
Abstract
Background
It is not established whether patellar resurfacing is better than patellar non-resurfacing during total knee arthroplasty (TKA). This study was to compare the clinical outcomes between groups with patellar resurfacing and non-resurfacing during cruciate retaining (CR) TKA.
Methods
In this retrospective cohort study, subjects undergoing primary CR TKA for osteoarthritis between 2012 and 2019 were included. Of 500 subjects, 250 had patellar resurfacing (group 1) and 250 had patellar non-resurfacing (group 2) CR TKA. Knee society knee score (KSKS), knee society function score (KSFS), Western Ontario and McMaster Universities Osteoarthritis (WOMAC) scale, Kujala score, anterior knee pain, patellar compression test and range of motion (ROM) of the replaced knee were assessed and compared between the two groups.
Results
There were no significant differences in KSKS, KSFS, WOMAC scale, Kujala score, prevalence of anterior knee pain and ROM of the replaced knee between the two groups at the last follow-up (p > .05). Group 2 had more subjects with positive patellar compression test than group 1 at the last follow-up (p = .010).
Conclusions
Clinical and functional outcomes of the replaced knee were not different between patellar resurfacing and non-resurfacing groups. Anterior knee pain was significantly reduced after total knee arthroplasty regardless of patellar resurfacing.
Level of evidence
Retrospective cohort study, Level III.
Introduction
Total knee arthroplasty (TKA) is currently performed as a definite surgical option for end stage osteoarthritis of the knee. Knee osteoarthritis generally affects the femorotibial joint as well as the patellofemoral joint. Widely implemented options of patellar management are resurfacing and non-resurfacing with or without deafferentation of the patella (electrocautery around patella). Some surgeons resurface all the patella during TKA while others do it selectively. Some other surgeons prefer to retain patellar surface even when the cartilage is severely degenerated. Proponents of patellar resurfacing point out its cost-effectiveness, lower rate of revision and less anterior knee pain. 1 However, patellar resurfacing has potential disadvantages of patellar fracture, implant failure, patellar tendon injury and patellar clunk syndrome.2–5 Advocates of patellar retention insist that patellar resurfacing has no advantages in functional outcomes, revision rates or healthcare cost. 6 Whether the patella should be resurfaced or retained during TKA remains controversial. 7
The objective of this study was to compare the clinical outcomes between patellar resurfacing group and non-resurfacing group after cruciate retaining TKA (CR TKA). Null hypothesis of this study was that clinical outcomes of patellar non-resurfacing TKA was comparable to those of patellar resurfacing TKA.
Materials and methods
Subjects
