
Abstract
Study Design
Narrative Review of published literature.
Objective
The objective of this article is to review the current state of treatment for patients with adult spinal deformity (ASD) with a focus on preoperative planning, optimization and intraoperative surgical techniques, including the application of current enabling technologies to spinal deformity surgery.
Methods
A literature review of publications related to preoperative planning, patient optimization, intraoperative techniques, and surgical outcomes for the treatment of ASD was performed.
Results/Conclusion
Standardized preoperative evaluation including imaging analysis now allows patient specific planning for the planned surgical procedure. The current work on patient optimization along with understanding and mitigating the surgical insult are being utilized as appropriate and should improve patient outcomes. The intraoperative application of enabling technologies including navigation, robotics and confirmatory radiographic software will continue to assist surgeons in safe placement of instrumentation, often with less invasive surgical techniques and achievement of intraoperative alignment goals.
Keywords
Introduction
The surgical treatment of adult spine deformity (ASD) patients has steadily evolved over the past 25 years with a focus on lessening complications, optimizing radiographic correction and surgical outcomes. However, complication rates for the most common adverse events such as proximal junctional failure, implant failure and pseudarthrosis and various medical complications still remain stubbornly high.1-4 The goal of this narrative is to utilize current clinical research to provide insight on how the proper use of preoperative planning, patient optimization and intraoperative surgical techniques can all be leveraged to lessen the morbidity and complications while improving short and long term outcomes for these often challenging patients and conditions.
Preoperative Planning
When evaluating a patient for an adult spinal deformity (ASD) it is important to consider several factors including patient complaints, neurological status, medical status, social situation, and thorough radiographic analysis. It is also critical to understand the mechanism of the spinal deformity, what region of the spine the deformity is affected, and to determine if the spinal deformity is a flexible, semi-rigid or rigid. Sagittal, regional, and global alignment has been well documented since the advent of the SRS-Schwab classification criteria for ASD, which was published in 2013.5-7 Upright anterior-posterior (A/P) and lateral x-rays, which include the base of the skull to the femoral heads, will allow for appropriate spinal alignment analysis and global balance analysis.
8
Traditionally, obtaining these measures involved measuring printed radiographs. Following the advent of modern imaging program interface, manual digital measurement of angles and measurements could be performed. Advancements within the field are beginning to provide automated solutions for these measurements in order to deliver consistency both in radiographic measurements and in the variables being evaluated which account for sagittal, spinopelvic parameters and coronal parameters.9-11 These automated software systems provide radiographic parameters that include: pelvic tilt, pelvic incidence, sacral slope, lumbar lordosis, T1 pelvic angle, sagittal vertical axis, and thoracic kyphosis; as well as coronal cobb angles, apex level, distance from apex to central sacral vertical line and distance to C7 plumb line for 3 regions that include T1-T4, T5-T10, and T11-L4. Figure 1 demonstrates a patient with an iatrogenic ASD demonstrating lateral and A/P radiographs with associated automated radiographic measurements. Patient with an iatrogenic ASD demonstrating lateral and A/P radiographs with associated automated radiographic measurements. Patient is a 29-year-old man with history of Scheuermann’s kyphosis who had a distal junctional failure and developed a 92° kyphosis centered at L2. (A) Lateral standing radiograph. (B) Spinopelvic parameters that are automatically generated from radiograph shown in (A). (C) A/P standing radiograph. (D) Coronal parameters that are automatically generated from radiograph shown in (C).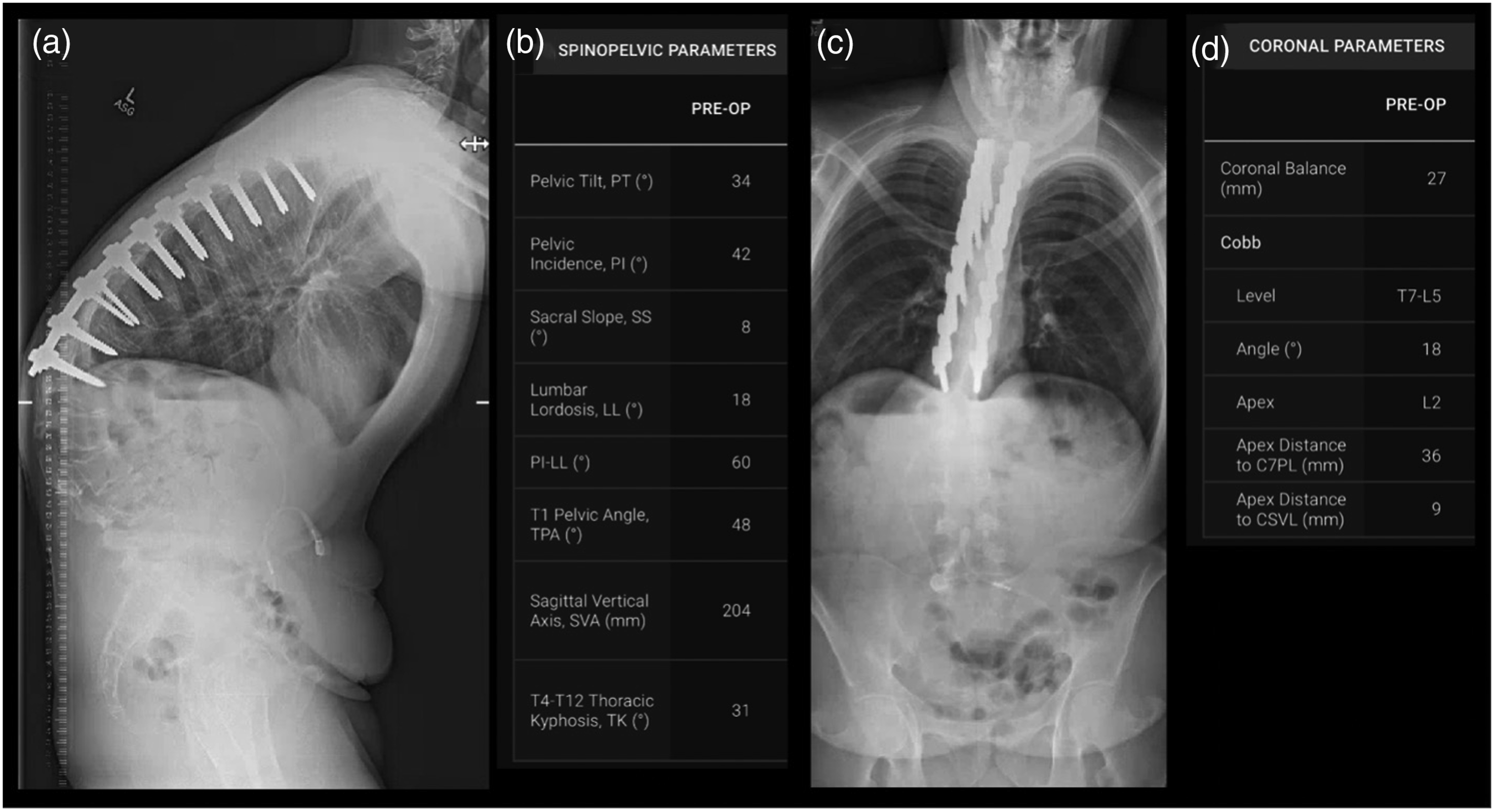
Understanding the underlying flexibility of the spine can be better identified by evaluating a patient utilizing x-rays in the upright, supine, flexion-extension, and bending positions. The advantage of an X-ray is the capability to obtain a full-length view of the entire spinal column in these various positions.12,13 Although x-rays do provide an opportunity for evaluation of spinal column change between these positions, there are other imaging modalities which can provide similar insights, such as computed tomography (CT) scans.
14
It is well known and understood that a vacuum disk phenomena implies motion through a disk space, and is best visualized with CT scans.
15
In contrast to a mobile segment inferred through a vacuum disc, a CT scan can also be utilized when evaluating for fusion. Using CT for evaluating the flexibility of the spine in the setting of a prior fusion, is the gold standard for evaluating fusion at a given level. Figure 2 demonstrates 2 patient examples which show (Figure 2A) vacuum discs, and dorsal fusion mass and fused disc spaces in the setting of a prior fusion (Figure 2B). Combining the upright, supine, and flexibility x-rays together with the CT scan, allows a surgeon who is evaluating the spinal flexibility/rigidity to gain insight and determine whether a deformity is flexible, rigid, or semi-rigid. Making this ultimate designation upon the kind of spinal deformity that is being encountered is imperative for preoperative planning of surgical techniques required to achieve the appropriate correction at the time of surgery. Patients examples including representative slices highlighting vacuum discs and robust fusion. (A) Midsagittal CT scan slice demonstrating vacuum disc within the 6 disc spaces spanning thoracic 12 to sacral 1 vertebra. (B) Para-sagittal CT scan slice demonstrating robust fusion through disc spaces (L4/5) as well and posteriorly (L2-S1), highlighted with arrows.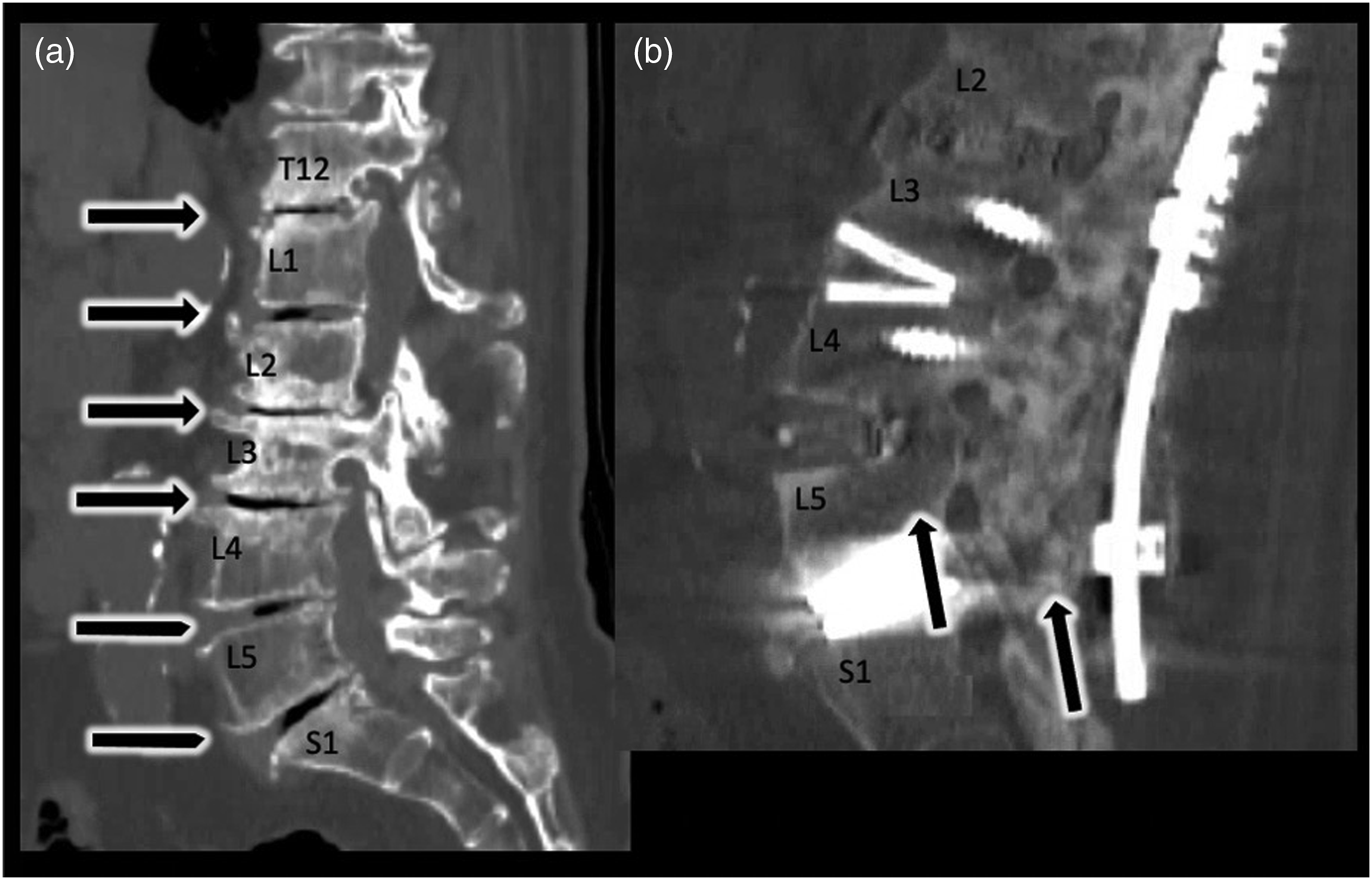
An MRI provides a critical and necessary evaluation of the underlying neural elements. 14 It is crucial to understand the relationship of neuroradiographic stenosis to an existing neurological deficit or radiculopathy prior to surgery so that it may be addressed at the time of surgery. At minimum, the total area incorporated within a spinal deformity reconstruction should be imaged with an MRI prior to surgery. Depending on the extent of surgery, it may be valuable to obtain a complete spinal axis MRI if the duration and invasiveness of the procedure is maximal. An example may include an upper thoracic to pelvis fusion, where it may be beneficial in this setting to also obtain a cervical MRI if the patient's age and/or demographics are suggestive of potential underlying cervical degeneration and/or stenosis, as there is a relatively high association of cervical degeneration and stenosis in patients presenting with a symptomatic thoracolumbar deformity. 16
Within the context of prior instrumentation, the degree of implant artifact created within the MRI field surrounding spinal instrumentation may compromise the ability to adequately evaluate neural elements at a region that may be in question. In these settings it may be valuable to obtain a CT myelogram in order to better understand either the area(s) within the previously instrumented region, or the area(s) immediately adjacent to the region such as the adjacent level disease. 17
A specific advantage of obtaining a full-length supine X-ray for the ASD patient is that the surgeon is provided insight into the difference and spinal alignment change between the standing/upright and supine radiographs. Shown in Figure 3 are 2 examples of patients who have both standing and supine x-rays for comparison. Figures 3A and 3B demonstrate an example of a flexible ASD, which is highlighted by the change from standing to supine. Figures 3C and 3D demonstrate an example of a semi-rigid ASD, which is highlighted by the minimal change shown from standing to supine. Utilizing x-rays can be the single modality that can provide the greatest amount of objective information when making the determinations whether a spinal deformity is flexible, semi-rigid, or rigid.
