right heart strain or absence of lung sliding to suggest pulmonary embolism or pneumothorax. However, his cardiac ultrasound revealed septal wall hypokinesis. This was presumed to be new given his reported lack of cardiac history, especially given that he was complaining of new-onset chest pressure and shortness of breath. ACS became a leading concern, potentially with concurrent HAPE.
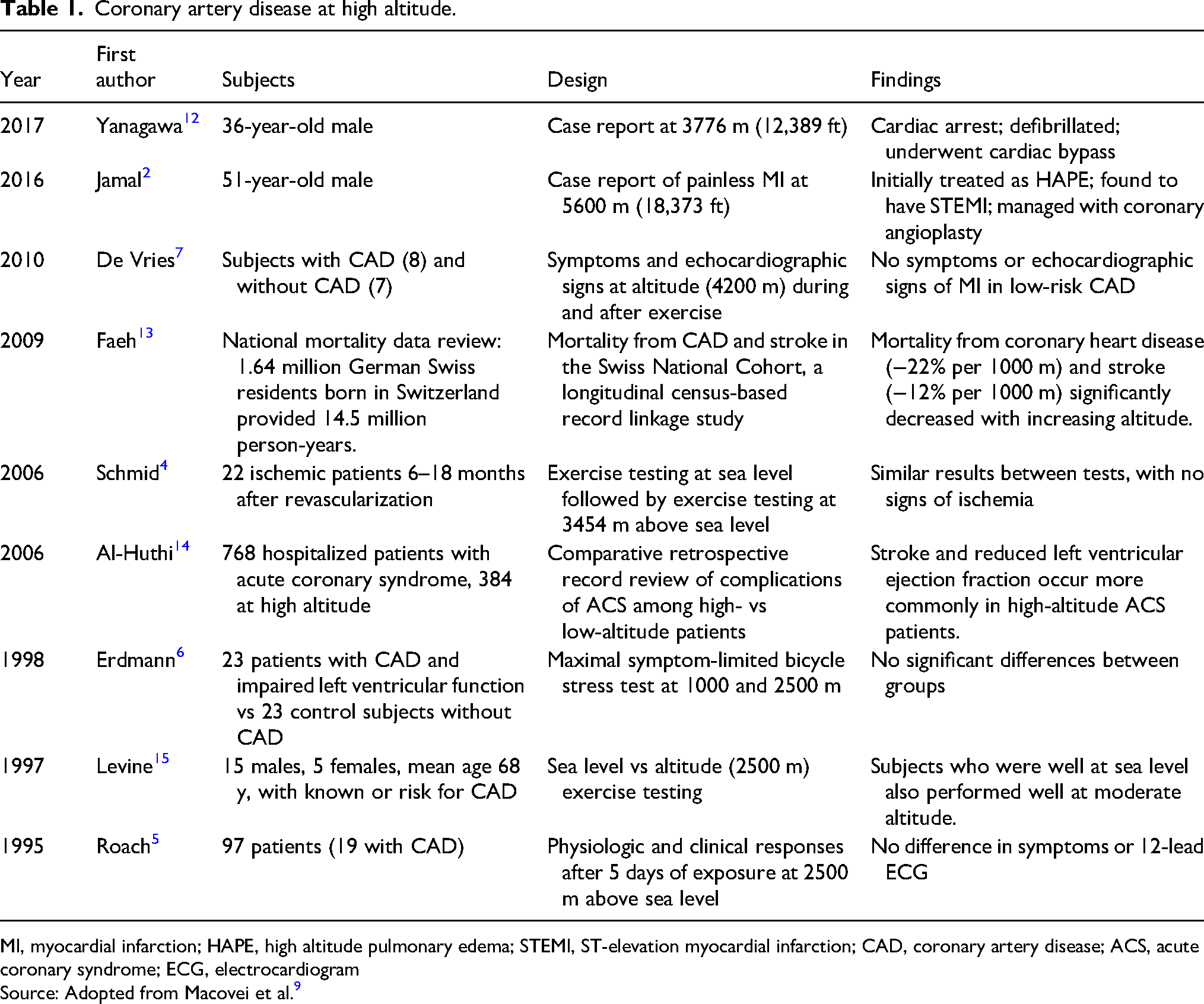
Dr. Sarah Schlein: It is interesting to consider which elements of the history of present illness and exam might raise ACS above HAPE as the underlying pathology. Literature addressing differences in presentations between cardiac and pulmonary causes of hypoxia and chest pain at altitude is limited.1,2 Careful histories and physical exams, combined with the use of tools such as a handheld ultrasound or portable ECG, are key to making such a critical diagnosis. A growing trend toward increased age and underlying comorbidities of travelers to altitude3 may lead to more occurrences of ACS that may aid future studies. That being said, a history of coronary artery disease (CAD) is not an absolute contraindication to traveling at high altitude.4–7 Interestingly, one study found living at altitude protective of CAD,8 and for travelers to high altitude, symptoms and echocardiographic evidence of left ventricular dysfunction or wall motion abnormalities were absent in low-risk patients with a history of CAD during and after exercise up to an altitude of 4200 m (13,780 ft),7 whereas other reviews found rare complications of traveling to altitude after myocardial infarction.9 Studies looking at CAD at altitude are summarized in Table 1. As remote medical evaluation evolves to include portable ECG, we will need to interpret changes with caution because one study found that incidental ECG changes at high altitude, without symptoms, were not associated with CAD on cardiac angiography.10 ECG changes may include right axis deviation, right bundle branch blocks, or changes in amplitude of P and T waves, consistent with increases in pulmonary artery pressure.11
More so, it seems that unaccustomed physical activity is more likely to trigger sudden cardiac death than the high altitude itself.16,17 Existing data suggest that climbers with stable CAD on optimal treatment and in good physical condition can tolerate traveling to high altitude up to 3500 m. However, patients with unstable angina or recent myocardial infarction should use caution with strenuous activity involving high altitude.9 In all climbers with known CAD, optimal medical management and prudent acclimatization are paramount,15 and cardiac stress testing should be considered prior to trip departure.11
