
Abstract
Purpose:
Dissatisfaction and an impaired quality of life after total knee arthroplasty (TKA) is often associated with postsurgical anterior knee pain (AKP). The underlying pathological mechanisms are not yet fully understood. Therefore, a multifactorial approach encompassing clinical and radiological parameters seemed reasonable and promising to investigate postsurgical AKP.
Methods:
In this cross-sectional study, 25 patients without and 25 patients with postsurgical AKP after unilateral TKA were randomly recruited from a larger cohort of patients. Multiple clinical and radiological parameters—including real-time shear wave elastography (SWE) to measure the patellar and quadriceps tendon elasticity—were acquired and subsequently associated with AKP. For statistical analysis, SPSS (IBM, version 25) was used.
Results:
In total 50 participants (58.0% men, mean age 63.42 years, mean body mass index 29.75 kg/m2), having different prosthetic designs implanted, were included. Independently of key covariates, the strength of the quadriceps muscle (p = 0.021), a thinner inlay (p = 0.041), and a lower position of the patella (p = 0.041) were associated with AKP. Although no correlation with AKP was found (p = 0.346, resp. p = 0.154), we observed significantly decreased Young’s modulus of the patellar and quadriceps tendons for the involved knee compared to the uninvolved knee (p < 0.001).
Conclusion:
In conclusion, quadriceps muscle strength, inlay thickness, and the patella position might be of particular relevance in avoiding postsurgical AKP. Future studies with larger sample sizes are needed to clarify the impact of quadriceps muscle strength and the postoperative patella position as well as the role of SWE as a personalized modifiable prediction marker.
Keywords
Introduction
High rates of satisfaction varying between 85.2% and 92.0% after total knee arthroplasty (TKA) have been reported. 1 –4 However, anterior knee pain (AKP) has been described by up to 30% of the patients after TKA, 5 and it has been strongly associated with patients’ dissatisfaction and impaired quality of life. 6 –9 Difficulties in standing after sitting on a chair, in walking up and downstairs, and in riding a bicycle are reported by patients suffering from AKP due to retropatellar or peripatellar pain, which limits their everyday lives. 10,11 Up to 50% of the revision surgeries after primary TKA are due to patellofemoral complications, 12 of which 1.9–7.8% of them are related to painful patellofemoral sensations. 13 –15 Despite numerous studies, the underlying pathology of AKP after TKA is not completely understood, and there are no clear correlations between clinical and radiological findings. 16 Due to the pronounced development of medical engineering methods, advanced diagnostic opportunities are applied in the research as well as the clinical setting. For example, the use of ultrasound (US) with more developed features—such as power Doppler (PD) and real-time shear wave elastography (SWE)—offers a good practical applicability without exposure to radiation. The SWE assesses quantitatively differences in tissue elasticity (stiffness) by using US that measures the shear wave velocity (m/s), which is generated by the US pulse. 17 Good to very good intra- and interobserver agreement for the SWE of the patellar and quadriceps tendon has been reported. 18 –20 Studies focusing on SWE observed that pathological clinical symptoms are often associated with “softer” tendons. 21 –23 So far, there are no studies that have used advanced US tools in the diagnosis and treatment of patients with AKP following TKA. Therefore, a multifactorial study approach seems promising to better understand the underlying pathological mechanisms of AKP. The aim of the present study was to investigate the associations of patients’ history, clinical as well as radiological parameters with the occurrence of postsurgical AKP.
Materials and methods
Participants
Patients with a minimum of 8 weeks postprimary or non-primary unilateral TKA with a minimum age of 18 years and the absence of neurological symptoms were included in the study. Patients with an inflammatory systemic disease (e.g. rheumatoid arthritis), impaired cognitive status, and a compromised cardiorespiratory fitness that could influence the clinical examination were excluded from this study. During their routine appointments at our inpatient clinic, patients with and without postsurgical AKP after TKA, meeting the criteria of inclusion, were randomly selected from a larger collective of TKA patients and invited to participate. We included an equal number of participants with and without AKP after TKA to achieve an adequate possibility for clinical and radiological comparability between these two groups. All patients gave their written and oral informed consent after receiving spoken and written information about the study. The study was approved by the local ethics committee (study number EK 072/17) and was conducted according to the principles found in the Declaration of Helsinki. Table 1 presents the demographic data of our study population.