18
Aside from determining the underlying spinal deformity flexibility, the supine X-ray also provides a proxy to what will be encountered during surgery when the patient is prone on the operating room table.
19
Patient examples demonstrating the use of standing and supine x-rays in order to understand the flexibility of a spinal deformity. Patient shown in (A, B) has sagittal vertical axis of 12 cm when measured on the standing lateral radiograph. Figure (A) is demonstrating a standing lateral radiograph, and (B) is the same patient with lateral supine radiograph (non-weight bearing). Comparison of (A) and (B) demonstrates a flexible spinal curvature that corrects simply when changing positions from standing to supine. Patient shown in (C, D) has a semi-rigid spinal deformity. Figure (C) is demonstrating a standing lateral radiograph with a focal kyphosis of 67° centered at T12, and (D) is the same patient with lateral supine radiograph (non-weight bearing) demonstrating a focal kyphosis of 51° centered at T12. Comparison of (C) and (D) demonstrates a semi-rigid spinal curvature at T12, which flexible enough to reduce by 16° making it non-rigid, but not flexible enough to reduce completely, therefore making it a semi-rigid spinal deformity.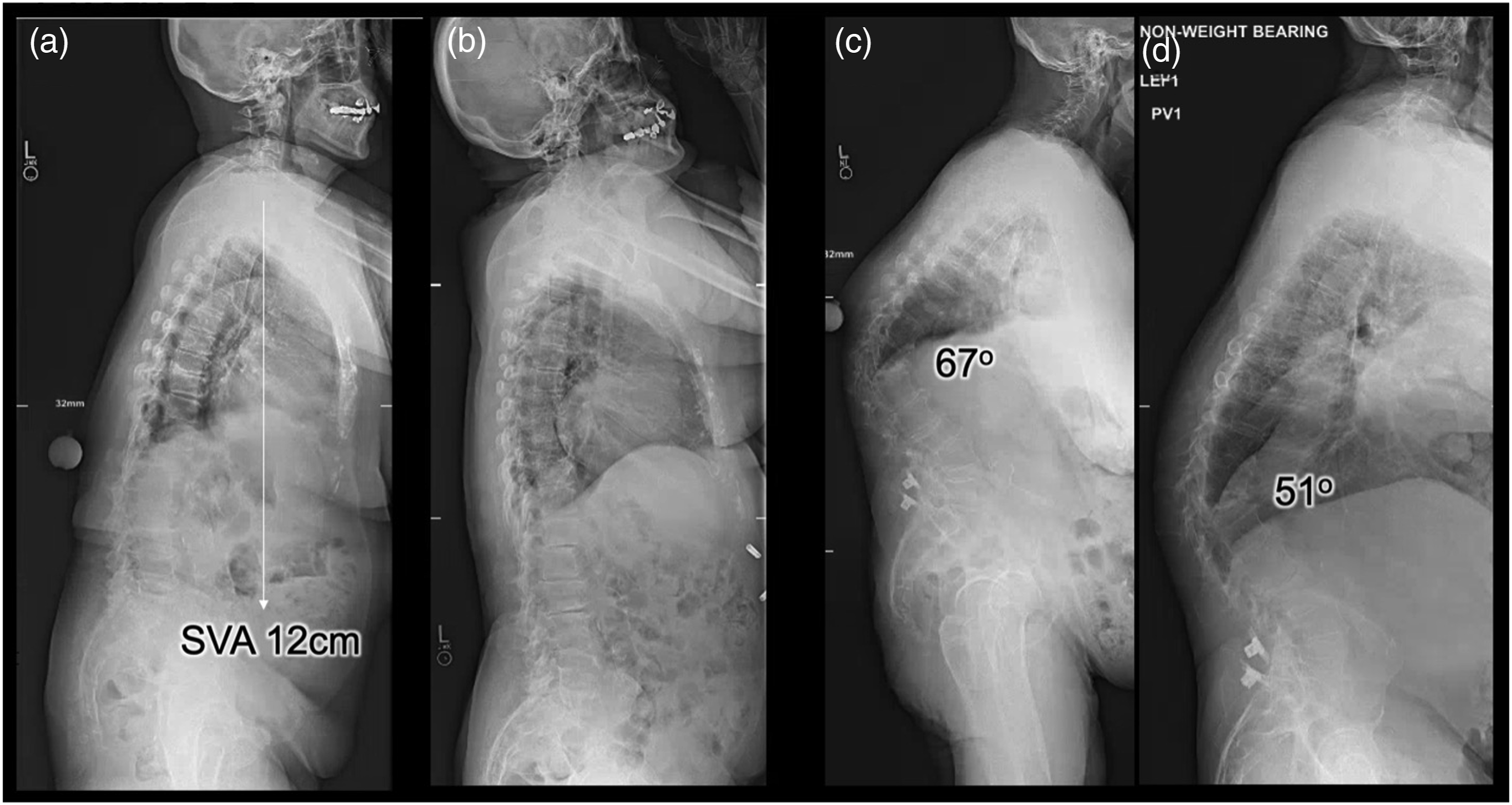
If the surgeon is seeking further affirmation as to the degree of change that can be obtained or the evaluation of a specific region with regards to mobility, x-rays can be acquired with the patient bending to both the left and right sides, in flexion and extension, using traction, or a fulcrum bend. Figure 4 demonstrates an adult idiopathic scoliosis patient who has an adult thoracolumbar scoliosis, where the upright and supine films are utilized to evaluate last touched vertebrae. Figure 4 also demonstrates bending films which could be further used to understand the regional correction and local change at the expected lower instrumented vertebra level. Traction x-rays are often those obtained when a patient is undergoing sequential halo-gravity traction leading up to an ASD correction.
20
Patient example for an adult idiopathic scoliosis demonstrating the use of standing, supine, and bending x-rays. Figure (A) is demonstrating a standing lateral radiograph with main thoracic scoliosis of 36° and thoracolumbar scoliosis of 56°. Figure (B) is the same patient with lateral supine radiograph (non-weight bearing). Comparison of (A) and (B) demonstrates a flexible spinal curvature that corrects the scoliosis of the main thoracic region and the thoracolumbar region. Figure (C, D) are standing bending radiographs. Figure (C) the patient is bending to the right and Figure (D) the patient is bending to the left.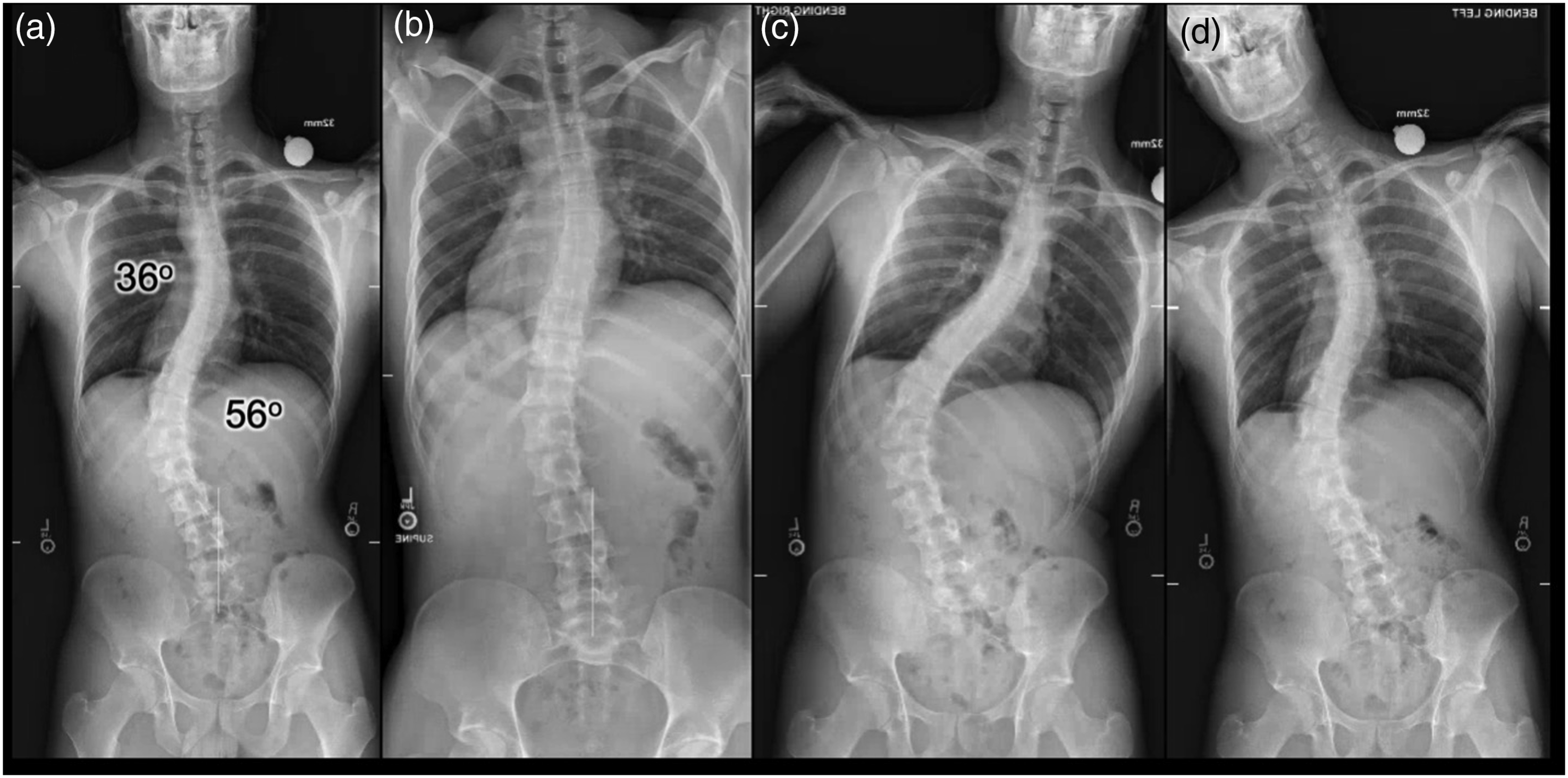
Software Measurement Tools
As was described in a prior section on radiographic spinopelvic parameters, there are software measurement tools that deliver an automated approach at measurements including global alignment, spinopelvic alignment, and scoliosis measurements. These same parameters are calculated in the preoperative radiographic measurement stage and are useful in determining the underlying etiology which is driving the ASD. Additionally, simulating various correction scenarios is a powerful technique and that can be utilized in modern software which incorporate predictive analytics.21,22 When considering more than one plan, and deciding between a variety of levels of fusion, various osteotomy techniques, and reciprocal changes within the non-instrumented regions, the plan simulation tools provide an opportunity for the surgeon to visually identify a target goal for radiographic realignment and the associated radiographic measurements that correspond to the planned correction. When using modern techniques, such as predictive analytics and software measurement tools, the surgeon can better delineate the difference for a desired outcome. Having a tool that provides a predictive outcome for a variety of invasiveness procedures allows the surgeon to carefully balance and risk stratify patients. The surgeon can then tailor the appropriate treatment for the desired outcome. The patient described in this example is a patient who is of advanced age, 85 years old, has a significant amount of disability but had a normal frailty index. A simulation in this scenario provides the opportunity to identify the least amount of surgery that is required in order to achieve a desired outcome.