Dr. Aaron Brillhart: You used your handheld ultrasound to visualize cardiac wall motion abnormalities as well as bilateral B-lines. Point-of-care ultrasound and the presence of B-lines are felt to be sensitive but not specific for the detection of HAPE.18 Yet, in this case, ultrasound seemed to be clinically useful. What findings did you feel were most useful to assist you in determining that the patient was suffering from acute coronary syndrome? Did you find other specific findings that could be used to determine whether his suspected pulmonary edema arose from high altitude exposure versus possible acute heart failure in the setting of myocardial infarction?
Dr. Chance Sullivan: While pulmonary B-lines on ultrasound are nonspecific for ACS or HAPE, a septal wall motion abnormality would not be expected with HAPE alone. Focal wall motion abnormalities are often seen in areas of ischemia to the myocardium, especially in the setting of concerning chest pain. The patient’s septal wall motion abnormalities may have suggested a left anterior descending artery occlusion leading to ischemia of the cardiac septum. A myocardial infarction in this region of the heart then could lead to acute systolic heart failure and pulmonary edema and the appearance of bilateral pulmonary B-lines. However, the patient's ultrasound revealed a normal ejection fraction. It is possible that he developed HAPE first, causing pulmonary congestion and increased cardiac demand, eventually leading to ACS. Ultrasound alone cannot tell us the whole story, but it increased our suspicion for another diagnosis, especially given the limited ability to obtain a full history from the patient.
Dr. Ellen Stein: Although you had a well-founded suspicion that your patient was having a cardiac event, it was impossible to make a definitive diagnosis. Because he also may have had elements of HAPE contributing to his symptoms, what did you feel you should do for the patient to safely treat his ACS, and how did you balance therapeutic considerations for HAPE?
Dr. Chance Sullivan: Treatment for this patient, as with many patients in austere environments, must carefully balance both potential benefit and harm. To address the concern for ACS, aspirin was given immediately, and the patient was started on oxygen via nasal cannula. Nitroglycerin was not given due to his recent self-administered sildenafil and concern for the risk of hypotension. Anticoagulants and thrombolytics were not available but certainly would have posed an interesting therapeutic consideration given the delay to cardiac catheterization. However, thrombolysis complications include life-threatening bleeding, which would be challenging to manage in an austere environment. Furthermore, medication storage and administration and patient observation after administration by a trained provider throughout transport pose challenges and therefore are not currently in use in this setting.
