
Abstract
Keywords
Introduction
Idiopathic scoliosis (IS) is the most common form of structural scoliosis, accounting for 80–90% of scoliosis cases, with an incidence of 1.5% to 16% in the general population.1,2 For patients unresponsive to conservative treatments such as bracing or physical therapy, 3 surgical correction and spinal fusion become necessary. 4 Osteotomy procedures, particularly Grade I and II as classified by Schwab et al.,5,6 are frequently employed to enhance spinal mobility and facilitate deformity correction. However, while higher-grade osteotomies can improve correction, they are associated with increased risks of complications, highlighting the need for careful procedure selection
Spinal flexibility has emerged as a key independent predictor of surgical correction outcomes in IS. 7 Reduced flexibility is linked to lower correction rates, often requiring higher-grade osteotomies. Conversely, in patients with greater flexibility, the correction achieved by Grade I and II osteotomies may be similar, but Grade II procedures carry a higher complication risk and may not always be warranted.
Given these considerations, guiding osteotomy selection based on spinal flexibility could optimize surgical outcomes. This study aims to establish a predictive model incorporating spinal flexibility and osteotomy grade, to identify a flexibility threshold that informs surgical decision-making. We hope this approach will help maximize correction rates while minimizing complications in IS patients.
Methods and materials
Patient selection and data collection
We retrospectively reviewed the medical records of patients with IS who underwent posterior osteotomy surgery at our hospital between 2018 and 2023. Two types of osteotomy procedures were included in this study: Facet Joint Osteotomy (FJO, Grade I osteotomy), involving resection of the inferior articular processes and joint capsule at the target level, and Ponte Osteotomy (PO, Grade II osteotomy), involving resection of both articular processes as well as the lamina and ligamentum flavum. The selection of osteotomy technique was based solely on the clinical experience and established practice preferences of two senior spine surgeons.
Inclusion criteria were as follows: (1) diagnosis of IS; (2) treatment with posterior osteotomy surgery (FJO or PO) at our hospital between 2018 and 2023; and availability of complete clinical and radiographic data (including preoperative and immediate postoperative images).
Exclusion criteria included: (1) non-IS (such as congenital, neuromuscular, or syndromic scoliosis); (2) previous spinal surgery; (3) severe comorbidities or contraindications to surgery; (4) incomplete clinical or radiographic data; and (5) other spinal diseases affecting spinal flexibility or surgical outcomes (e.g., ankylosing spondylitis, severe osteoporosis).
Baseline demographic and clinical data were collected for all patients, including gender, age, number of surgical segments, preoperative Cobb angle, and immediate postoperative Cobb angle. The surgical correction rate was calculated as the ratio of the immediate postoperative curve correction to the preoperative Cobb angle. To evaluate spinal flexibility, preoperative X-rays bending toward the convex side were obtained, and the Cobb angle was measured. Spinal flexibility was then calculated as the ratio of the correction of the curve on bending radiographs to the Cobb angle in the standing position.
Statistical Analysis
To compare baseline characteristics between the FJO and PO groups, we applied the t test for continuous variables and the chi-square test for categorical variables. Statistical significance was defined as p < .05.
To investigate whether spinal flexibility could serve as an independent predictor for selecting the surgical method, we performed Spearman’s rank correlation analysis and Pearson correlation analysis to evaluate the correlations between spinal flexibility and other potential influencing factors, including age, gender and preoperative Cobb angle. Furthermore, multivariate linear regression analysis was performed to evaluate whether spinal flexibility is an independent predictor of correction rate after adjusting other preoperative parameters (age, gender, and preoperative Cobb angle).
To further explore the relationship between spinal flexibility and surgical correction outcomes, we constructed linear regression models for each group, with spinal flexibility as the independent variable and surgical correction rate as the dependent variable. To determine the threshold of spinal flexibility, we employed restricted cubic spline (RCS) analysis. By plotting RCS curves of spinal flexibility against the correction rate for both surgical methods, we identified the inflection point that may serve as a critical threshold.