Demographic, clinical, and radiological characteristics of participants.

PCL: posterior cruciate ligament; SD: standard deviation; TKA: total knee arthroplasty; CDI: Caton–Deschamps index; BMI: body mass index.
Medical history
The definition of AKP encompasses pain experienced in the area of the anterior knee and is a syndrome rather than a disease, 24 although an up-to-date and consistent definition is still lacking. 25 AKP in this study was defined as pain at the front and center of the knee. Information about a previous history of periprosthetic or septic infections and/or an implant exchanges was derived by a clinical evaluation. The thickness of the tibial inlay, more specifically the polyethylene liner construct, was retrieved from the individual surgical reports or, if available, from the prosthesis pass.
Knee Society clinical rating system
The “knee score” (Knee Society Score (KSS)) 26 and “the function score” (Knee Society Function Score (KSFS)) of the Knee Society clinical rating system, which is a validated scoring system 27 to assess the function of the artificial knee joint, 28 were determined.
Clinical examination
The function of the quadriceps muscle was tested according to the research of muscle function testing of Janda 29 and graded from 0 = plegie to 5 = normal muscle function. Additionally, the strength of the quadriceps muscle was measured by investigating the sitting to standing transfer from a chair. The latter variable was subdivided into (1) moving up freely, (2) moving up easily supported by their own hands, (3) moving up with difficulties supported by their hands, and (4) being unable to move up independently from a chair. The coronal alignment was determined during the clinical examination, which focused on the intercondylar and the intermalleolar distance and, thereby, specified the leg axis into neutral, varus, or valgus alignment. The range of motion was assessed using a goniometer applying the neutral zero method. The cruciate and collateral ligaments were tested as stable or instable, and instability was categorized into three grades. The collateral ligaments were tested at 0° and 30° flexion of the knee by applying valgus and varus stress.
Sonographic evaluation
Real-time SWE, B-mode US, and PD were used to examine the patellar and quadriceps tendon of the involved and uninvolved knee joint. Three modes of US imaging of the patellar and quadriceps tendon (SuperLinear™ SL 15-4, Supersonic Imagine, Aix-en-Provence, France) comparing the TKA with the contralateral knee were conducted: (1) US examination with B-mode, (2) US examination with PD to determine the modified Öhberg score, 30 and (3) real-time SWE. The conventional B-mode was applied to qualitatively examine the morphology, the thickness, the echogenicity, and the structure (e.g. the presence of calcifications or fascicle desintegrity) of the patellar and quadriceps tendon in the longitudinal section and; then, the tendons were subsequently categorized as pathological or nonpathological. 31,32 The PD was applied to assess the neovascularization of the patellar and quadriceps tendon in longitudinal sections. We also determined the modified Öhberg score using PD where the amount of neovascularization was quantified. 33 –35 To quantify the neovascularization of the tendon, we applied a modification of the original 5-grade scale (0–4) of the Öhberg score. 30 Thus, a modified 4-grade scale (0–3) was used (0 = no flow, 1 = paratendinous flow, 2 = 1–2 intratendinous vessels, and 3 = multiple intratendinous vessels). 36,37 SWE provides the opportunity to measure the elasticity of tendons in real time (E in kPa). 38 It was applied at the proximal, medial, and distal third of the patellar and quadriceps tendon in the strictly longitudinal as well as the transverse direction of the extended knee joint in a relaxed state of the tendons, as previously described. 18,39 Mean Young’s modulus was evaluated by placing a region of interest in the most rigid area of the tendon with a standardized diameter of 2 mm. Subsequently, the mean values of the SWE for the patellar and quadriceps tendon and the ratio (involved over uninvolved tendon) were calculated. In addition to the ratio of the SWE signal, the percentage difference between the uninvolved and involved patellar and quadriceps tendon was calculated (Table 2). All US examinations were performed by two radiologists with at least 5 years of experience in US imaging.