There is an added value in understanding what the compensatory changes will be for the non-instrumented vertebral segments. The reciprocal thoracic kyphosis, or anticipated proximal change, is often simulated in these predictive analytic tools. The degree of mobility through the non-instrumented regions, proximal segments, and whether or not the compensatory changes can be realized, is a factor that is not fully incorporated into predictive analytic tools. The same tools utilized for preoperative radiographic measurements and preoperative planning are the tools that are used for post-operative assessment of realignment. Software that is used preoperatively allows the surgeon an analytic-based assessment of their correction. Surgeons have the ability to look at their global realignment, and spinopelvic realignment over a series of cases.
The predictive model is an iterative model which utilizes a data set of known preoperative, and postoperative standing x-rays, and attempts to predict a proximal compensatory change directly intended to correlate with proximal junctional failure. The goal of these predictive models is to predict and therefore avoid proximal junctional failures. The methodology for reducing these failures involves placing the appropriate amount of correction within the spinal segments being utilized for the correction in order to recreate the appropriate global and spinopelvic realignment. Currently, there is a singular platform that provides a predictive analytic tool resulting in a patient-specific implant, which is a rod that ultimately will yield a desired outcome for a specific plan. 23 As the model further understands the surgeon’s capabilities by analyzing prior results from surgeon-specific data, it is better able to provide accurate surgeon-specific predictions. Short and long-term results of this type of new technology will be important to critically review to assess the perceived benefits promoted.
ASD Classfication Schemes
Several classification systems have been developed to standardize the description of adult spinal deformities and guide treatment decisions. Among these, the Aebi, Scoliosis Research Society (SRS)-Schwab, Roussouly, and Lenke classification systems are prominent and widely referenced. The Aebi classification was one of the first comprehensive attempts to categorize spinal deformities in adults. It primarily focused on the etiology of the deformity and divided cases into 3 broad categories: Type I, degenerative; Type II, idiopathic; and Type III, deformities secondary to metabolic or other underlying diseases. This classification system emphasized the importance of understanding the underlying nature of the deformity, specifically in adult patients whose deformities may have progressed from earlier life stages or developed as a result of aging and degenerative changes.
The SRS-Schwab classification system, originally published in 2006 and revised in 2012, sought to communicate more specific characteristics of an individual’s deformity rather than the etiology.
5
The SRS-Schwab system consists of coronal curve types and 3 sagittal modifiers (Figure 5). The coronal curve types are identified as thoracic, thoracolumbar/lumbar, double major, and no major coronal deformity depending on the region and magnitude of the curve. Sagittal modifiers in the Schwab system include the pelvic incidence minus lumbar lordosis mismatch (PI-LL), SVA, and pelvic tilt (PT). The implications for treatment planning are profound, as the Schwab classification guides the surgical approach by highlighting which patients may benefit from sagittal plane correction. For example, patients with significant PI-LL mismatch may require posterior column osteotomies or other techniques to restore lumbar lordosis, while patients with severe SVA displacement may need more aggressive sagittal alignment restoration strategies. The SRS-Schwab system was the first to help develop a surgical plan tailored to the individual’s deformity, with a strong emphasis on achieving proper sagittal spinal alignment. The SRS-Schwab classification of ASD consists of curve type and 3 sagittal modifiers.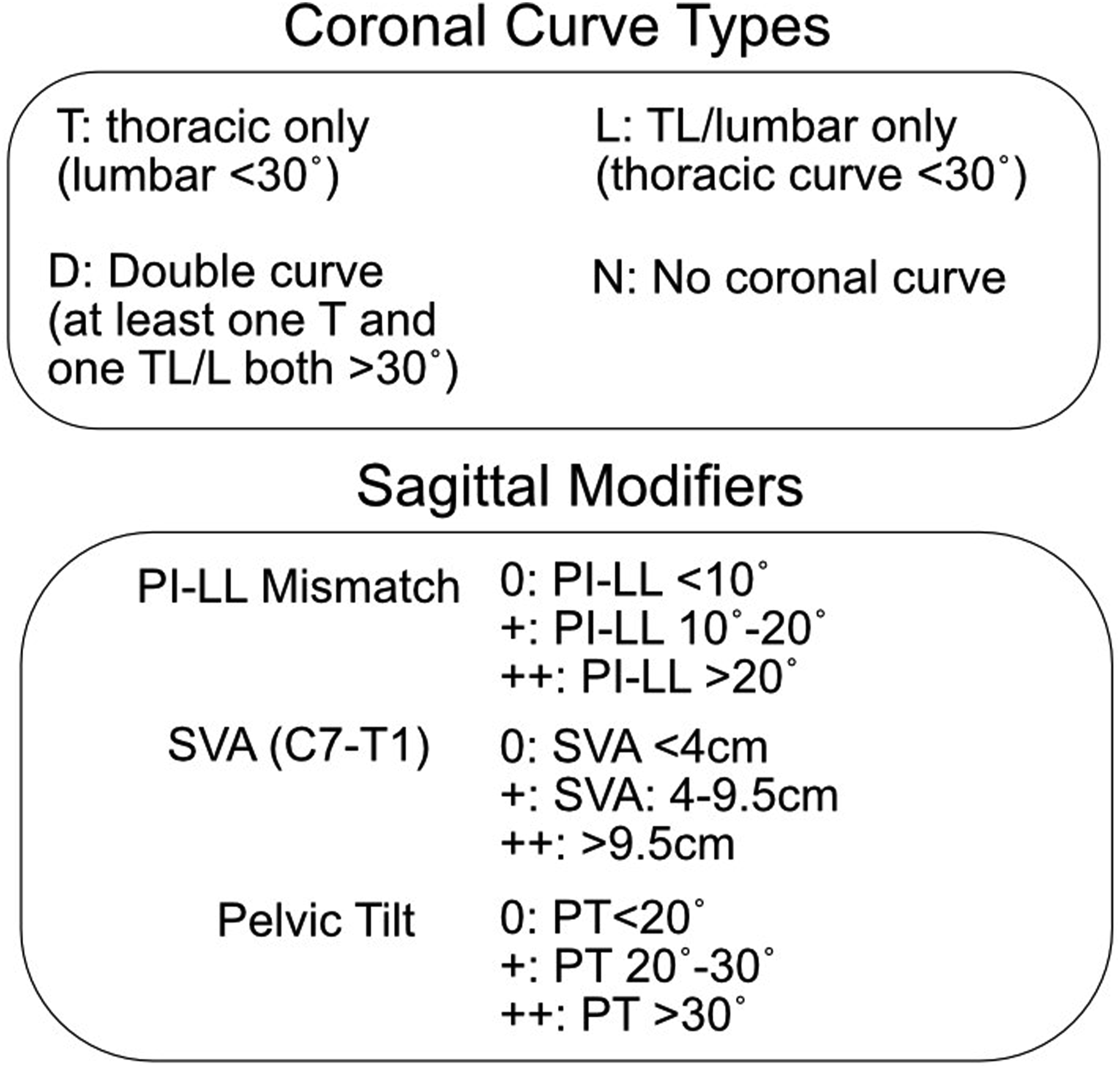
Roussouly also understood the importance of sagittal alignment and characterized 4 patterns of variation of normative sagittal alignment based on the pelvic incidence and location of the inflection point where thoracic kyphosis transitions to lumbar lordosis (Figure 6).
24
In Type 1 curves, the pelvic incidence is low and the inflection point occurs at the L3/L4 level. This results in a long kyphotic curve and short lordotic curve proportioned in an 80:20 split. In Type 2 curves, the pelvic incidence remains small and the inflection point occurs more cranially at the L1/L2 level. Here the kyphotic curve becomes shorter and the lordotic curve becomes longer proportioned in a 60:40 split. Type 3 curves have a higher pelvic incidence and an inflection point at the T12/L1 level. The length of the kyphotic and lumbar curves is almost equal, i.e., 50:50 split. Finally, Type 4 curves have the highest pelvic incidence, most cranial inflection point occurring at the T9-10 level and a reversed split of the length of the kyphotic and lumbar curves at 20:80. Although this classification system categorizes alignment with discrete types, it is helpful to think of this classification as a continuum where the pelvic incidence and location of the inflection point are closely related to the corresponding kyphotic and lordotic curves. Schematic depicting the different curve types identified in the Roussouly classification.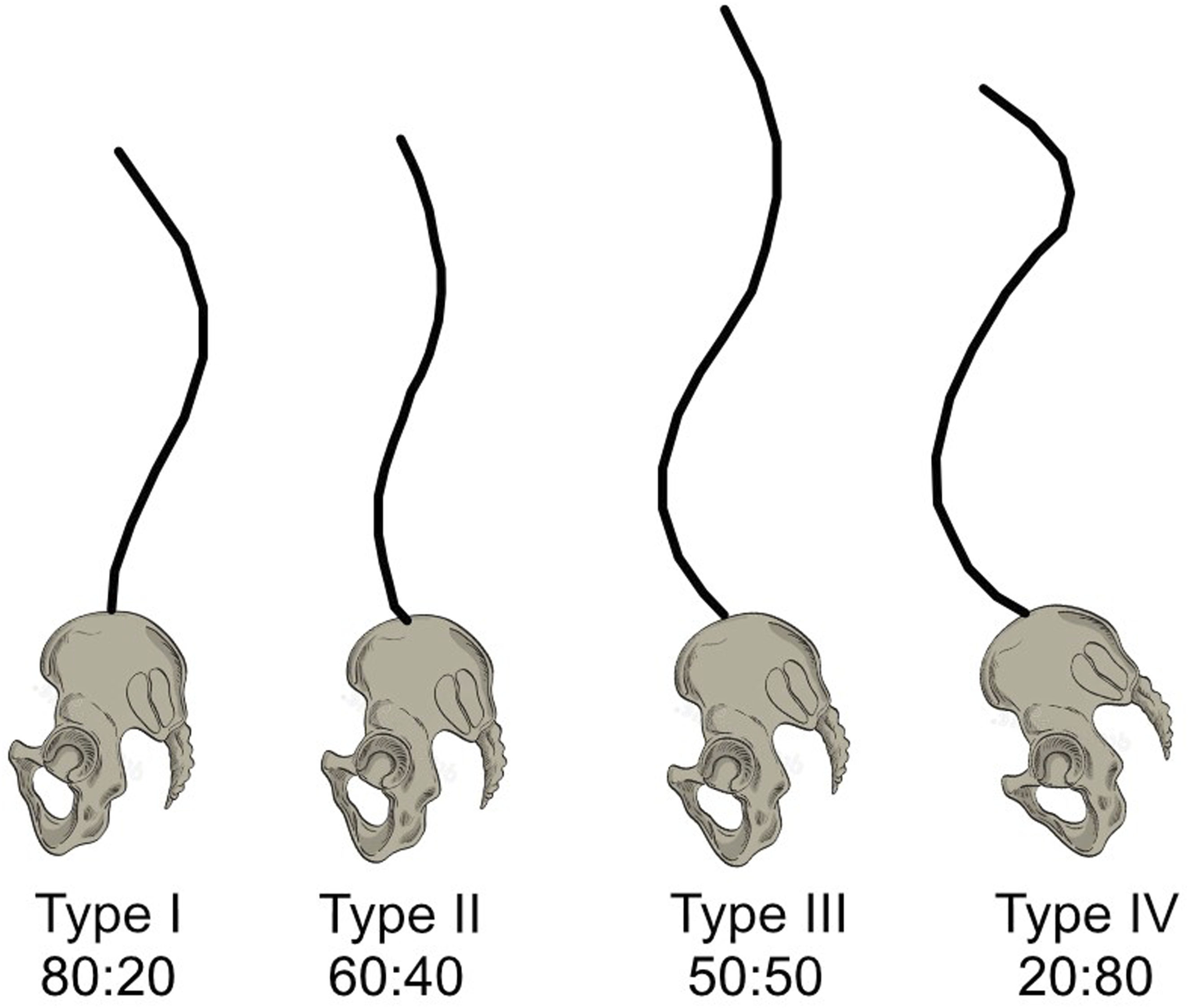
The widespread acceptance and utility of the Lenke classification for AIS led to the development of an Adult Idiopathic Scoliosis (AdIS) Lenke classification system tailored for ASD.