Subsequently, we validated the consistency and correlation of surgical methods with correction outcomes both before and after the identified inflection point using Spearman’s rank correlation analysis.
Complication analysis
To examine the differences in surgical complications between the two methods, we compared the following perioperative parameters between the FJO and PO groups: total intraoperative blood loss (mL), average blood loss per segment (mL), postoperative hospital stay (days), and extubation time (days). These outcomes were used to assess the severity and frequency of complications associated with each surgical approach. The normality of continuous variables was assessed using the Shapiro–Wilk test. Data with a normal distribution are presented as mean ± standard deviation (SD), and those with a non-normal distribution are presented as median (interquartile range, IQR). The Mann-Whitney U test was used for non-normally distributed variables, and the independent t test for normally distributed variables.
All statistical analyses were performed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA) and R version 4.3.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
A total of 77 patients were included in the study, with 41 undergoing FJO and 36 undergoing PO. A schematic representation of the patient selection process is provided in Figure 1. The baseline characteristics of the two groups are summarized in Table 1. There were no significant differences in preoperative baseline characteristics between the two groups. The FJO group had a significantly greater number of fused segments compared to the PO group (p < .001), while the surgical correction rate was significantly lower in the FJO group than in the PO group (p = .033). Patient selection flowchart. Flowchart illustrates the inclusion and exclusion criteria for the study cohort. A total of 77 IS patients were divided into two groups based on osteotomy techniques: facet joint osteotomy (FJO, n = 41) and ponte osteotomy (PO, n = 36). Comparison of basic data between FJO group and PO group.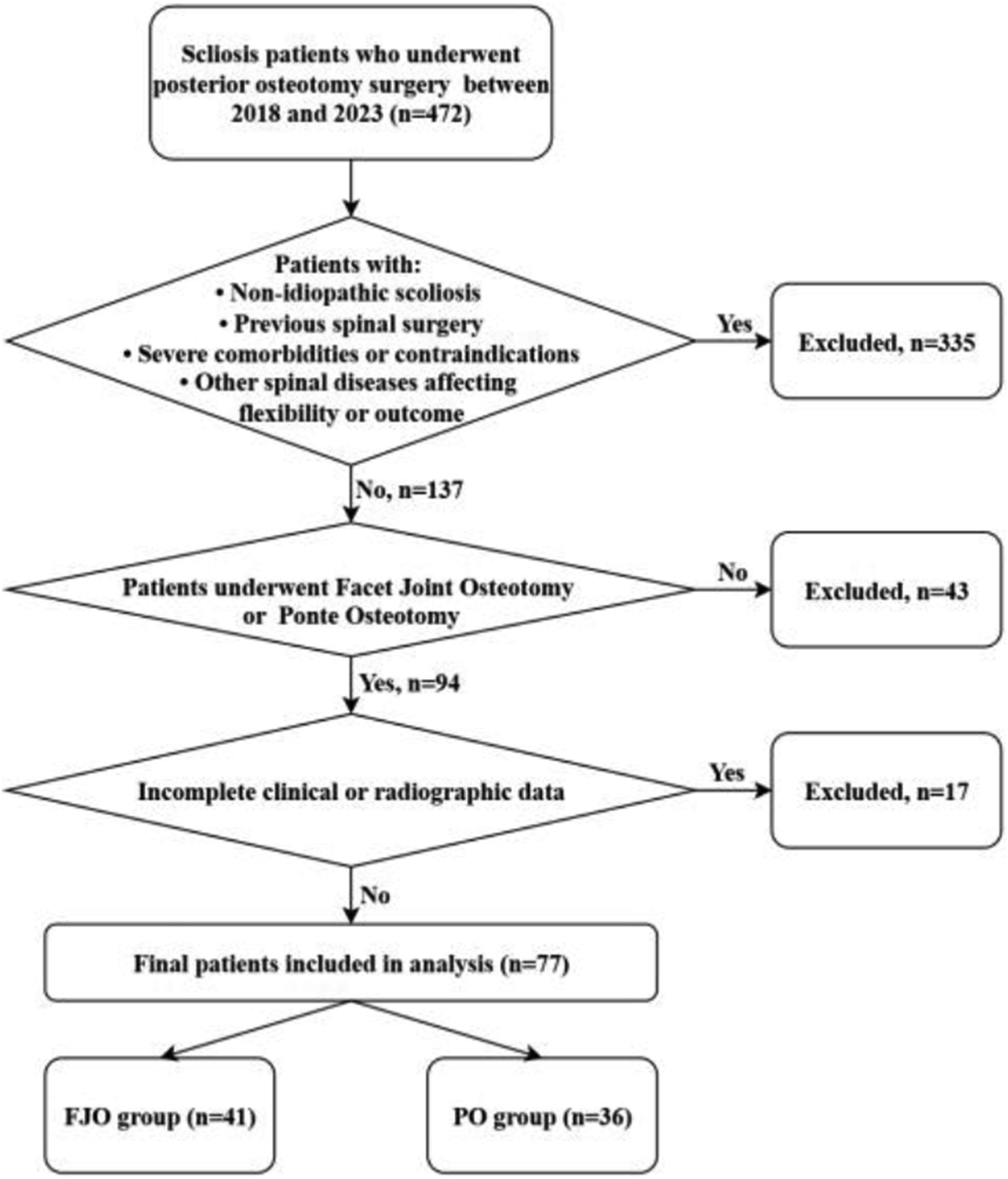

Pearson correlation analysis of preoperative variables and flexibility.


Correlation between age and spinal flexibility. Scatter plot showing the negative correlation between age and spinal flexibility (r = −0.633, p < .001). Younger patients tend to have higher spinal flexibility, as indicated by the downward trend.
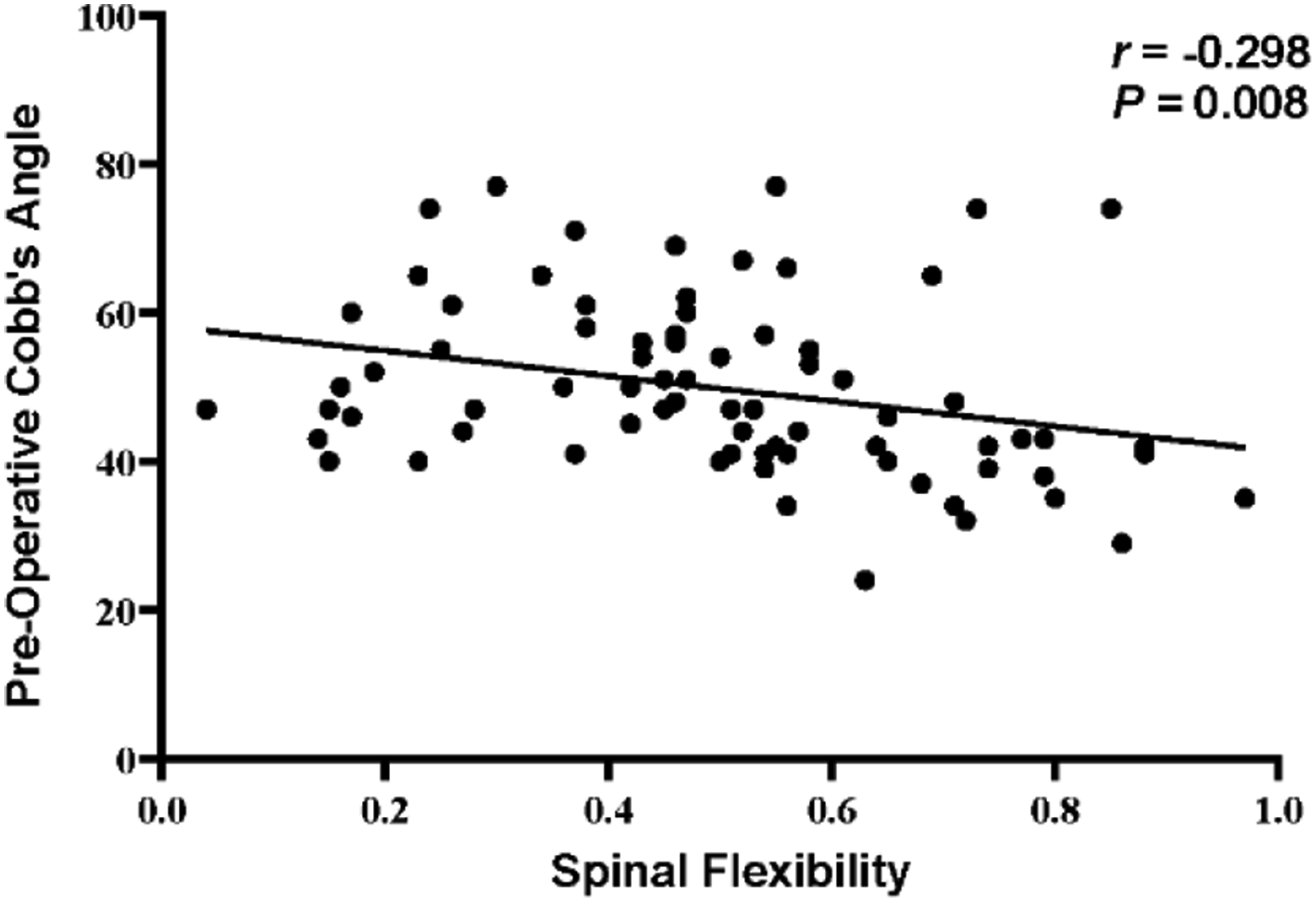