US characteristics of the participants.

AKP: anterior knee pain; kg: kilogram; kPa: kilopascal; m: meter; mm: millimeter; m/s: meter per second; PCL: posterior cruciate ligament; SD: standard deviation; TKA: total knee arthroscopy; SWE: shear wave elastography; US: ultrasound.
Caton–Deschamps index
The Caton–Deschamps index (CDI) was applied to describe the position of the patella, and it is calculated by measuring the ratio of the length of the patella tendon and the length of the patella joint area during a 30° knee flexion. 40,41 The physiological range of the ratio is between 0.6 and 1.3; hereby, a CDI >1.3 is defined as a patella alta, and a CDI <0.6 is defined as a patella baja (PB).
Radiographic evaluation of femoral and tibial components
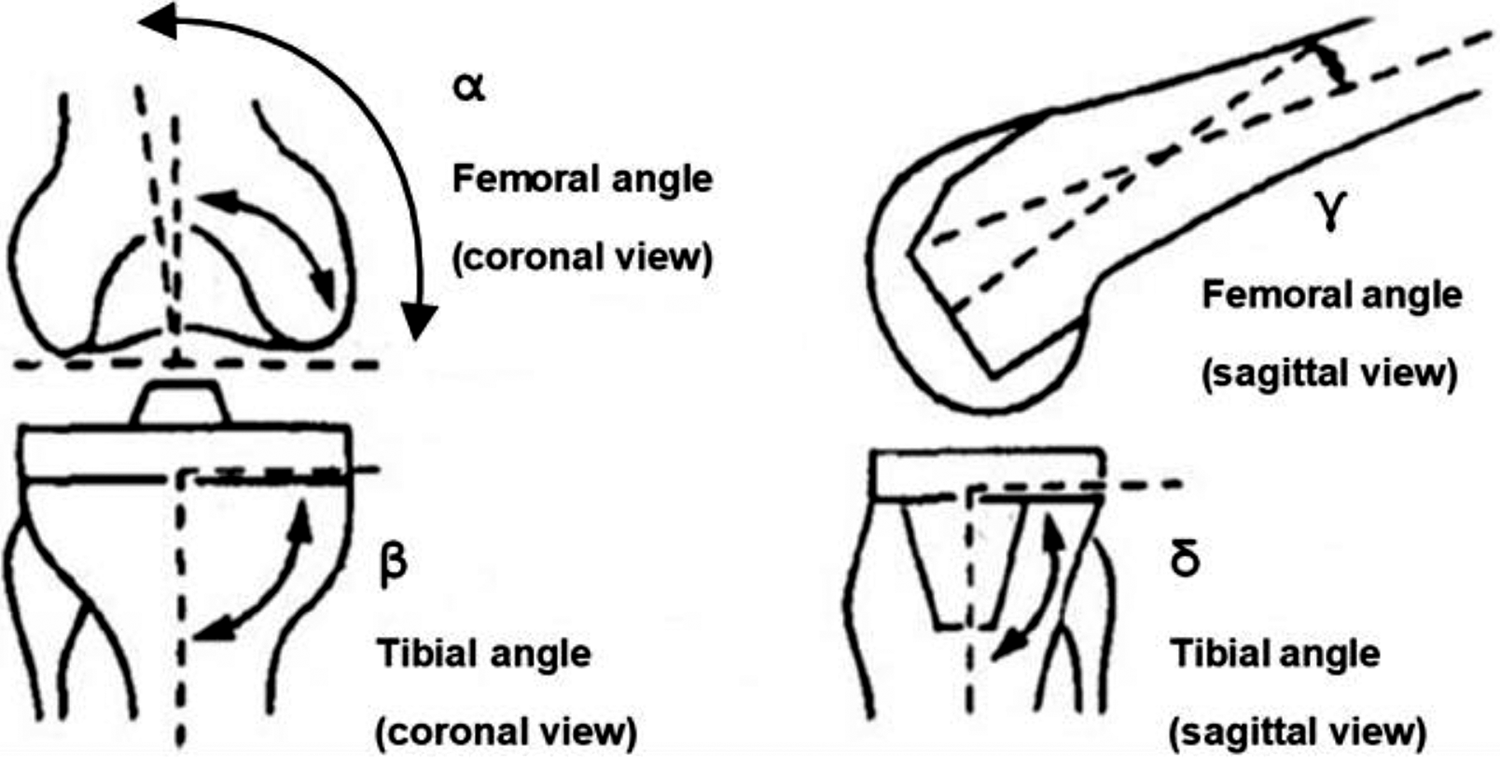
The alignment of the TKA was calculated according to the femoral and tibial axes. According to Ewald, 42 the axial alignment of the femoral and tibial components are assessed by measuring the femoral (α) and tibial angle (ß) using the coronal view as well as the lateral view to measure the angle γ of the femoral and the angle δ of the tibial component (Figure 1). Thus, the tibial slope of the TKA was retrieved by subtracting the angle δ from 90°.
Statistical analyses
For statistical analyses, SPSS (IBM, version 25) was used. The measured values of the SWE were saved in a picture archiving and communication system and were manually transferred to SPSS. For independent nominal data, the χ 2 test was used and for expected frequency <5, the exact Fisher’s test was used. The Mann–Whitney U test was applied for ordinal independent data. The two-sided Student’s t-test was used to compare independent samples, whereas the Welch t-test was automatically applied in case of variance heterogeneity. A binary logistic regression was conducted for the key variables of sex, body mass index (BMI), age, primary versus non-primary TKA, the thickness of the tibial inlay, the ratio of the patellar tendon (involved over uninvolved limb), the strength of the quadriceps muscle, the CDI, and the amount of months after surgery as independent variables and AKP as the dependent variable. All calculations were conducted with n = 50 unilateral TKA, including the characteristics of the participants and functional scores in relation to AKP.
Results