To address the patient’s potential HAPE, as mentioned earlier, he was immediately started on oxygen via nasal cannula. Given guideline recommendations, nifedipine administration was considered.18,19 However, his hypotension was considered a relative contraindication, especially when the diagnosis remained unclear. Because oxygen and descent are key steps in management regardless of etiology, arrangements were immediately made to evacuate the patient via helicopter. A portable hyperbaric bag (Gamow Bag, Chinook Medical Gear Inc, Tulsa, OK) was available, but there were no delays in helicopter transport and therefore hyperbaric therapy was not necessary.
Dr. Aaron Brillhart: Dr. Rodrigo Duplessis is the medical coordinator of Extreme Medicine, a private operation contracted by Aconcagua Provincial Park to function as the park medical service and to provide medical screening and care for all sick and injured climbers on Mount Aconcagua. The medical service oversees the medical aspects of rescues and evacuations on the mountain and maintains a medical base and large dome tent at the Plaza de Mulas Base Camp. Dr. Duplessis also was present and cared for this patient. Dr. Duplessis, could you describe the typical medical management for this type of patient in your remote base camp environment and the normal evacuation procedure from the Mount Aconcagua Base Camp?
Dr. Rodrigo Duplessis: In terms of management, despite the language barrier, our medical team was able to rapidly respond to this patient. Furthermore, the use of ultrasound corroborated our primary diagnostic suspicion of ACS. Given our differential diagnoses, our management focused on the administration of oxygen, aspirin, clopidogrel, and atorvastatin and minimizing any possible cardiac demand of the patient, including carrying him by stretcher to the helicopter landing zone. An automated external defibrillator and advanced medications including epinephrine were available, so advanced cardiac life support could have been provided if the patient deteriorated. Fortunately, this was not necessary. This case highlights the value of basic cardiac testing at the Plaza de Mulas Base Camp, and limited ECG capabilities are now available as of the 2023–24 season.
Regarding the evacuation process, our medical service determines evacuation necessity, makes transport recommendations, and monitors and stabilizes the patient until transport arrives. Transport is often via helicopter to the Horcones Park entrance at 2950 m (9680 ft) if conditions permit, and this process is in coordination with Aconcagua Park Rangers. The park service helicopter is modified for high-altitude flight and is not staffed with medical personnel or equipment beyond supplemental oxygen. Depending on patient severity, flight carrying capacity, and pilot guidance, the medical service determines whether a physician should accompany the patient in the rescue helicopter. Our doctors will, at times, accompany the patient and provide a transfer of care on meeting local emergency services. The park service then coordinates with the provincial emergency service to arrange transport of the patient by ground ambulance or medical helicopter from the park entrance to either a rural hospital or a larger hospital in the city of Mendoza depending on the complexity of the case. Although not common, if needed, our doctor can accompany a patient in the rescue helicopter and directly transfer care to the responding emergency services transport doctor at the park entrance landing zone.
Dr. Chance Sullivan: Stable patients, such as those with mild HAPE, often improve rapidly with descent and therefore do not require hospitalization. In this case, however, the patient clearly needed further workup and management based on our ultrasound findings and his description of chest discomfort. He was met by EMS at the trailhead and taken directly to the nearest tertiary care center in Mendoza. Case follow-up confirmed that he had a prehospital ECG displaying an occlusive myocardial injury pattern (Figure 1), and he underwent successful coronary artery stenting immediately after evacuation.
Prehospital electrocardiogram.
Conclusion
Given the growing number of climbers with cardiac comorbidities, chronic illnesses, and advanced age participating in mountaineering, practitioners in these settings may expect more presentations of ACS. While a history of CAD is not an absolute contraindication to climbing at high altitude, medical optimization and adequate acclimatization prior to the climb are important considerations. Some of the medications used to treat altitude illness may pose a risk for patients with ACS, adding to the risk of misdiagnosing ACS as HAPE or in potential situations with simultaneous ACS and HAPE. Calcium channel blockers and phosphodiesterase inhibitors could compromise blood pressure, especially in the setting of a preload-dependent inferior myocardial infarction, which could be dangerous in a setting with limited ability to correct for hypotension. Careful consideration of ACS in addition to HAPE is prudent, and the use of portable diagnostic tools may be helpful in guiding the diagnosis. Weighing the risks and benefits of treatment and evacuation in remote settings is important. This case highlights the utility of point-of-care ultrasound in aiding decision making and patient care in expedition medicine.