Correlation between preoperative Cobb’s angle and spinal flexibility. The scatter plot shows a weak negative correlation between preoperative Cobb’s angle and spinal flexibility (r = −0.298, p = .008). Patients with lower Cobb’s angles tend to exhibit higher spinal flexibility.
Multivariate linear regression analysis of predictors for surgical correction rate.

The fitting curve analysis is shown in Figure 4, where both groups exhibited an upward trend. For patients with poor spinal flexibility, the surgical correction rate was significantly higher in the PO group compared to the FJO group. As flexibility improved, the correction rates of the two groups converged and eventually stabilized. Results of the RCS trend analysis are shown in Figure 5. The vertical axis (β) represents the regression coefficient of spinal flexibility on the correction rate, reflecting the strength and direction of their relationship. As depicted, spinal flexibility and correction rate were positively correlated. Within a specific range, the impact of spinal flexibility on the correction rate increased progressively. However, beyond a certain threshold, the impact plateaued and subsequently diminished. The mean inflection point of the two curves was determined to be 0.657. Fitted curves of spinal flexibility and orthopedic rate. Fitted curves illustrate the relationship between spinal flexibility and orthopedic rate for the FJO group (red line) and the ponte group (blue line). The analysis shows that the ponte group achieves higher orthopedic rates at lower spinal flexibility, while both groups converge to similar outcomes as flexibility increases. Shaded areas represent 95% confidence intervals. Restricted cubic spline (RCS) analysis of spinal flexibility and orthopedic rate. RCS analysis showing the relationship between spinal flexibility and orthopedic rate, represented by regression coefficients (β) with 95% confidence intervals for the FJO group (blue line) and PO group (pink line). The curves illustrate that the impact of spinal flexibility on orthopedic rate increases progressively up to a plateau, with both groups showing similar trends.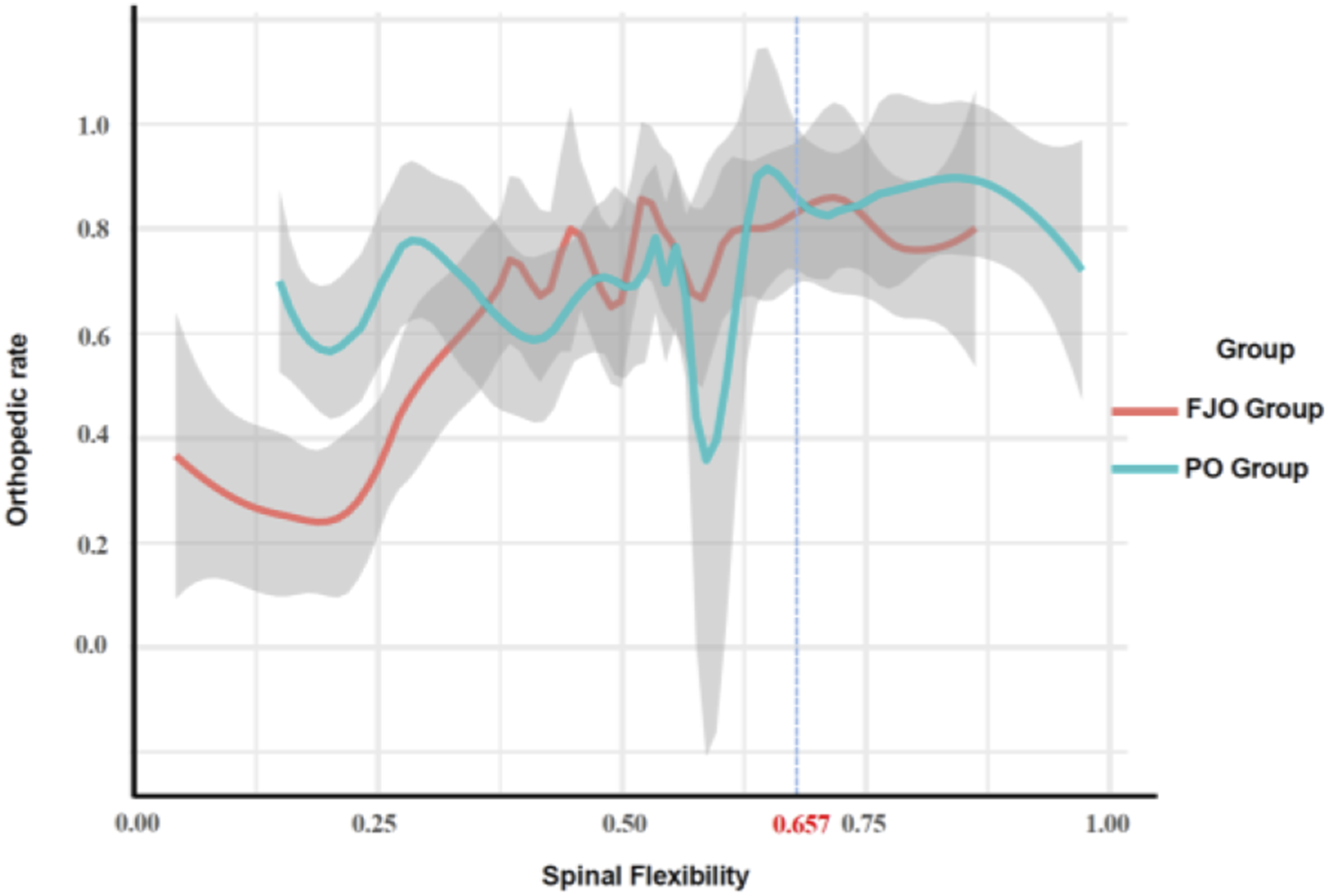

Spearman correlation analysis before and after the threshold revealed distinct trends. When flexibility was <0.657, the surgical method was positively correlated with the overall correction rate (r
s
= 0.591, p = .001). In contrast, when flexibility was ≥0.657, no significant correlation was observed between the surgical method and the overall correction rate (r
s