The 50 participants (29 men, mean age 63.42 years) had a mean BMI of 29.75 kg/m2 and mean time after surgery of 25.30 months (±27.05). No correlation was observed with either age or sex for AKP (p = 0.559, resp. p = 0.774). Also, AKP was not correlated with the number of months after surgery (p = 0.429) while the mean postoperative months for participants without AKP were 28.36 (±33.43) and for participants with AKP 22.24 (±19.00). The mean BMI for participants without AKP was 30.42 and 29.08 kg/m2 for participants with AKP (p = 0.390). Among the participants, 50.0% had a non-primary TKA, which was significantly correlated with AKP (p = 0.048). A posterior cruciate ligament (PCL)-sparing TKA was implanted in 30 (60.0%) participants, a constrained TKA was implanted in 15 (30.0%) participants, and a PCL-substituting TKA was implanted in 4 (8.0%) participants. The specific designs of the prostheses were not significantly associated with AKP (p = 0.241). Neither the mean extension deficit of 0.94° nor the mean range of flexion of 108.70° was associated with postsurgical AKP (p = 0.324, resp. p = 0.109). No correlation was observed between the coronal alignment (p = 0.349), the degree of coronal instability (p = 0.128–0.695), and the degree of the sagittal instability (p = 0.270–0.469) (not shown). The mean radiographic angles measured on X-rays were not significantly associated with AKP (p = 0.232–0.859). Ten participants had a history of infection or septic loosening/revision of the TKA, which was also not significantly associated with AKP (p = 0.480). A significant correlation with AKP (p = 0.041) was observed for the mean inlay thickness, which compared participants without AKP (10.45 mm) and with AKP (8.67 mm) (Table 3). A significantly stronger quadriceps muscle (p = 0.012) was observed in participants without AKP (mean 3.88) compared to the group with AKP (mean 2.92). This observation was supported by the fact that patients without AKP had a significantly easier time rising from a chair (p = 0.038). The KSFS and KSS were significantly lower (p < 0.001) in participants with AKP. A mean CDI of 0.77 was observed and associated with AKP (p = 0.001). Of the investigated TKAs, 18.8% (n = 9) had a PB (CDI < 0.6), which was associated with AKP (p = 0.001). In addition, lower KSS and KSFS were significantly associated with AKP (p = 0.040, resp. p = 0.001) (Table 3).