This was a retrospective cohort study reviewing clinical records of subjects who underwent primary CR TKA for osteoarthritis of Kellgren-Lawrence grade 3 or 4 by a single experienced orthopaedic surgeon in our institute between 2012 and 2019. This study was approved by the IRB of our institute. Of 1219 replaced knees reviewed, revision TKA, posterior cruciate ligament substituting TKA, those with inflammatory or neuropathic arthropathy, history of patellar fracture or previous major knee surgery and those who did not have follow-up for at least 2 years were excluded (Figure 1). Regardless of the severity of chondral degeneration, the patella was resurfaced between 2012 and 2016 (group 1) and retained between 2017 and 2019 (group 2). Subjects in group 2 were matched 1:1 with each one of the subjects in group 1 on sex and age (±3 years). Follow-up period of the subjects in group 1 were also matched with those of each one of the subjects in group 2 (±6 months). Flow diagram of the subjects.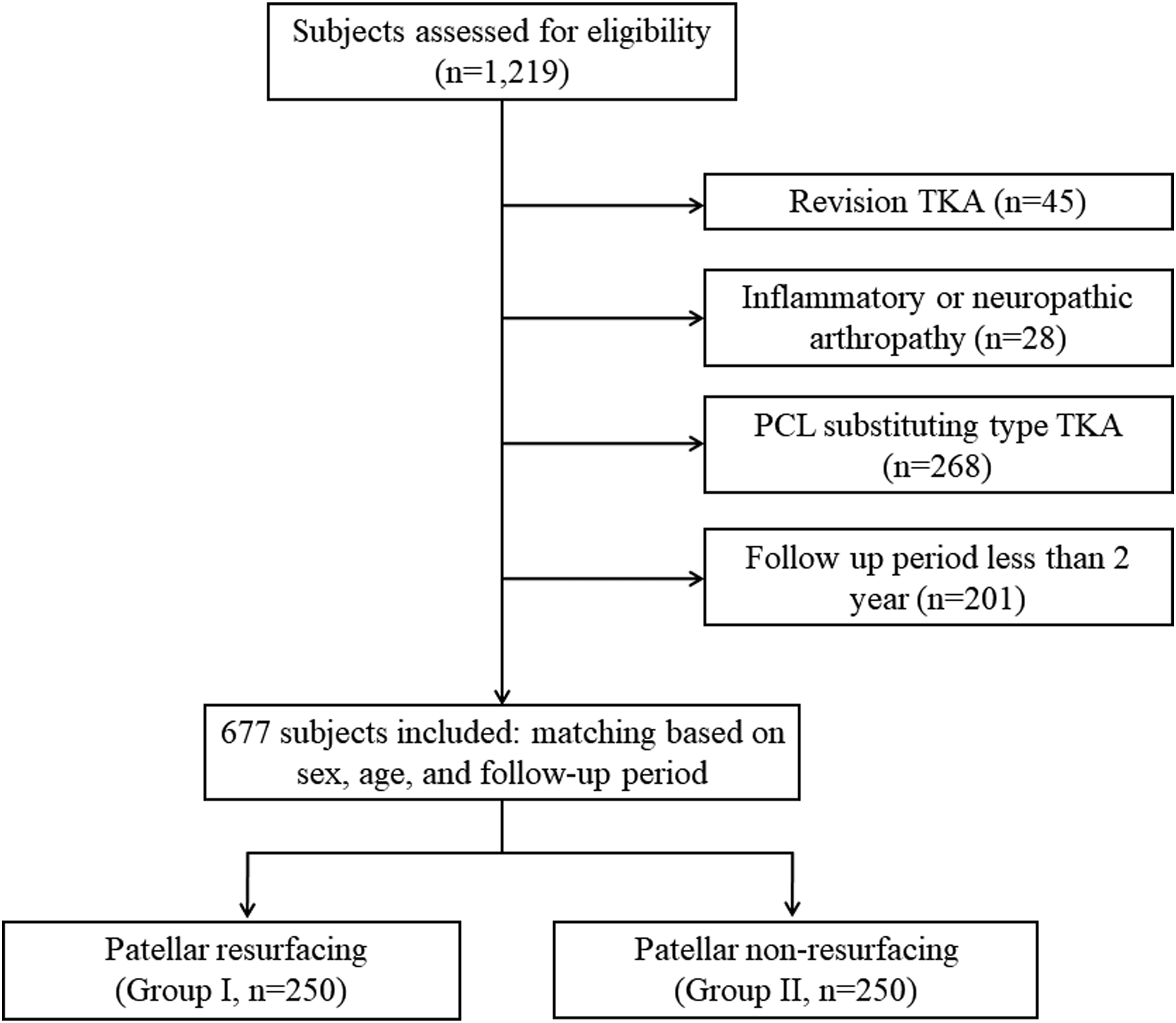
Operative technique
All subjects underwent cemented TKAs with consistent surgical technique through midline skin incision, medial parapatellar arthrotomy and patellar eversion. Chondral lesion of the patella was graded according to the Outerbridge classification system. 8 The valgus cut angle of the distal femur was set at 5–8° to create a neutral mechanical axis depending on the hip-knee-femoral shaft angle measured on preoperative long leg standing antero-posterior radiograph. Proximal tibial cut was perpendicular to the shaft with the posterior slope of 3–5°. Surgery was conducted using a modified measured resection technique. Antero-posterior femoral resection was performed using an anterior referencing cutting guide. Posterior cruciate ligament was released to balance the flexion and extension gaps if necessary. Group 1 included subjects with patellar resurfacing after preparation of the femur and tibia according to instructions of manufacturers. Patellar resurfacing was performed with a freehand technique, removing bone of the same thickness as the prosthetic component and accepting up to 1 mm over- or under-resection (measured with calipers before and after resection). However, the thickness of the remaining patella was made to be at least 12 mm or more. The onlay patellar component was all-polyethylene and symmetrical dome-shaped with three pegs. Group 2 included subjects with patellar non-resurfacing CR TKA. Osteophytes around the patella were resected. Deafferentation of the patella with electrocauterization was not performed for any subject. Patellofemoral articulation was assessed with “no thumb technique” throughout the range of motion (ROM) with the tourniquet deflated. If any of the patellar maltracking such as subluxation, dislocation or elevation of the medial edge of the patellar component was observed, lateral retinaculum was released to optimize patellar tracking, which was uniformly performed using inside-out technique, 1cm lateral from the patellar margin. The arthrotomy was closed with simple interrupted sutures. Drainage tube was removed on postoperative day 2.