25
This relatively new radiographic classification categorizes AdIS based on 3 main criteria: curve type, lumbosacral curve morphology, and global spinal alignment. Similar to the AIS classification, curve types are defined by the location and magnitude of the deformity, identifying 6 primary curve types: • • • • • •
Assessment of the lumbosacral curve is also included in this classification scheme with the use of a modifier. A structural lumbosacral curve is defined as a lumbosacral curve measuring greater than 20° on a supine coronal radiograph. The Cobb angle of the lumbosacral curve is determined using the angle between the superior endplate of L4 and the superior endplate of S1. Curves are described using the modifier as either structural (S) or nonstructural (NS). Finally, the SVA and CVA are used to assess sagittal and coronal alignment, respectively. A SVA greater than 40 mm indicates sagittal malalignment while a CVA greater than 40 mm indicates coronal malalignment. Patients are assigned a modifier of either aligned, sagittal malalignment, coronal malalignment, or combined malalignment (Figure 7).
25
Table depicting the Adult Idiopathic Scoliosis (AdIS) Lenke classification system.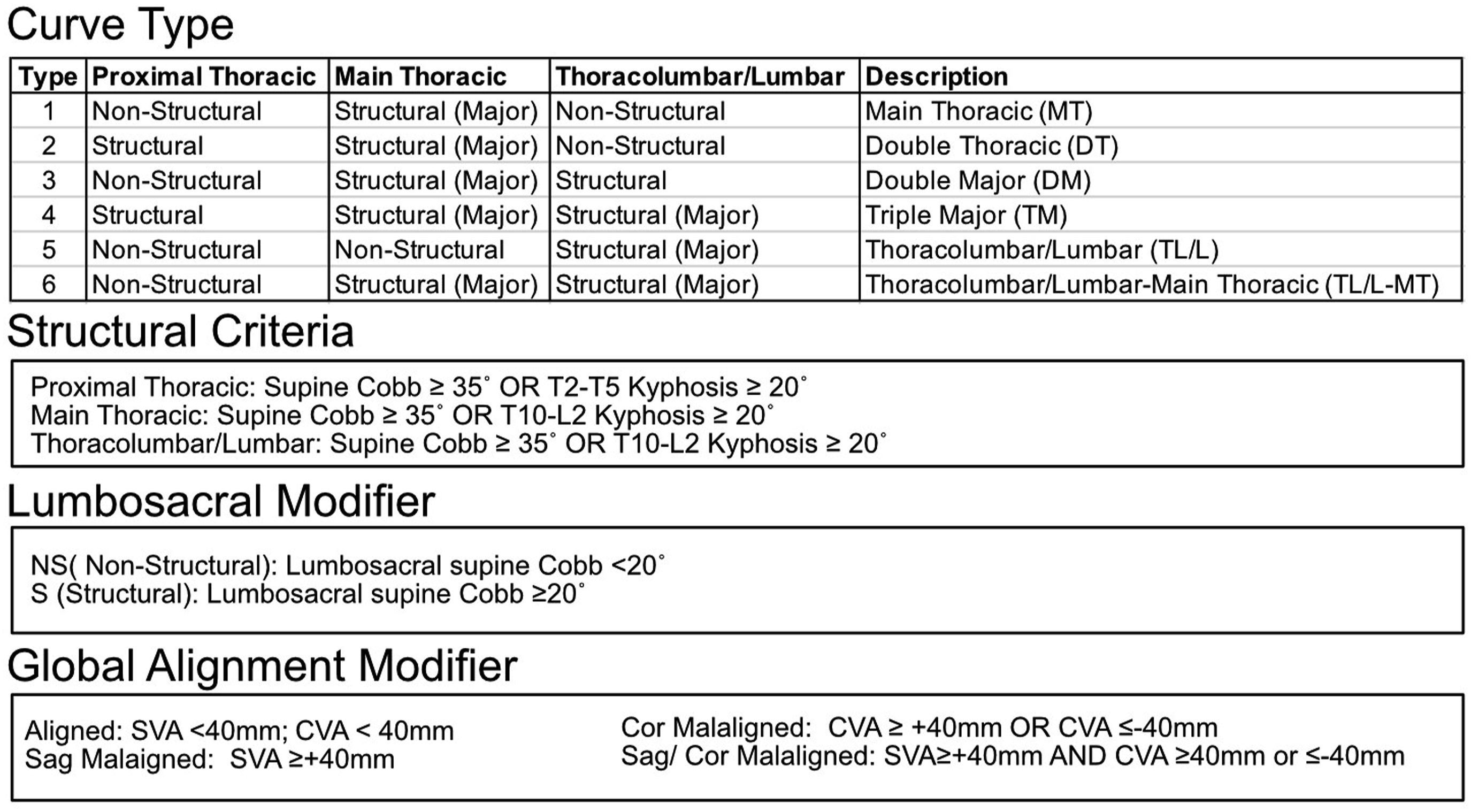
All of these ASD classification schemes provide insight into various radiographic and alignment patterns that allow for appropriate communication and various treatment implications. Obviously, there are still many factors that lead into proper planning and ultimate intraoperative technical execution, but one would argue that the more prepared a surgeon is for the type of ASD being treated, the more specific and successful plan can be created with a greater chance of success and optimal outcome. However, this thought process has not yet been proven in a large clinical trial(s) and more work is needed in this area to confirm the benefit of patient classification with an eye towards surgical treatment.
Patient Risk Stratification
There has been a big emphasis on optimizing ASD patient health status prior to surgery as a logical means of limiting complications and ultimately improving outcomes.26-30 The use of fragility measures and assessments have become standard for many ASD centers with the goal of moving patients into a more favorable fragility level preoperative which has been shown to lower complications, especially for those in the most frail category.31-33 We have instituted a thorough fitness evaluation on nearly all of our ASD preoperative patients in order to objectify their preoperative fitness status and potentially improve upon their condition prior to surgery.27,34,35 Logically, patients who are less frail and with better fitness levels should be able to tolerate an extensive ASD surgery more reliably than those frailer and with lower fitness levels.36,37 Bone health optimization is another critical piece of patient preparedness for surgery, and this topic has already been dealt with in much detail in another manuscript.38,39 The theory that patient preoperative optimization will result in more favorable outcomes still awaits relevant clinical research confirmation.
Certainly one way of objectifying the type of surgical procedure being performed is by a surgical invasive score. 40 The goal of this score was to quantify the amount of surgery being planned and actually being performed on a patient in order to help better risk stratify the patient and the procedure which are obviously linked intimately together. Ideally, taking a healthy patient with a lower invasive surgery should encounter far less complications and lead to a more reliable and successful outcome than with an unhealthy patient undergoing a much more invasive surgery. Ideally, with large data sets and machine learning techniques, it should be possible to preoperatively match the desired patient to an optimal surgical technique that both provides for the necessary surgical correction and radiographic alignment while limiting perioperative adverse events leading to an optimal outcome. This theory also still awaits relevant clinical research confirmation.
Lastly, there are other patient specific factors that recently have been brought to the surgeon community's attention, such as various biologic parameters that may play key roles in patient complications and outcomes. Although frailty has been a prominent feature of patient attribution and evaluation, certain biologic factors, such as ttelomere length, have also been shown to highly correlate with surgical outcomes. In a novel study, Safaee et al have documented that patients with shortened telomere length had greater complications following ASD surgery, which was somewhat irrespective of their chronologic age. 41 These type of biological markers may end up playing a pivotal role in assessing patients overall health status and ability to successfully undergo extensive ASD surgical procedures and is an exciting area of future research in this field.
Surgical Decision Algorithms
In many areas of medicine, treatment variability has been lowered in order to ultimately improve care at the point of contact. One example is the rapid adoption of acute stroke treatment algorithms that have populated nearly all emergency rooms and in-patient hospital settings in the United States. Ideally, this type of consistent treatment paradigms would appear to benefit ASD surgical treatment where the variability is quite high both in the patient presentation as well as the surgical treatment rendered. Certainly, the commonsense goal of performing the least invasive and morbid surgical procedure to solve the patients clinical problem is a logical initial step. However, things are much more heterogeneous and complex in ASD patients, who often have a combination of neurologic, radiographic, instability and alignment issues all packaged into their presentation. Thus, solving the main issue of lumbar stenosis producing neurogenic claudication via a multilevel decompression may seem appropriate, but when the segments being decompressed have marked deformity, instability such as rotatory subluxations and foraminal narrowing from intersegmental collapse, decompression alone may not suffice or provide only short term benefit. Thus, each ASD patient really needs a more universal assessment to provide an individual treatment plan for the amount of heterogeneity involved in their condition. This is why a “typical” 45° degenerative lumbar scoliosis can produce surgical treatment options ranging from micro-decompression all the way to a lower (or even upper) thoracic to sacrum and pelvis spinal reconstruction and every possible intervention in between. Thus, to be able to produce evidenced- based treatment algorithms for ASD patients is currently beyond the scope and capability of this review, but this field is ripe for joining the power of large data (and databases) to the rapidly growing field of machine learning and AI to help bridge these individual treatment gaps and assist in a more structured, less variable portfolio of surgical procedures, based on the surgeons ultimate areas of technical expertise, to render a more consistent operative procedure producing reliable and consistent treatment outcomes.
Intraoperative Considerations
Positioning
Appropriate patient positioning in spine surgery is vital to a successful and safe procedure. Positioning serves to allow adequate exposure to the surgical site, assist in passive spinal column correction, and minimize risk of associated pressure-related injuries to the patient. While spinal deformity surgery can be performed in various patient positions, e.g., lateral or supine, the most commonly employed is the prone position.