Clinical and radiological results.

CI: confidence interval; KSFS: Knee Society Function Score; KSS: Knee Society Score; mm: millimeter; SD: standard deviation; CDI: Caton–Deschamps index; PB: patella baja.
a Mean CDI < 0.6 in n = 9.
US examinations
When comparing the involved knee with the uninvolved knee a significant difference (p < 0.001) of the Young’s modulus (the tissue elasticity) was observed for the patellar (45.69 kPa, resp. 36.43 kPa) as well as quadriceps tendon (60.08 kPa, resp. 45.69 kPa). Neither the ratio (involved over uninvolved limb) nor the percentage difference (%) of the patellar nor the quadriceps tendon showed a significant association with the occurrence of AKP (p = 0.154–0.346) (Table 4). A larger difference in participants without AKP than in participants with AKP was observed for the percentage difference of the patellar and quadriceps tendon (p = 0.346, resp. p = 0.154). Additionally, a higher ratio of the patellar and quadriceps tendon being associated with AKP (Figure 2) was observed (p = 0.346, resp. p = 0.154). In other words, this larger difference and higher ratio indicate that softer patellar and quadriceps tendons are less associated with the development of postsurgical AKP. Pathological signs using the B-mode were observed in 94.0% of the patellar and in 92.0% of the quadriceps tendon of the involved limb. The uninvolved limb had a pathological B-mode in 28.0% of the patellar and in 4.0% of the quadriceps tendon. No association was observed between experiencing AKP and pathological signs in the B-mode for the patellar (p = 0.235) and the quadriceps (p = 1.0) tendon after TKA. The mean Öhberg score of the uninvolved limb was 0.16 for the patellar and 0.14 for the quadriceps tendon. No statistically significant correlation was found for the Öhberg score of the patellar and quadriceps tendon with AKP (p = 0.832, resp. p = 0.801). Figures 3 to 5 show sonographic B-mode/PD and real-time SWE images.
Results of the US examinations.

AKP: anterior knee pain; CI: confidence interval; SD: standard deviation; SWE: shear wave elastography; US: ultrasound.

To assess the postsurgical individual difference of the elasticity of the patellar and quadriceps tendon, examined by SWE, after a TKA, the ratio was calculated by dividing the involved by the uninvolved tendon. Subsequently, this ratio was compared to participants with and without AKP. The nonsignificant trend (p = 0.154–0.346) of an association between a higher ratio and experiencing AKP is observed. The error bars are representing one standard deviation of uncertainty. AKP: anterior knee pain; SWE: shear wave electrography; TKA: total knee arthroplasty.

Postoperative sonographic images of a patellar and a quadriceps tendon. The sonographic B-mode/PD images show a hypoechoic patellar tendon with intratendinous neovascularization (modified Öhberg score 2) and calcification (a) as well as intratendinous neovascularization (modified Öhberg score 3) of a quadriceps tendon (b). PD: power Doppler.

Postoperative sonographic image of a quadriceps tendon from a patient with postsurgical AKP. SWE demonstrates a semi-quantitative color-coded map displayed over a regular B-mode image. Real-time quantitative measurement within the circular ROI reveals a mean tendon stiffness of 166.55 kPa. AKP: anterior knee pain; SWE: shear wave electrography; ROI: region of interest.