A standardized rehabilitation program was carried out postoperatively. Crutch- or walker-assisted ambulation and continuous passive motion exercise were started on the second postoperative day. Intermittent pneumatic calf compression was applied to prevent deep vein thrombosis for 5–7 days. Oral or parenteral chemoprophylaxis for deep vein thrombosis was not administered. Discharge disposition was either to a community hospital or a rehabilitation facility.
Clinical and radiographic assessments
Merchant classification of patellofemoral arthritis.

Outerbridge classification.

Statistical analysis
All statistical analyses were done using SPSS ver. 23.0 software (IBM Inc., Armonk, NY, USA). Means and standard deviations were used to describe data. Radiographic assessment of patellofemoral arthrosis and intraoperative chondral assessment of patella were performed by two orthopaedic surgeons. Interobserver reliability was assessed based on intraclass correlation coefficient (ICC) with 95% confidence interval. Intraclass correlation coefficients were more than 0.85 for all parameters. Values measured by the senior surgeon were used for statistical analyses. Comparisons of outcomes between two groups were conducted using independent t-test, repeated measured ANOVA test and Chi-square test. Correlation analysis between two independent nonparametric variables was conducted using spearman correlation test. p value less than .05 was considered significant.
Results
Demographics of the subjects in each group.

1chi-square test.
2independent t-test.
3Biomet Inc., Warsaw, IN, USA.
4DePuy Synthes, Warsaw, IN, USA.
5DePuy Synthes, Warsaw, IN, USA.
6Zimmer, Warsaw, IN, USA.
7Zimmer, Warsaw, IN, USA.
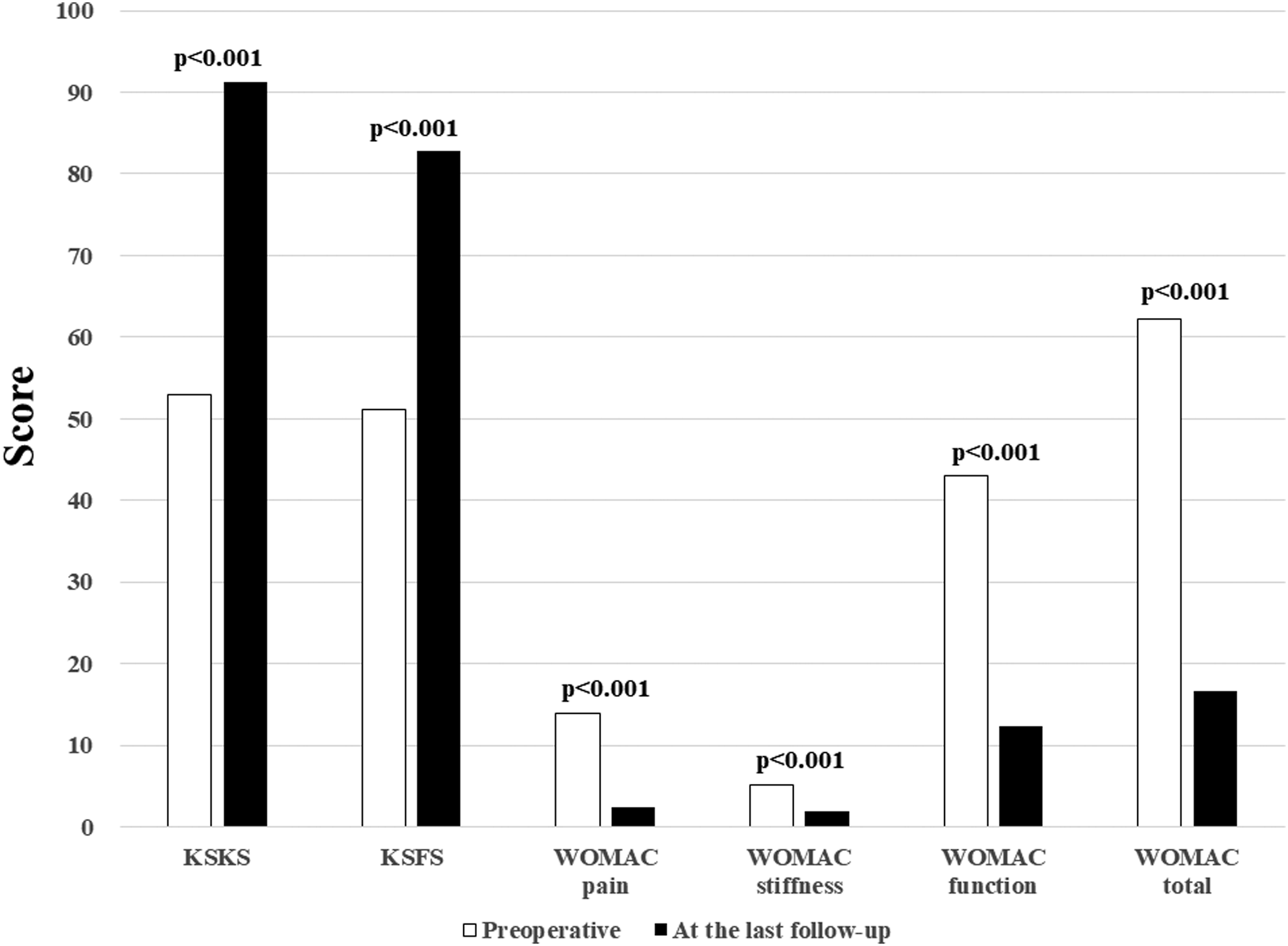
Patient-reported outcome measures preoperatively and at the last follow-up.

Range of motion of replaced knee preoperatively and at the last follow-up.
Comparisons of preoperative variables between two groups.
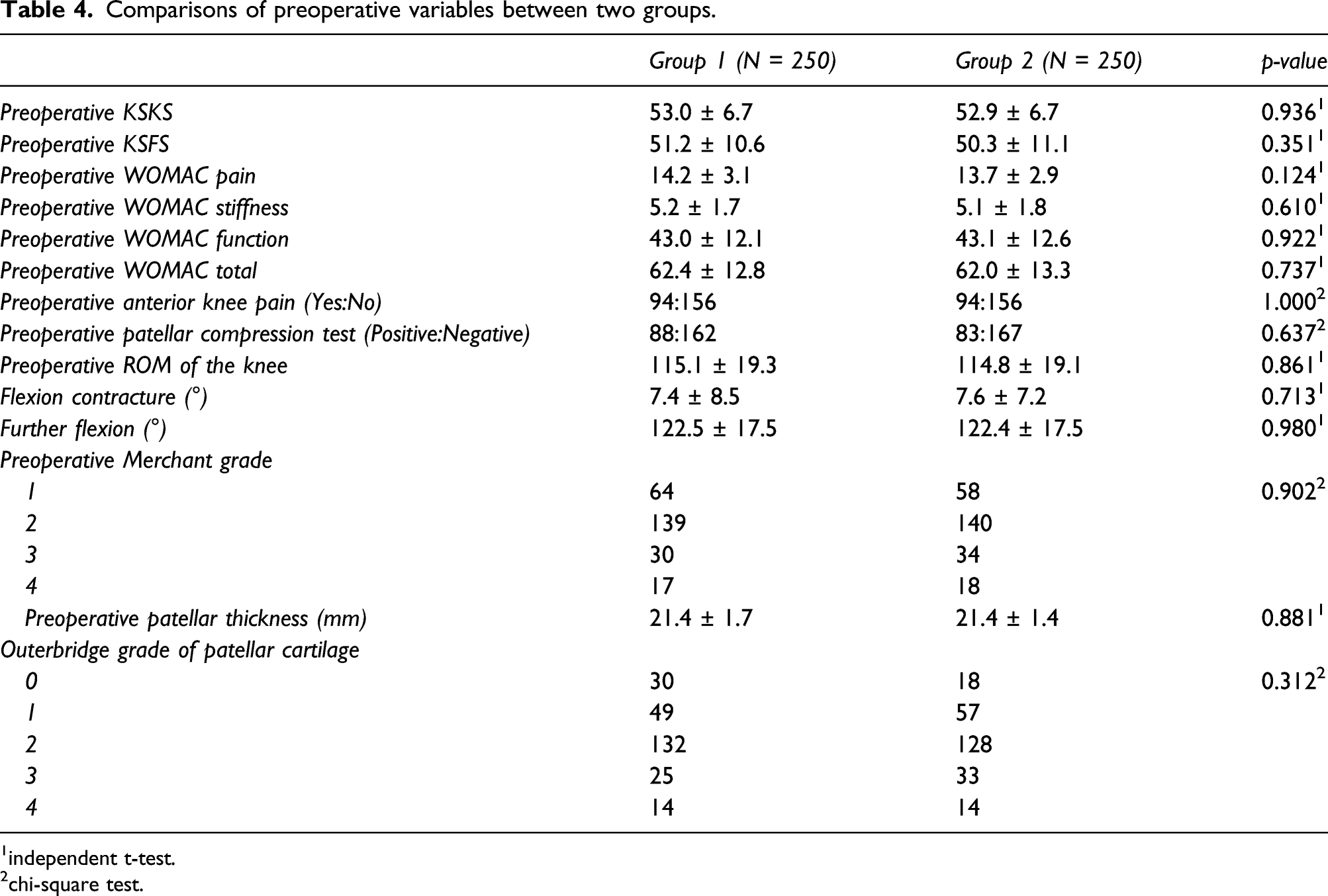
1independent t-test.
2chi-square test.
Evaluation of patellofemoral articulation according to preoperative anterior knee pain.

chi-square test.

Prevalence of anterior knee pain preoperatively and at the last follow-up.
Comparisons of postoperative outcomes between two groups.

1repeated measured ANOVA test.
2independent t-test.
3chi-square test.
During follow-up, two subjects in group 1 developed patellar osteonecrosis without a trauma history. One subject in group 1 who had patellar fracture after falling down underwent open reduction and fixation. One subject in group 2 who developed spontaneous patellar tendon rupture underwent tendon repair. Two subjects in group 2 who developed periprosthetic joint infection underwent subsequent operation. These six subjects with serious postoperative complications were excluded from statistical analyses.
Discussion