42
Historical descriptions of the prone position include the “tuck, knee-chest, and praying position”, however, these are associated with high rates of complications such as vascular and peripheral nerve injury, as well as muscle necrosis leading to acute kidney injury.43,44 The development of modern frames has significantly reduced such complications with an aim to pad bony prominences, maintain physiologic positioning of the limbs, and reduce intra-abdominal and intra-ocular pressure.
45
Additionally, frames play a vital role in inducing lordosis or kyphosis on the native spine, depending on the goals of surgery. With an emerging awareness of the importance of restoring sagittal alignment in spinal deformity surgery, frames that induce lordosis are becoming increasingly utilized. Tan et al reported on the changes in preoperative standing alignment vs intra-operative alignment following positioning on chest rolls, the Andrews frame, the Hastings frame, and a four-poster spinal frame.
46
They found a 50% reduction in overall lumbar lordosis when using the Hasting, Andrews, and four-poster frames. The OSI Jackson surgical table, introduced in 1992, is a dual column design which allows for the abdomen to be unrestricted, 360 degrees of rotation, and complete radiolucency. It has gained in popularity for use in deformity surgery in which lordosis needs to be generated. Peterson et al showed superiority of the OSI Jackson frame in maintaining or increasing lordosis vs the Hastings frame.
47
Likewise, Marsicano et al showed an increase of thoracolumbar and lumbar lordosis for patients with AIS undergoing a deformity correction when using an OSI frame.
48
In addition to frame designs, the positioning of the legs can also influence lordosis and kyphosis on the spine. For example, placing the legs in a sling allows for relative hip flexion which in turn will facilitate decreasing lumbar lordosis. Conversely, placing the legs on flat boards with pillows will extend the hips, inducing lumbar lordosis (Figure 8). This is an intra-operative patient example demonstrating prone pads positioning which is optimized for the apex of the spinal deformity. The cranial pads are pushed his for cranial as possible, and the anterior superior iliac spine pads are pushed caudally. Shown in the red arrow is the apex of the deformity and the pad positioning shown by the black arrows in both images.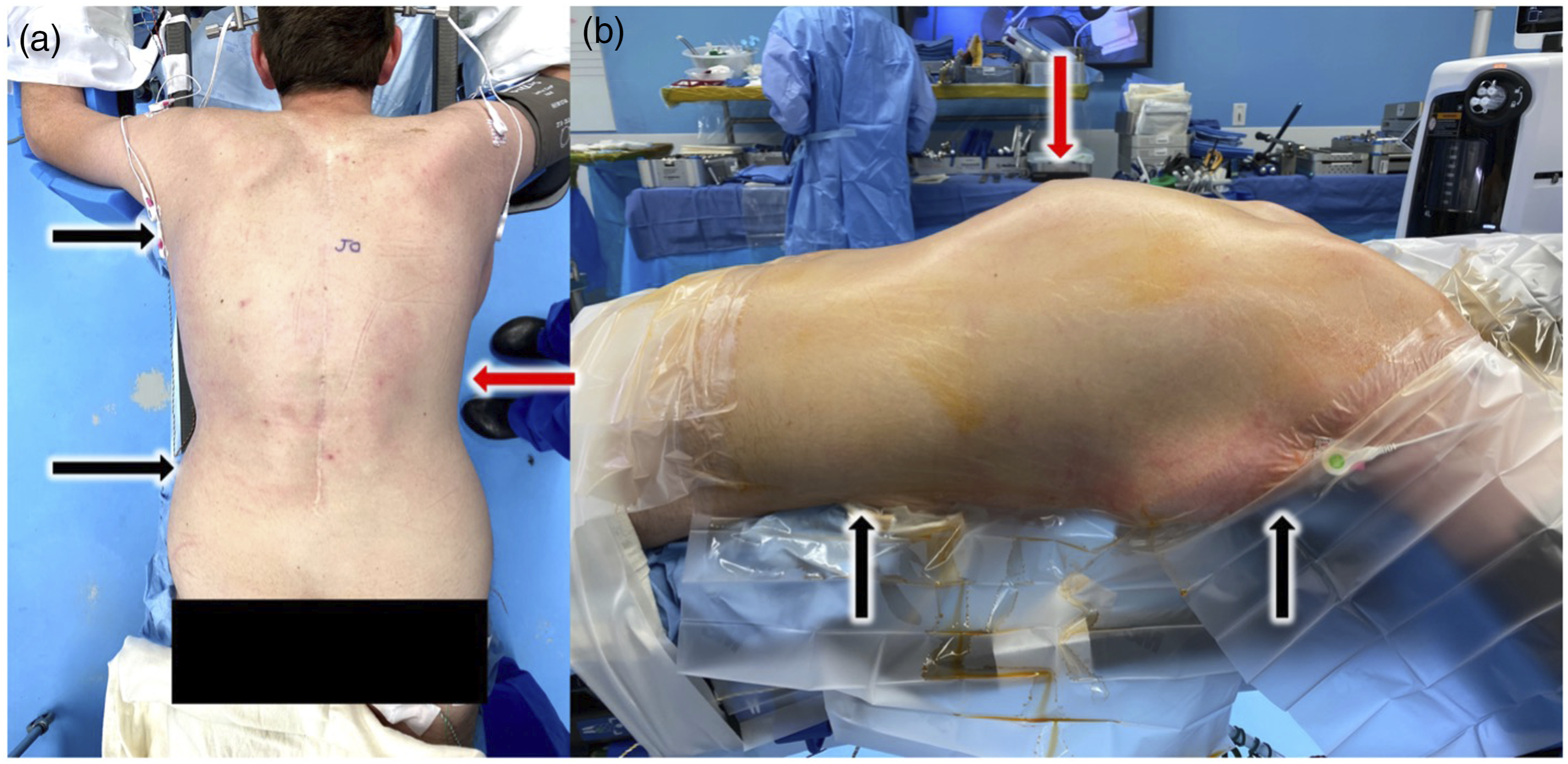
Despite advances in positioning techniques and operative table design, improper patient positioning during spine surgery continues to pose a risk for injury to the patient. This is due to the supra-physiologic stresses that are placed on patients while in the prone position. 49 Although rare, the most reported complications associated with the prone position include post-operative vision loss (POVL) and perioperative peripheral nerve injury (PPNI). 49 Post-operative vision loss is a rare yet potentially devastating complication following spine surgery with a reported occurrence of 0.03%50-52 POVL has been reported as a result of ischemic optic neuropathy, central artery occlusion, ischemic orbital compartment syndrome, or occipital cerebral infarction. 53 The proposed pathogenesis is an increased orbital venous and intraocular pressure secondary to applied external pressure during surgery. Risk factors include prolonged operative time, intraoperative anemia, hypotension, and high-volume infusions. Other risk factors include a Trendelenburg position, rotation of the head, and applied ventral pressure as they may compromise blood flow to the optic nerve.54,55 At our institution, it is routine to utilize a skull clamp, such as a Gardner-Wells tongs, halo or Mayfield, for patients undergoing long-segment spinal deformity surgery. While these instruments pose unique but rare complications of their own, including laceration of the superior temporal artery, fracture of the inner table, and infection, they have the distinct advantage over horseshoe and foam headrests in that they do not apply any external pressure to the orbit.56-59 Additionally, they allow for unobstructed visualization of the face, controlled positioning of the cervical spine, and more readily facilitate surgical exposure of the spine in instances where a cervicothoracic fusion is indicated. Proper lower extremity positioning, especially in those patients with significant fixed sagittal malalignment is essential and warrants continued intraoperative monitoring as patients can sustain various lower extremity nerve compressions, such as quadriceps palsy, while positioned prone even with appropriate padding, which can be relieved with appropriate recognition and interventions. 60
Appropriate positioning of the upper extremities while in the prone position is critical to prevent injury to the brachial plexus or peripheral nerves, especially during prolonged operative periods. These typically present in the form of neuropraxia or axonotmesis. 61 The brachial plexus is fixed at the cervical and axillary fascia, traversing various bony architecture including the clavicle, first rib, and humeral head making it highly susceptible to stretch injuries. 62 Uribe et al reported on 17 patients who experienced brachial plexus injuries following surgery in the prone position. 62 The single greatest risk factor was abduction of the arm greater than 90°. Other risks included extension, external rotation plus abduction of the arm, rotation plus lateral flexion of the neck in the ipsilateral direction, and lastly application of shoulder braces. The most common clinical presentation of brachial plexus injury is a motor deficit with the majority of cases resolving over time.63,64 Peripheral neuropathies have also been reported secondary to improper positioning. The ulnar nerve is at risk of injury with elbow flexion greater than 90°, direct pressure to the cubital tunnel, or mal-positioning of a blood pressure cuff. 65 Chung et al demonstrated that the ulnar nerve is the most vulnerable peripheral nerve in the upper extremity to brachial artery ischemia. They also identified obesity and preoperative cubital tunnel syndrome as risk factors for ulnar nerve injury following prone positioning. Lateral femoral cutaneous neuropathy, also known as meralgia paresthetica, has been reported in up to 24% of patients undergoing prone spinal surgery. 66 This is thought to be due to direct compression of the nerve by the pelvic bolsters near the anterior superior iliac spine.
Instrumentation
Standard 2 Rod vs Multi-Rod Constructs
Two rod constructs have been the standard of care for spinal deformity surgery since the advent of segmental spinal instrumentation systems, such as the Cotrel-Dubousset (CD) system in the 1980s. However, with the increased use of 3 column osteotomies with increased spinal destabilization occurring intraoperatively, high rates of rod failure have occurred. Hyun showed a statistically lower rate of implant failure and need for revision surgery in 3-column osteotomy (3CO) surgery treated with multi-rod constructs (MRC’s) vs standard 2 rod constructs in a single surgeon consecutive series. 67 The use of triple or “quad” rod techniques and associated placement of 3 to 4 iliac screws has gained in popularity over the last decade even for non 3CO constructs. The first description of a “four-rod” technique by Shen et al has been proven to be biomechanically superior to traditional 2 rod constructs. 68 However, this technique is technically challenging as it requires pedicle screw placement at different angles throughout the construct. Merril et al showed that the use of multi-rod constructs significantly reduces the risk of rod breakage. 69 Long-term studies are required to determine the ideal rod configuration and to assess whether supplemental rods influence fusion rates in these constructs, but most surgeons utilize MRC’s when performing 3CO’s in the thoracic or lumbar spine in ASD patients.