Postoperative sonographic images of a patellar tendon. SWE semi-quantitative measurement reveals a turquoise color signal and a reduced mean tendon stiffness of 37.55 kPa accompanied by substantial pathological changes of the patellar tendon. SWE: shear wave electrography.
Multifactorial analyses of AKP
A logistic regression with AKP as the dependent and sex, BMI, age, primary versus non-primary TKA, the thickness of the inlay, the ratio of the patellar tendon (SWE of the involved over uninvolved limb), the strength of the quadriceps muscle, the CDI, and the time after surgery (months) as independent variables was executed (Table 5). This logistic regression was as a model (χ 2(9) = 24.256, p = 0.004, n = 39) statistically significant. The results of the multivariate analysis show that the statistically significant predictors for AKP subsequent to a TKA were the thickness of the inlay (odds ratio (OR) = 0.674), the strength of the quadriceps muscle (OR = 0.304), and the CDI (OR ≤ 0.001). In other words, a thicker inlay implanted, a stronger quadriceps muscle, and a larger CDI are correlated with experiencing less postsurgical AKP. Sex, BMI, age, primary or non-primary TKA, the ratio of the SWE patellar tendon, and the number of months after surgery were not statistically significant predictors of AKP after a TKA (p = 0.207–0.989). The Nagelkerke R 2 is 0.619; therefore, the latter logistic regression model shows a good explanatory power for the variance of the dependent variable of AKP.
Multivariate logistic regression for predictors of the dependent variable of AKP (n = 39).a

BMI: body mass index; B: partial regression coefficient; CI: confidence interval; OR: odds ratio; SE: standard error; TKA: total knee arthroplasty; SWE: shear wave elastography; CDI: Caton–Deschamps index.
a The model consists of sex, BMI, age, primary versus non-primary TKA, the thickness of the inlay, the ratio of the patellar tendon (SWE of the involved over uninvolved limb), the strength of the quadriceps muscle, the CDI, and the months after surgery as independent variables and the occurrence of AKP as the dependent variable. The reference for the regression coefficient of sex is female.
b p < 0.05: statistical significance.
Discussion
The present study investigated multiple variables regarding the prevalence of postsurgical AKP. The magnitude of variables demonstrated no clear correlation with postsurgical AKP, whereas some show statistically significant associations. In line with the current literature, the present study found that the patients’ age, sex, and BMI were not found to be predictive of AKP. 43 –45 Knee-specific characteristics—including the prosthetic design, the history of an infection of the knee prosthesis, the mean radiographic angles of the implanted TKAs, the US parameters of the SWE as well as the B-mode, and Öhberg score—were also not related to the occurrence of postsurgical AKP. Our finding that the prosthetic design is not associated with the development of AKP is supported by the meta-analysis of Li et al. 46 who reported for PCL-sparing and PCL-substituting TKAs similar clinical outcome regarding postoperative knee pain. Although there is no general consensus about the optimal alignment of the femoral and tibial components, there are several recommendations for optimal TKA component placement to avoid postsurgical knee pain and impaired knee function in daily living activities. 47 The mean angles of the present investigation correspond well with the recommendations for optimal TKA component placement suggested by Gromov et al. 47 As in the present study done, applying US to investigate tendons has proven to be more sensitive compared to magnetic resonance imaging, 48 and, therefore, it is reasonable to use to examine soft tissues. 49 The examination of PD US showed neovascularization in 63.2% of the patellar tendon and 69.4% of the quadriceps tendon for the involved side compared to 12.0% and 14.0% for the uninvolved side. Thus, the PD US of the patellar and quadriceps tendon were significantly more often defined as pathological for the involved compared to the uninvolved side. These US related findings, however, were neither in the B-mode nor in the feature of PD associated with AKP. Future studies with larger study populations are necessary to determine the relevance of pathological findings using US in relation to clinically apparent symptoms. For instance, the therapy of chronic painful Achilles tendinosis 30 and patellar tendinopathy 36 —namely sclerosing the neo-vessels with injections or topical application 50 of polidocanol—appeared to be effective and could be a treatment option in patients with AKP attributed to patellar or quadriceps tendinosis. During TKA implantation an irritation of the patellar and quadriceps tendons occurs, and, therefore, the subsequently observed neovascularization might be part of the physiological tissue repair, in particular short- to midterm postoperatively. 