The most important finding of this study was that postoperative outcomes such as KSKS, KSFS, WOMAC scale, Kujala score, prevalence of anterior knee pain and ROM of the replaced knee were not significantly different between patellar resurfacing and non-resurfacing groups.
Total knee arthroplasty is one of the surgical options to relieve pain and to restore function to an arthritic knee. This study revealed that both groups showed statistically significant improvements in KSKS, KSFS, WOMAC scale, anterior knee pain and joint mobility after TKA. Resurfacing the patella during TKA remains a controversial issue. Proponents of patellar resurfacing point out its lower reoperation rates, less pain on anterior knee and cost-effectiveness.1,10,11 Longo et al. 12 have concluded that patellar resurfacing TKA performs better than non-resurfacing TKA in their meta-analysis. Migliorini et al. 13 have also stated that patellar resurfacing TKA performs superior and shows lower rate of anterior knee pain and reoperation. Reported rates of anterior knee pain range from 0 to 47% in the patellar resurfacing group,14–16 and from 0 to 43% in the patellar non-resurfacing group.14,17 Several studies have concluded that about 10% of patients would still have anterior knee pain after TKA regardless of patellar management.18,19 In the present study, the proportion of postoperative anterior knee pain was not significantly higher in the patellar non-resurfacing group than in the resurfacing group (7.6% vs. 4.4%). There was no revision of secondary patellar resurfacing due to serious anterior knee pain in either group during the follow-up.