Osteotomies in ASD Surgery
When addressing complex pathology in adult spinal deformity, surgeons may need to utilize osteotomies in order to achieve appropriate correction. The use of osteotomies has become increasingly common as segmental pedicle screw fixation has afforded surgeons the ability to do posterior only surgical corrections. While posterior only surgery spares patients the significant morbidity of an anterior approach, it requires surgeons to be familiar with various osteotomy options in order to achieve similar results to anterior-posterior surgery. This is particularly true when treating patients with acute kyphotic deformities. Three classic osteotomies utilized include the posterior column osteotomy (PCO), the pedicle subtraction osteotomy (PSO), and the vertebral column resection (VCR)
Posterior Column Osteotomy
The emergence of the term posterior column osteotomy (PCO) was an attempt to simplify the often-confusing nomenclature surrounding Smith-Petersen Osteotomy 70 and Ponte 71 osteotomies. Despite different surgical techniques, the terms Ponte (performed through unfused spinal segments) and Smith-Petersen Osteotomy (performed through fused spinal segments) are often used interchangeably. For this reason, we prefer use of the term posterior column osteotomy (PCO) to refer to any osteotomy which removes posterior column bony and soft tissue elements. 72
In modern adult spinal deformity surgery, the PCO is the most versatile osteotomy and represents the “work horse” in most practices. It is most effective when attempting to correct smooth or non-angular deformities. Because PCO’s can be performed at multiple levels in a reproducible, expedient, and safe manner, they represent a powerful tool for global deformity correction. Cho et al, showed that sagittal correction of up to 10.7° per level can be achieved with a PCO.73,74 Furthermore, they found that the use of at least 3 PCO’s offers comparable sagittal correction to a pedicle subtraction osteotomy with nearly half the blood loss. In addition to sagittal correction, PCO’s are a powerful technique for “deconstructing” stiff scoliotic curves in order to facilitate coronal correction. Nonetheless, these techniques have their limitations as they are significantly less effective in the setting of angular kyphotic deformities or in the presence of circumferential fusion mass (Figure 9). This is a case example of a 64 year-old female presenting with degenerative scoliosis and coronal as well as sagittal malalignment. Her sweeping thoracolumbar kyphosis was corrected with multilevel posterior column osteotomies. To correct the coronal imbalance, a kickstand rod was utilized.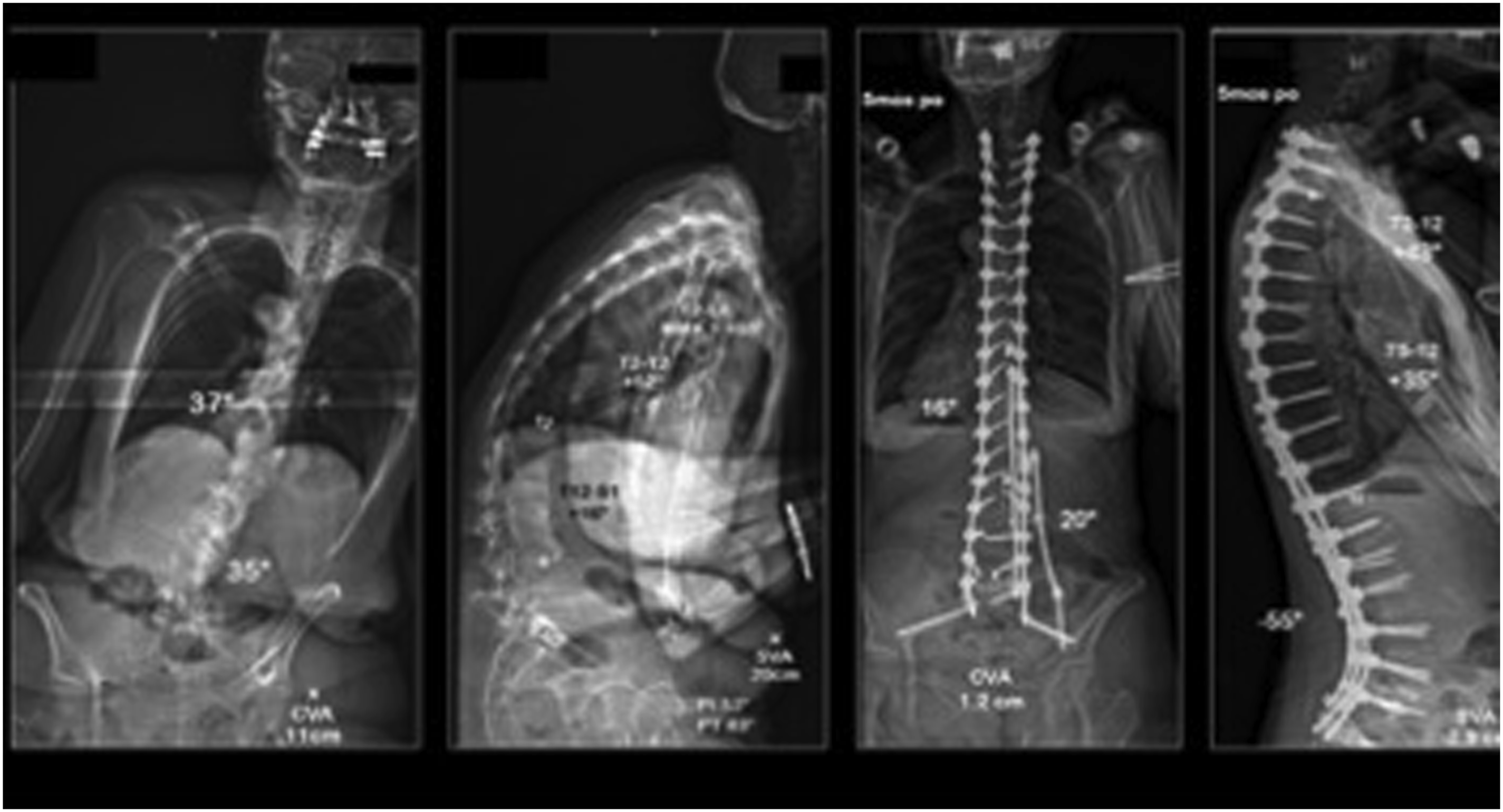
Pedicle Subtraction Osteotomy
Pedicle subtraction osteotomy (PSO) is a technique by which the posterior elements including the facets and ligamentum flavum are excised, followed by pedicle excision bilaterally and removal or decancellation of a wedge of the vertebral body. A compressive force is then applied through the posterior column using the anterior longitudinal ligament as a fulcrum. PSO’s are also commonly referred to as closing wedge osteotomies or eggshell osteotomies. Additionally, removal of the superior vertebral endplate and supra-adjacent disc may be referred to as an “extended” PSO. Schwab et al further classified the classic PSO and extended PSO as grade 3 and 4 osteotomies respectively. 75
PSO are a powerful osteotomy which is typically indicated for patients with rigid/fixed deformities in need of significant sagittal and/or sagittal and coronal correction and in patients where circumferential fusion limits the efficacy of PCO’s.73,76 Additionally, the use of asymmetric pedicle subtraction osteotomies can result in significant coronal correction. While a PSO may be utilized in the thoracic spine, they are more commonly performed in the lumbar spine where more impact on sagittal correction can be achieved.
77
Cadaveric models have demonstrated PSO can achieve 36.4 degrees of kyphotic correction for Schwab grade 3 osteotomies and 48.5° for Schwab grade 4 “extended PSO”.
78
Likewise, numerous clinical retrospective studies have demonstrated sagittal correction per level ranging from 26.2 to 40.1°.79-83 Despite being a profound tool for inducing sagittal correction, PSO’s are more technically challenging and have a greater complication profile when compared to posterior column osteotomies alone. The most common complication reported with PSO’s are transient neurologic, especially nerve root, deficits ranging from 3.7% to 19.5%.79,81,84-86 Another commonly reported complication is pseudarthrosis following PSO's. Additionally, PSO's have longer operative times and carry the risk of greater blood loss when compared to sequential PCO’s
73
(Figure 10). This is a case example of a patient who underwent a prior fusion in a “flat-back” position. She presented with significant sagittal imbalance and disability. CT scan demonstrated multilevel pseudarthrosis. She underwent a “sandwich PSO” at L5 with 50 degrees of correction and excellent overall sagittal alignment.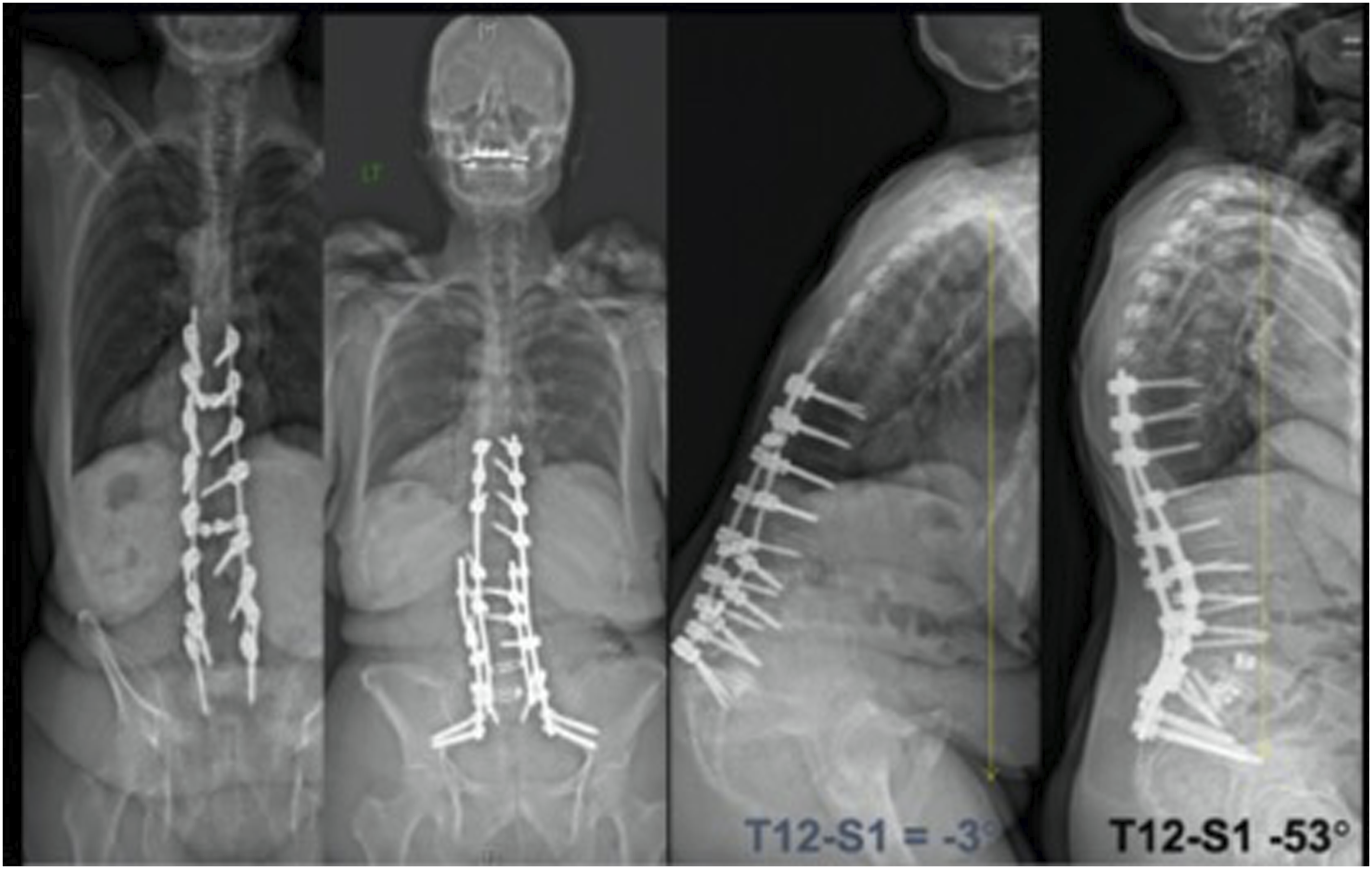
Vertebral Column Resection
The description of vertebral column resections (VCR) for the treatment of various spinal pathologies dates back nearly one century. 87 pVCR is most commonly indicated in cases of severe thoracic or thoracolumbar acute, angular kyphotic deformities. It is additionally a powerful technique for correction across a circumferentially fused deformity, particularly in the thoracic spine. Similar techniques have been described for the excision of hemivertebrae, congenital kyphoscoliosis, spondyloptosis, as well as for the treatment of bony spinal tumors.76,88-92 The technical aspects of a pVCR include removal of all posterior elements from the vertebral body including the superior and inferior facets. A total discectomy is performed at the cephalad and caudal discs with removal of the entire vertebral body. This allows for powerful deformity correction by essentially disarticulating the spine. Anterior column support by use of a titanium cage or structural allograft/autograft is recommended. This allows for a biomechanically superior construct, facilitates sagittal correction, and serves as a nidus for anterior column fusion.