= 0.119, p = .409). To more intuitively illustrate the difference in surgical outcomes between the two osteotomy techniques when spinal flexibility is favorable, we present Figure 6. This figure shows two patients with similar curve characteristics and good spinal flexibility: Patient A underwent FJO, while Patient B underwent PO. As shown, there was no significant difference in postoperative correction between the two techniques. This further supports our conclusion that comparable correction can be achieved with either approach in patients with good spinal flexibility. Pre- and postoperative radiographs of two IS patients (same Lenke curve) Treated with FJO and PO Osteotomy. (A and B) show preoperative full-spine radiographs (A1, B1), preoperative bending films (A2, A3, B2, B3), and postoperative full-spine radiographs (A4, B4) of two IS patients. For Patient (a) T6–12 Cobb angle 43°, T12–L4 45°; after bending, 14° and 10°, flexibilities 0.674 and 0.778, postoperative correction rates 0.930 and 0.933, FJO osteotomy was performed. For Patient (b) T6–12 Cobb angle 33°, T12–L4 40°; after bending, 5° and 7°, flexibilities 0.848 and 0.825, postoperative correction rates 0.818 and 0.750, PO osteotomy was performed. Both had Lenke type 5 curves with good flexibility and achieved similar correction.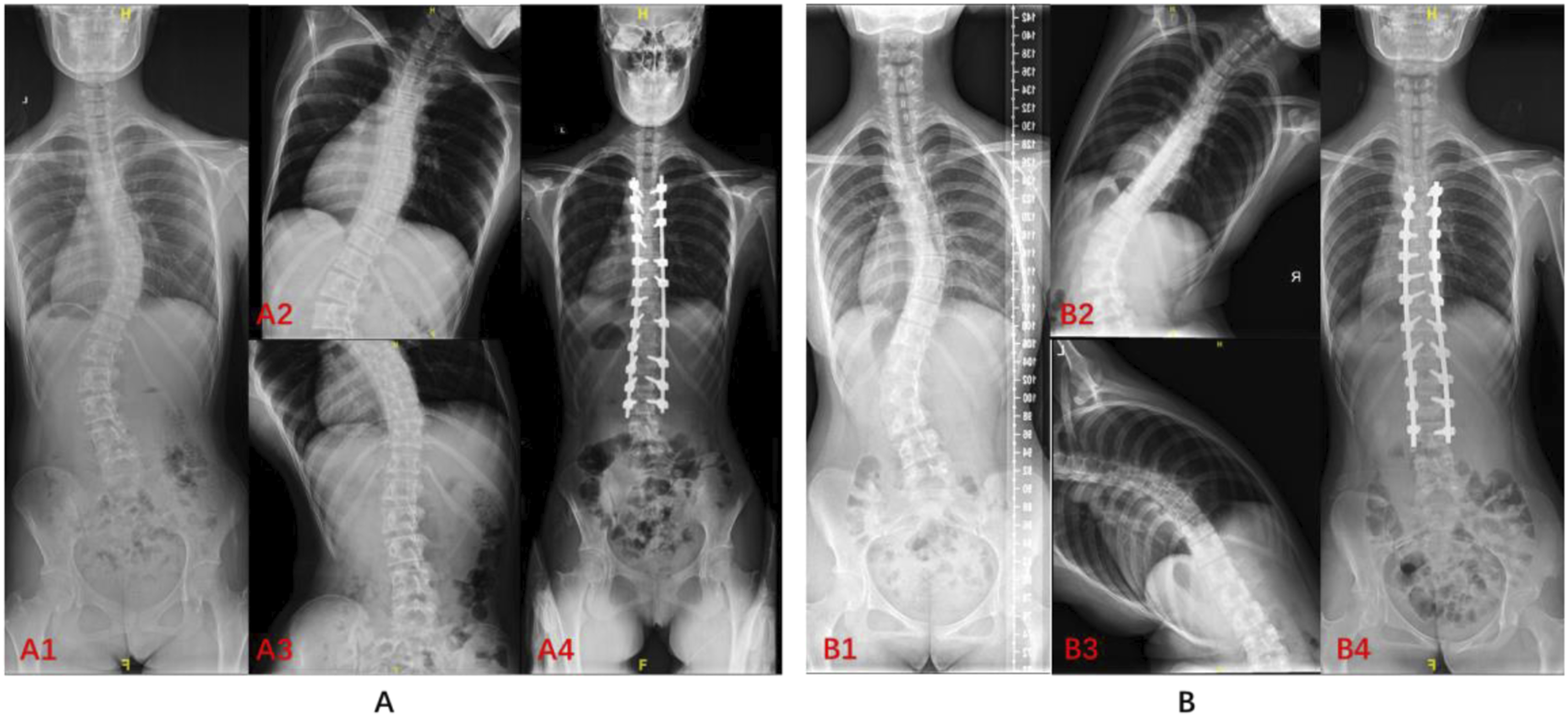
Comparison of peri-operative complications between FJO group and Ponte group.