Footnotes
Author Contribution(s)
Chance Sullivan: Conceptualization; Data curation; Formal analysis; Writing – original draft; Writing – review & editing.
Aaron Brillhart: Conceptualization; Data curation; Formal analysis; Writing – original draft; Writing – review & editing.
Rodrigo J. Duplessis: Conceptualization; Data curation; Formal analysis; Writing – original draft; Writing – review & editing.
Ellen Stein: Conceptualization; Data curation; Formal analysis; Writing – original draft; Writing – review & editing.
Sarah M. Schlein: Conceptualization; Data curation; Formal analysis; Writing – original draft; Writing – review & editing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
1.
BasnyatBSillDGuptaV. Myocardial infarction or high-altitude pulmonary edema?Wilderness Environ Med. 2000;11(3):196-198.
2.
JamalNRajhyMBapumiaM. Painless acute myocardial infarction on Mount Kilimanjaro. BMJCase Rep. 2016;2016.
3.
KeyesLEMatherLDukeC, et al.Older age, chronic medical conditions and polypharmacy in Himalayan trekkers in Nepal: an epidemiologic survey and case series. J Travel Med. 2016;23(6):taw052.
4.
SchmidJPNoveanuMGailletRHelligeGWahlASanerH. Safety and exercise tolerance of acute high altitude exposure (3454 m) among patients with coronary artery disease. Heart. 2006;92(7):921-925.
5.
RoachRCHoustonCSHonigmanB, et al.How well do older persons tolerate moderate altitude?West J Med. 1995;162:32-36.
6.
ErdmannJSunKTMasarPNiederhauserH. Effects of exposure to altitude on men with coronary artery disease and impaired left ventricular function. Am J Cardiol. 1998;81:266-270.
7.
De VriesSTvan EnstGCBreemanAHofAWJV. Effects of altitude on exercise level and heart rate in patients with coronary artery disease and healthy controls. Neth Heart J. 2010;18:118-121.
8.
MalletRTBurtscherJRichaletJPMilletGPBurtscherM. Impact of high altitude on cardiovascular health: current perspectives. Vasc Health Risk Manag. 2021;17:317-335.
LalKSinghNKumarA, et al.Association of ischemic electrocardiographic changes in high-altitude areas with coronary angiography. Med J Armed Forces India. 2021;77(4):403-407.
11.
DoneganiEHillebrandtDWindsorJ, et al.Pre-existing cardiovascular conditions and high altitude travel. Consensus statement of the Medical Commission of the Union Internationale des Associations d’Alpinisme (UIAA MedCom) travel medicine and infectious disease. Travel Med Infect Dis. 2014;12(3):237-252.
12.
YanagawaYOmoriKTakeuchiI, et al.Cardiac arrest at high elevation with a favorable outcome. Am J Emerg Med. 2017;35:661.e5-661.e7.
13.
FaehDGutzwillerFBoppM; Swiss National Cohort Study Group. Lower mortality from coronary heart disease and stroke at higher altitudes in Switzerland. Circulation. 2009;120(6):495-501.
14.
Al-HuthiMARaja’aYAAl-NoamiMRahmanARA. Prevalence of coronary risk factors, clinical presentation, and complications in acute coronary syndrome patients living at high vs low altitudes in Yemen. Medscape Gen Med. 2006;8:28.
15.
LevineBDZuckermanJHdeFilippiCR. Effect of high-altitude exposure in the elderly: the Tenth Mountain Division study. Circulation. 1997;96(4):1224-1232.
16.
BurtscherMPonchiaA. The risk of cardiovascular events during leisure time activities at altitude. Prog Cardiovasc Dis. 2010;52(6):507-511.
17.
BurtscherM. Risk and protective factors for sudden cardiac death during leisure activities in the mountains: an update. Heart Lung Circ. 2017;26(8):757-762.
18.
LuksAMBeidlemanBAFreerL, et al.Wilderness Medical Society clinical practice guidelines for the prevention, diagnosis, and treatment of acute altitude illness: 2024 update. Wilderness Environ Med. 2024;35(1):2S–19S.
19.
BärtschPMaggioriniMRitterMNotiCVockPOelzO. Prevention of high-altitude pulmonary edema by nifedipine. N Engl J Med. 1991;325(18):1284-1289.