Suk first described the pVCR for the treatment of spinal deformity in 70 patients with correction of 61.9% in the coronal plane and 47.5° in the sagittal plane with 2.53 cm restoration of coronal balance and 2.77 cm restoration of sagittal balance. 93 Lenke et al, reported on the first North American series of adult and pediatric patients undergoing pVCR for spinal deformity. 94 Patients were divided into 4 main groups: severe scoliosis, global kyphosis, angular kyphosis, and kyphoscoliosis with correction rates of 69%, 54%, 63% and 54% respectively. In 2013, Lenke et al published on the largest series of pediatric VCR’s in the literature comprising 127 pVCR and 20 circumferential VCR’s. 95 Their cumulative results showed an improvement of 54% in the coronal plane and 47% in the sagittal plane. Of note, there was no difference in complication rates between pVCR and circumferentially performed VCR, nor was there a difference in staged vs single-stage VCR procedures. Numerous other studies have likewise found between 50% and 70% correction in the coronal and sagittal plane following VCR procedures.96-102
Despite excellent clinical and patient reported outcomes, VCR’s remain a technically demanding procedure with the potential for significant perioperative morbidity. Bradford’s first report of a stage circumferential VCR demonstrated an operative time of 10.5 hours and EBL of 5800 mL. 103 Bradford and Tribus, likewise showed surgical times of 12.2 h and an EBL of 5500 mL. 104 While the use of posterior only VCR’s has shown to significantly reduce operative time and perioperative bleeding, it still remains a significant risk. Suk et al demonstrated an operative time of 4.5 h and mean EBL of 2333 mL in his series of 70 patients. 93 Lenke et al, likewise reported that operative time was significantly less for pVCR (486 min) vs circumferential VCR (639 min), but no statistically significant difference in EBL was demonstrated between the 2 procedures. As expected, staged procedures had much greater EBL and operative time than single-stage procedures. 95 Advancements in pharmacologics, particularly the use of anti-fibrinolytic agents has been shown to significantly reduce blood loss in vertebral column resection procedures. 105
Due to extensive operative times, surgical site infection remains a concern when performing VCR’s. Pull ter Gunne et al, reported a significantly higher risk of deep SSI with PVCR (9.7%) than PSO (3.4%) and PCO (1.5%). 106 While there were no differences in superficial SSI, VCR did have the highest overall SSI rate of 11.1% (vs 4.8% for PSO and 2.9% for PCO). Other authors have reported rates of SSI requiring return to OR ranging from 3%-9%.98-100 Lastly, due to the complexity of these procedures, changes in intraoperative neuromonitoring are common, seen in roughly 1 in 4 cases. The vast majority of these changes can be corrected with surgical intervention. The risk of permanent neurologic complication (either root or spinal cord) ranges from 2% to 6% in the literature.93-95,98,99
Technical Considerations
Thoracic VCR’s may require resection of the ribs either unilaterally or bilaterally. Typically, 5 cm of rib is resected in addition to the transverse processes, exposing the lateral aspect of the vertebral body. Following dissection with Penfield elevators, the nerve roots on the convexity are clamped for 5 min while continuously evaluating for neuromonitoring changes prior to ligation. Commonly, the nerve root on the convexity is clamped and ligated while the concave root may be preserved. Prior to performing a VCR, the spine should be stabilized with a temporary rod fixed to pedicle screws at least 3 segments above and below the desired VCR site. In instances of severe kyphosis, dual stabilization rods are recommended. If there is a fusion mass present, then hooks placed above and below the planned VCR site can be used both for stability and for correction via compression through the hook-rod construct. 107 The vertebral body is typically rotated laterally and dorsally on the convexity of the deformity.
In this manner, much of the bony corpectomy can be performed from the convex side. The lateral body can be dissected and protected with a malleable retractor. The concave pedicle(s) can be removed either prior or following the convex corpectomy. Often, spinal shortening can be obtained with convex compression that can relieve some of the neural tension on the neural elements against the concave pedicle, and thus is beneficial during the gentle, but necessary, concave dural protection. The concave pedicle is always very sclerotic and should be burred away or removed carefully with a kerrison rongeur while limiting dural retraction. A thin portion of the anterior vertebral body can be left intact, attached to the anterior longitudinal ligament to promote fusion. The posterior wall is the last to be removed in order to limit epidural bleeding and protect the spinal cord.
The correction maneuvers involve shortening and translation of the vertebral column. This can be achieved by direct compression across the convexity if there is good bony screw purchase or through construct-to-construct compression. The spinal cord should be monitored constantly to assess for stretch or buckling. Following shortening, an anterior cage is placed to help restore anterior column support, serve as a fulcrum for kyphosis correction, and prevent excessive shortening and spinal cord buckling that can produce neuromonitoring changes/data loss. 108
Once the correction has been achieved across the temporary rod, the contralateral final rod may be inserted along with additional support rods. Structural allograft or autograft may be placed dorsally over the laminectomy site to both protect the neural elements and to facilitate fusion (Figures 11A and 11B). (A) This is a case example of a patient with neurofibromatosis presenting with myelopathy and 180 degrees of thoracic kyphoscoliosis. Due to the sharp and rigid angular deformity, a 3 level VCR was performed resulting in decompression of the neural elements as well as significant improvement in radiographic and clinical imaging. (B) This is a case example of a patient with neurofibromatosis presenting with myelopathy and 180 degrees of thoracic kyphoscoliosis. Due to the sharp and rigid angular deformity, a 3 level VCR was performed resulting in decompression of the neural elements as well as significant improvement in radiographic and clinical imaging.
Minimally Invasive Surgical (MIS) Techniques in ASD Surgery
In the past 2 decades, there has been tremendous progress made in the use of MIS techniques for ASD surgery.109-114 At the heart of these methods has been the use of MIS anterior or lateral approaches to the thoracolumbar spine, 115 along with MIS placement of posterior pedicle screw-rod constructs often by what is referred to as “percutaneous” techniques. 116 The goals behind these advanced procedures are to replicate the indirect decompression, anterior stabilization and fusion and posterior correction, stabilization and +/− fusion being performed through formal open anterior and posterior approaches through less invasive means. There has been much focus on the types of patients and procedures most likely to benefit from MIS approaches, and the MISDEF algorithms have spearheaded these efforts from a multicenter/surgeon approach. 109 The MISDEF algorithm considers the amount of coronal scoliosis, lumbar, lumbosacral and global sagittal malaligment and whether the thoracic spine is also involved in the pathology to produces levels of MIS surgical complexity. For lower levels, MIS approaches are recommended and beneficial, but at the highest levels of ASD deformity, the MIS approach is suboptimal and conventional open approaches are recommended. Certainly there are individual surgeon and patient variables that go into the appropriate treatment selection, but these algorithms have played a key role in guiding the proper use of these MIS techniques for producing optimal patient outcomes. This field will only continue to evolve as enabling technology such as robotics, navigation, AR and VR become more commonly available in operating rooms across the world.
Intraoperative Correction Techniques
Cantilever Technique
In engineering, a cantilever is defined as a projecting beam or girder which is fixed only at 1 end. While various cantilever techniques have been described in the literature, the most common technique used in adult spinal deformity surgery is an applied moment arm cantilever technique. 117 Using this technique, a moment arm can be applied to the fixed structure (pedicle screw) either during insertion or following fixation of the cantilever rod. These forces can include distraction, compression, or bending through the fixed cantilever. However, the most common application of this technique in ASD surgery is using the insertional force from the cantilever to reduce the spine to the fixed rod. This is typically achieved by fixing the rod to the sacrum and/or ilium. The surgeon will then sequentially reduce the rod to the fixed pedicle screws. This technique is highly effective for correction in both the coronal as well as sagittal plane. It is particularly effective for removing kyphosis at the thoracolumbar or thoracic spine. When performing this technique, it is important to note that enormous stress is placed on the interface between the screw and the bone. To minimize these stresses, load sharing the rod across multiple pedicle screws at a time, while slowly and sequentially tightening them down should be considered. The use of reduction or extended tab screws is particularly helpful when using the cantilever technique.
Vertebral Translation
Vertebral translation involves the reduction of the spinal column to a fixed rod. As opposed to the cantilever technique where only 1 side of the rod is rigidly fixed, vertebral translation involves fixation of a rod to both the cephalad and caudal anchors. The intervening vertebral bodies are then sequentially translated to the rod through use of reduction instruments or with reduction pedicle screws. In severe deformity, the rod can be positioned to initially capture all of the apical screws and then rotated into the desired sagittal plane. The rod will often be over-contoured, allowing for viscoelastic creep in the system. It is a particularly effective technique for inducing kyphosis in the thoracic spine. Similar to the cantilever technique, vertebral rotation can place significant stress on the screw bone interface. Therefore, it is recommended that reduction be performed in a slow, sequential manner with load shared across multiple screws at once. The surgeon should be vigilant in assessing for screw pullout, especially in patients with poor bone quality or dysplastic pedicle anatomy where fixation is tenuous.
Compression/Distraction
Compression and distraction are techniques which allow the surgeon to increase or shorten the interpedicular distance between 2 vertebrae along a fixed rod. This can be applied to a single segment or over multiple segments, inducing a global corrective maneuver. It is important to appreciate that compressive and distractive forces impart two-dimensional segmental correction. In this manner, any posterior compressive force is additionally lordogenic. Conversely, posterior distraction induced between 2 vertebrae will be kyhpogenic. Understanding this concept is critical when attempting to correct across multiple curves in a deformity patient. The decision to first impart compression to a convexity versus distraction to a concavity may be highly influenced by the need to generate kyphosis or lordosis at that segment. In some instances, compression/distraction can be applied for uniplanar correction exclusively, such as achieving even shoulder balance or attempting to horizontalize the lower instrumented vertebrae (LIV). It has been demonstrated that the inferior pedicle pole is stronger than the superior pole, and thus repetitive forces applied against the inferior pole (e.g. compressing a pedicle screw caudal) will provide better correction prior to any bone-screw interface failure than forces applied to the superior pole (e.g., compressing a pedicle screw cephalad)
118
(Figure 12A and B). (A) Radiographic example of the use of cantilever technique to correct a main lumbar curve. The rod should be first placed on the convexity of the lumbar curve. Subsequent compression will further drive lordosis in the lumbar spine. Sequential reduction of the rod to the screws will additionally correct excessive thoracolumbar kyphosis. (B) Radiographic example of the use of cantilever technique to correct a main lumbar curve. The rod should be first placed on the convexity of the lumbar curve. Subsequent compression will further drive lordosis in the lumbar spine. Sequential reduction of the rod to the screws will additionally correct excessive thoracolumbar kyphosis.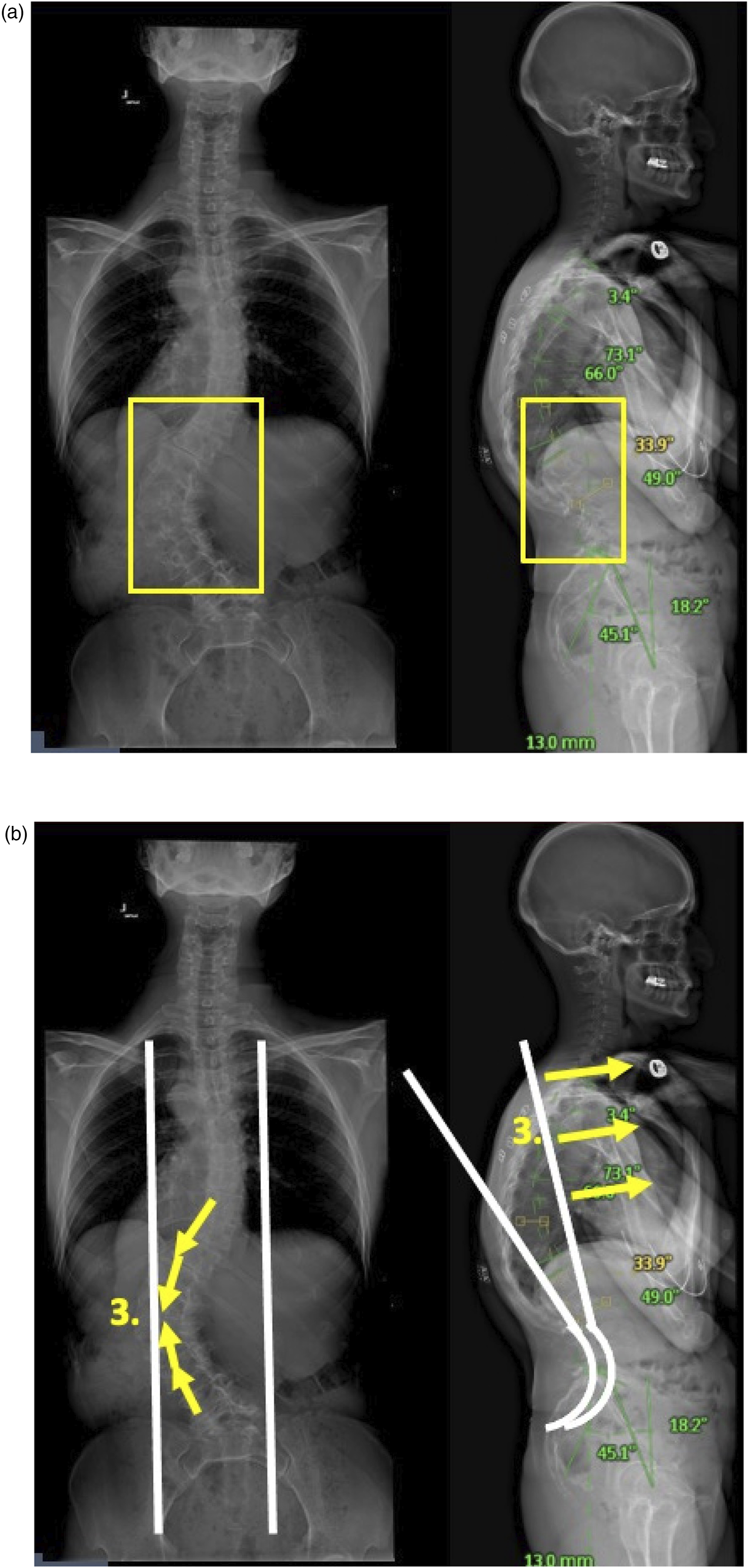
In-Situ Contouring
In-situ contouring is the process of inducing scoliosis, lordosis, or kyphosis on a rod following its fixation to pedicle screws. This technique is typically utilized following one of the previously described maneuvers when there is residual scoliosis or kyphosis. Care should be paid to the angles at which in-situ correction is applied. If the force is applied in a purely coronal or sagittal plane, then the correction will be one-dimensional. However, if the force is applied in an oblique plane, then the bending will induce a degree of both coronal and sagittal correction. When using large diameter rods, simultaneous bending between the surgeon and the assistant is recommended to maximize the force imparted on the stiff rod. Conversely, in-situ contouring is less effective when using smaller diameter or titanium rods due to higher degrees of elasticity.