Discussion
This study proposes a preoperative spinal flexibility threshold (0.657), providing scientific evidence for the selection of osteotomy techniques in patients with IS. The results indicate that when flexibility is below the threshold, PO significantly improves the correction rate. Conversely, when flexibility exceeds the threshold, FJO achieves comparable correction outcomes while offering lower complication risks and faster postoperative recovery. By quantifying the impact of flexibility on surgical decision-making, this study addresses the absence of quantitative guidance in the existing literature.
The role of spinal flexibility in surgical outcomes has been well-documented in the literature. 7 Bridwell’s classification of coronal deformities 8 emphasizes the importance of flexibility in determining the need for osteotomy; However, our study refines this concept by introducing a quantitative threshold, offering more precise guidance for surgical decision-making. This quantitative model complements the Bridwell classification by offering a clear decision-making tool, especially in borderline cases where clinical judgment may vary. Research on utilizing preoperative model construction to optimize surgery has also been emerging continuously. Ruchit V. Patel et al. 9 highlighted the role of advanced imaging techniques in preoperative planning. The integration of our flexibility-based threshold into three-dimensional (3D) modeling and surgical simulation technologies could enhance preoperative planning by allowing surgeons to visualize and predict the outcomes of different osteotomy techniques in patients with varying degrees of flexibility. For example, combining flexibility thresholds with 3D-printed spine models10,11 could facilitate the development of patient-specific surgical strategies, thereby improving accuracy and reducing operative time.
The flexibility threshold identified in this study has significant clinical implications for surgical practice. The threshold value (0.657) provides surgeons with a clear demarcation to tailor surgical strategies for patients with varying degrees of spinal flexibility. For patients with higher flexibility (such as those with adolescent idiopathic scoliosis, AIS), 12 less invasive techniques like FJO can be prioritized, reducing intraoperative blood loss and shortening recovery time while avoiding the risks associated with overtreatment.13,14 Additionally, the flexibility threshold helps identify the minority of cases requiring more complex interventions, such as patients near the threshold, thereby minimizing reliance on subjective, experience-based decision-making.