51 Comparable to the B-mode and PD, the applied SWE revealed that the patellar and quadriceps tendons of the uninvolved side were significantly “harder” (i.e. less elastic). To the best of our knowledge, this is the first study that uses SWE to investigate the presence of AKP in patients with TKA. We calculated a ratio that includes the patellar and quadriceps tendon of the involved limb to the patellar and quadriceps tendon of the uninvolved limb. The rationale behind this approach was to correct for age-related physiological changes of the elasticity of tendons, which has been previously applied for investigating patellar tendinopathies. 52 Notably, our observations point in the same direction as previous studies investigating patellar tendons, which reported higher patellar tendon elastic modulus in patients with patellar tendinopathies. 39,52 It needs to be considered that decreased elastic modulus and shear wave velocity values are reported in healthy elderly people, 18 and while showing a wide physiological range, the interindividual differences might rather be related to their physical condition in general. 53 Literature concerning normative age-related values and values adapted for certain physical training conditions (e.g. athletes vs. nonathletes) is missing. Therefore, to establish normative age-related values of different tendons of interest, further studies are needed that use multiple measurement time points investigating healthy individuals as well as subjects with sustained surgery. Dirrichs et al. 21 established SWE as a diagnostic tool for the early detection and monitoring of clinically relevant tendinopathies. However, SWE in the diagnosis and treatment of tendinopathies following TKA still needs to be evaluated and future studies will need to elucidate the role of (preoperative) SWE, and in particular the aforementioned ratio (involved over uninvolved limb), as a personalized predictive marker for postsurgical AKP and its impact as a potentially modifiable factor.
In line with the literature, 54,55 a prior history of revision surgery was associated with AKP and impaired functional outcome. Each surgical intervention adds up to a cumulative tissue injury and scar formation, which is hypothesized to be associated with concurrent increased activation as well as the intensity of the nociceptors being responsible for the experienced pronounced pain. 54,55 Furthermore, we observed that the strength of the quadriceps muscle, the ability to stand from sitting on a chair, the thickness of the tibial inlay, and a radiologically measured PB are associated with experiencing postsurgical AKP. Logistic regression revealed that the inlay thickness, the strength of the quadriceps muscle, and the CDI are independently from the sex, BMI, age, revision knee surgery, and the number of months after surgery associated with AKP. Several investigations pointed out the importance of the function of the quadriceps muscle as a predictor of functional abilities in patients undergoing TKAs, 56 –58 especially for the elderly. 59,60 The observed association of AKP with reduced strength of the quadriceps muscle underlines the necessity of strength training and appropriate physical therapy. To accomplish a more profound approach to address the often-observed weakness of the quadriceps muscle, Werner 61 , for instance, suggested a multiphasic approach, including an early correction of imbalance between the vastus medialis and vastus lateralis for physically active individuals with AKP. A significant association of the thickness of the tibial inlay with AKP was observed when comparing the samples and, in addition, as part of the logistic regression analysis as an independent variable, we found an independent association of the thickness of the tibial inlay with AKP, whereby participants having a thinner inlay implanted were more prone to experience postsurgical AKP. Multiple studies observed a correlation between different types and thicknesses of inlays and AKP. 62 –64 It is conceivable that thinner inlays are predisposed for instability due to a slackening of the ligaments, which, in turn, may be related to AKP. Therefore, thicker inlays may reduce the slacking; however, unpredictable results for polyethylene exchange only for prosthetic knee instability are reported with regard to pain and instability. 65 Furthermore, different studies reported an incidence of PB after TKA between 34% and 65%. 66 –68 By applying a modified Caton–Deschamps index (mCD), Prudhon et al. 69 observed a difference between pre and postoperative mCD of 0.19 and a lower patella in 81.7% of the cases. In line with our observations, Pfitzner et al. 70 reported a lower CDI (0.48; ±0.15) after TKA. Our results indicated that a CDI <0.6 (“patella baja”) measured by the CDI was significantly associated with lower KSS and KSFS scores. Potential complications of a PB are patellar impingement on the tibial polyethylene insert, 71 a painful limitation of knee flexion as a result of tightening of the collateral ligaments, 67,68 and diminished femoral rollback 72 ; therefore, it should be avoided.