Some studies have shown that anterior knee pain and revision rate are higher in the patellar resurfacing group.3,20 When complications related to the extension mechanism occur after patellar resurfacing TKA, management may become more difficult. Kaseb et al. 21 have stated that patellar resurfacing does not lead to decreased patellar crepitus or enhanced clinical outcomes of TKA. Grassi et al. 7 concluded that patellar resurfacing is not superior to non-resurfacing in their meta-analysis. Chen et al. 22 stated that the benefit of patellar resurfacing is limited although it can decrease the risk of reoperation after TKA. Migliorini et al. 13 stated that patellar non-resurfacing TKA group shows better ROM than resurfacing TKA group. The present study showed that there were no significant differences in patient-reported outcome measures such as KSKS, KSFS, WOMAC scale or joint mobility between patellar resurfacing and non-resurfacing groups.
Besides excision of osteophyte and smoothening of articular surface, several techniques have been introduced to manage the patella in non-resurfacing TKA such as electrocautery around the patella, drilling and facetectomy.23,24 However, Cheng et al. 25 found no evidence either for or against electrocautery compared with non-electrocautery in TKA after conducting meta-analysis. Xie et al. 26 have also found no statistical significance in outcomes between patellar denervation group and no-denervation group after 1 year follow-up. In the present study, only excision of significant osteophytes around the patella was performed while other patelloplasty or electrocautery was not conducted. We speculate that medial denervation through medial parapatellar arthrotomy might play a part in reducing anterior knee pain. Maralcan et al. 27 stated that superomedial and superolateral nerves are important for patellar innervation in a cadaveric study. Møller and Helmig 28 have improved patellar pain syndrome through medial denervation in more than half of subjects.
Cho et al. 29 stated that patellofemoral arthritis is associated with anterior knee pain before TKA. On the contrary, some other studies have concluded that the severity of radiographic findings of patellofemoral arthritis is not directly related to anterior knee pain.30,31 The present study revealed that radiologically degenerative change of patellofemoral joint was related to preoperative anterior knee pain. It also revealed that gross findings of patellar cartilage at the time of surgery were related to preoperative anterior knee pain. These results indicate that anterior knee pain is caused by chondral lesion of the femoral trochlea as well as that of the patella. However, Seo et al. 32 stated that there is no association between the severity of the patellar articular defect and resurfacing in terms of clinical or functional outcomes in their retrospective study.
There was no significant difference in the flexion angle of the replaced knee between patellar resurfacing and non-resurfacing groups at the last follow-up in the present study. Knee Society Scores and WOMAC scale were also similar between the two groups.
During study period some complications such as patellar osteonecrosis, patellar fracture and patellar tendon rupture have been occurred. Management may be difficult when there is a problem with the extensor mechanism after TKA. 33 Especially, transosseous fixation through the resurfaced patella is challenging. 34 The authors thus suggest that, in consideration of additional surgery due to extensor mechanism-related complications, patellar non-resurfacing TKA is performed regardless of patella cartilage degeneration during primary TKA. Patellar clunk syndrome is one of complications after patellar resurfacing TKA. Some authors have suggested etiologies such as high position of the patellar component, inadequate synovial tissue debridement at the upper pole of the patella, joint line change more than 8 mm and specific implant design.35–38 However, no patellar clunk syndrome was found during follow-up in the present study.
This study has some limitations. First, the follow-up period was short. Although clinical and functional outcomes are not significantly different between the two groups in terms of patient-reported outcome measures, anterior knee pain might increase as time goes on and functional outcomes may worsen accordingly. Longer period of follow-up might be needed to compare the long-term complications. However, many studies have stated that results at 1–2 years after primary or revision surgery are similar to those at 5 or 10 years postoperatively.39,40 Another shortcoming of this study was that implants used in this study were not homogenous.
Conclusions
Clinical and functional outcomes such as KSKS, KSFS, WOMAC scale, Kujala score, prevalence of anterior knee pain and ROM of the replaced knee were not significantly different between patellar resurfacing and non-resurfacing groups. Anterior knee pain was significantly reduced after TKA regardless of patellar resurfacing.
Footnotes
Author contributions
The study design was developed by JHN. NYK and KIS collected the data. Data analysis was performed by JHN. All authors contributed to the writing of the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the hospital Institutional Review Board (IRB).
Informed consent
Not applicable. Retrospective study design.