For patients with lower flexibility (e.g., those with adult scoliosis, AS), greater spinal release is often required, making PO a more suitable option. In cases of more complex or rigid deformities—where flexibility is significantly below the threshold (e.g., <0.4)—conventional PO may fail to achieve sufficient correction. In such scenarios, more extensive bony release techniques, such as Pedicle Subtraction Osteotomy (PSO) 15 or Vertebral Column Resection (VCR), 16 should be considered. Furthermore, preoperative flexibility evaluation and corresponding osteotomy selection allow for the early identification of high-risk patients prone to complications. Low flexibility and high-grade osteotomies are often associated with increased intraoperative blood loss and a higher risk of intraoperative spinal cord injury (ISCI).17,18 By utilizing the flexibility threshold, surgeons can anticipate these risks and implement preventive measures, such as optimizing intraoperative blood management strategies (e.g., the use of tranexamic acid or cell salvage systems)17,19 and employing advanced techniques like intraoperative navigation 20 or robotic assistance to minimize spinal cord stress during correction. In addition, the flexibility threshold enables surgeons to engage in clearer preoperative communication with patients and their families regarding potential risks and surgical strategies. 21 This improves the level of informed consent, enhances patient understanding, and ultimately leads to greater satisfaction with the surgical process. 22
This study has several limitations. First, it was a single-center retrospective study with a relatively small sample size limited to IS patients, which may affect the generalizability of the findings. Second, only two commonly used low-grade osteotomy techniques (FJO and PO) were evaluated; thus, the proposed flexibility threshold may not apply to higher-grade procedures such as PSO or VCR. Third, 3D deformity parameters 23 were not included in the analysis, which may limit the comprehensiveness of deformity assessment in IS patients. Fourth, other potential confounding factors—such as age, bone quality, Cobb angle, gender, and soft tissue stiffness 24 —were not comprehensively analyzed, which could influence the accuracy of the model. Fifth, as a retrospective study, the choice of surgical approach was based on surgeon experience rather than randomization, which may theoretically introduce selection bias. However, baseline characteristics between groups were similar, and multivariate regression was used to control confounders, minimizing the risk of systematic selection bias. Finally, only immediate postoperative correction rates were assessed, with no long-term follow-up data available. This limits the evaluation of the durability and safety of the surgical outcomes.
Future research should recruit larger, multicenter populations and include both low- and high-grade osteotomy techniques to enhance clinical relevance. Comprehensive 3D analyses and systematic consideration of variables are needed to further refine predictive models. Extending follow-up periods will help capture long-term changes in spinal alignment and late complications. Additionally, developing predictive models for other types of scoliosis will broaden the applicability of these findings and support more individualized clinical decision-making. Integrating our models with emerging technologies, such as 3D printing and artificial intelligence, may further expand their clinical utility and impact.
Conclusion
The introduction of a quantified flexibility threshold (0.657) provides a novel framework for optimizing osteotomy selection in patients with IS. By objectively defining the relationship between spinal flexibility and surgical outcomes, this study offers a practical tool for improving preoperative planning and balancing deformity correction with complication risks. The clinical application of this flexibility threshold could lead to more personalized and effective surgical strategies. Future integration with 3D modeling, intraoperative navigation, and artificial intelligence technologies holds promise for further enhancing the precision and impact of this approach.
Footnotes
Acknowledgments
We would like to thank the surgical and nursing teams at our hospital for their outstanding support in patient care and data collection during this study. Special thanks are extended to Dr Qiyi Li and Dr Jinqian Liang for their guidance in surgical planning and methodology. We are also grateful to the patients and their families for their trust and cooperation, which made this study possible.
Author Contributions
Yibing Liu (Author A): Conceptualization, Methodology, Data Collection, Formal Analysis, Drafting of the Manuscript. Zhenzhuo Zhang (Author B): Data Collection, Statistical Analysis, Visualization, Reviewing and Editing of the Manuscript. Guomao Zhu (Author C): Literature Review, Data Validation, Reviewing and Editing of the Manuscript. Jinqian Liang (Author D): Supervision, Project Administration, Reviewing and Final Approval of the Manuscript (Corresponding Author).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National High Level Hospital Clinical Research Funding (Project number: 2022-PUMCH-B-002) and National Natural Science Foundation of China (Project number: 82072477).
Ethical statement
Data Availability Statement
The data that support the findings of this study are derived from the database of our hospital, which contains sensitive patient information. Due to the privacy and confidentiality policies of the institution, the data is not publicly available. However, de-identified data may be made available upon reasonable request to the corresponding author and with approval from the institutional ethics committee.