We note several limitations with the present investigation. First, there is no singular definition of AKP, and to differentiate the patellofemoral pain syndrome (PFPS) is difficult. Similar to postsurgical AKP after TKA, an attempt to allocate postsurgical PFPS after TKA to an anatomical correlate was unsuccessful, and therefore, PFPS and AKP are used synonymously. 73 Furthermore, due to the rather small sample size and heterogeneous study population, a generalization of the results might be limited. We investigated a magnitude of clinical and radiographic factors, including the novel strategy of applying SWE in patients after TKA. Thereby, we tested the feasibility of the applied study protocol. Also, we aimed to identify especially relevant factors responsible for postsurgical AKP which can be applied in future studies; therefore, this work is best interpreted in the sense of a pilot study. In addition, it is noteworthy that we included patients at a rather early postsurgical stage. However, the number of months after surgery was nor correlated with AKP neither was the postsurgical time a significant independent predictor for the occurrence of AKP. Furthermore, a relevant portion of the participants underwent at least one revision surgery (50%) and only about two-third of the TKAs were PCL sparing. Future larger studies are necessary to draw conclusions from subgroup analyses consisting of primary and non-primary TKAs. However, in line with prior studies, 74,75 we did not find an association of AKP after TKA with the prosthetic design. Furthermore, it is not conclusively possible to clarify if the observed limited strength of the quadriceps muscle in participants with AKP is responsible for the postsurgical AKP or if the postsurgical AKP results in less loading of the leg, which impairs quadriceps muscle strength. To extend prior studies, 58 future studies may want to also focus on quadriceps muscle strength of the uninvolved limb considering the fact that patients tend to shift weight away from the operated limb. 76 Therefore, a causal relationship between postsurgical AKP and the ability to stand up from a chair cannot be finally drawn, and a careful interpretation of the obtained results is necessary. Due to radiation hygiene and conflicting literature regarding the impact of coronal alignment, we abstained from making whole leg radiographs, which, in turn, also accounts for the lack of availability of n = 9 radiological plain radiographs. Since preoperative misalignment of the leg axis (varus or valgus knee) is shown to be predictive for postoperative AKP, 77 future studies aiming to identify risk factors for postsurgical AKP may want to implicate whole leg radiographs to calculate the coronal TKA alignment. Furthermore, recently published large registry data, investigating the controversial issue of patellar resurfacing, indicate that unresurfaced knees are at higher long-term risk for revision surgery after primary TKA 78 ; therefore, future studies may also want to include patella resurfacing as an independent variable in multifactorial analyses.
Conclusion
Postsurgical AKP is prevalent and clinically relevant. With respect to an expected increase of TKAs by 143% by 2050 in the United States, 79 there is an absolute necessity for further investigations. This multifactorial analysis including the novel strategy of applying SWE as a diagnostic tool revealed that the identification of single variables that are likely to predict the occurrence of AKP is limited. Based on the results of this study, avoiding a PB postoperatively and preoperative conditioning of the quadriceps muscle may help to prevent the development of postsurgical AKP.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.