The following adult spinal deformity case illustrates all of these differing types of correction maneuvers for this patient undergoing a long standing adult idiopathic thoracolumbar scoliosis deformity.
It is critical to obtain adequate radiographic images following spinal deformity correction to document the desired correction and alignment. In patients treated with instrumentation and fusion from the thoracic spine to the sacrum and pelvis, this will require images spanning from the cervico-thoracic region to the sacrum/pelvis in both the frontal and sagittal plane. The surgeon needs to work with their hospital radiology departments and technicians to determine which will be the optimal means to achieve this. One method is to stitch 2 short-cassette images in each plane together into a “long cassette” image. Whatever method is utilized, these images need to be thoroughly evaluated to ensure the alignment is acceptable or needs to be adjusted at that point in time while the wound is still open (Figure 13) In the vertebral translation technique. The rod is affixed proximally and distally. The vertebra are reduced to a hyper-contoured rod through use of reduction screws or reduction towers.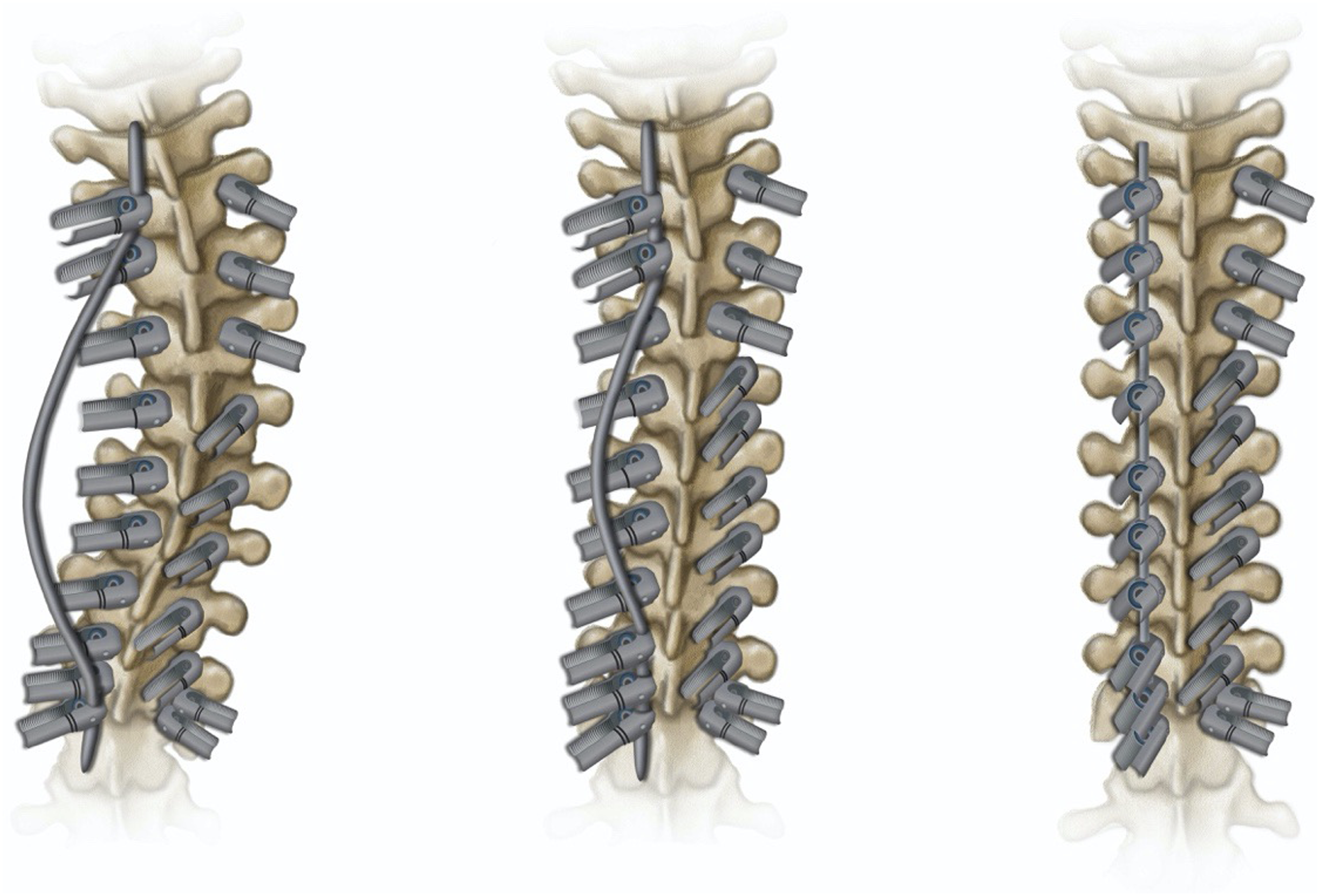
Limitations
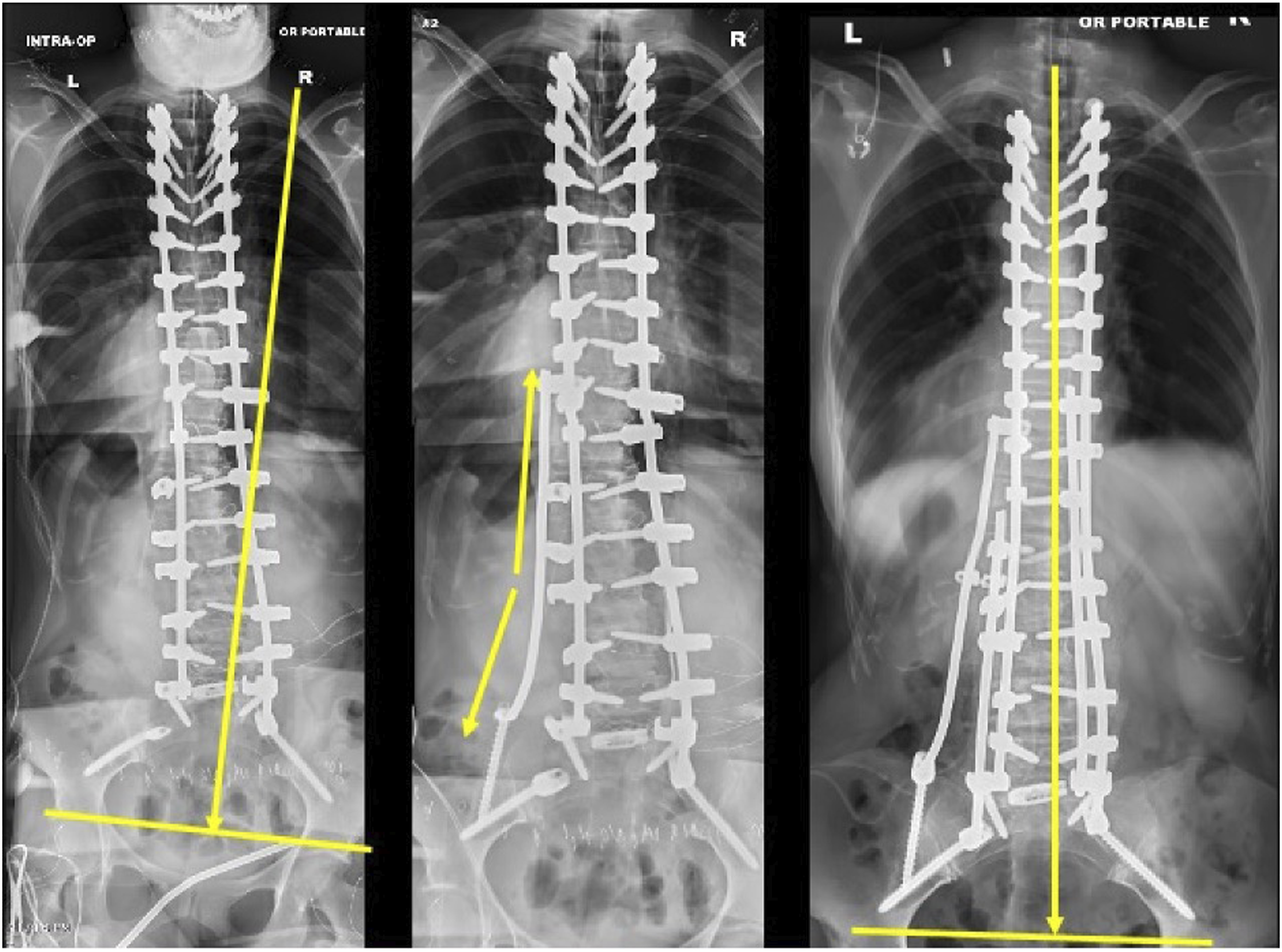
This review is not without limitation. Due to its non-systematic format, this review is limited by its potential subjectivity and lack of a standardized methodology. Instead, this review relied primarily on the exposure, expertise, and experience of the authors to provide a critical review and suggestions to the preoperative and intraoperative considerations that should be assessed in the treatment of ASD. The authors are well-versed with the literature and available treatment methods utilized in the discipline. However, the lack of a standardized methodology can potentially introduce bias in the review. In addition, this review may not provide a comprehensive overview of all the relevant research topics in treating ASD. Nonetheless, the authors used their experience and expertise backed by relevant sources in the literature to provide a comprehensive review of the topic at hand (Figures 14 and 15). (A) Radiographic example of the use of compression and distraction to correct the lumbosacral fractional curve with the ultimate goal to horizontalize L4. Compression will begin in the convexity of the fractional curve to drive lordosis. This will be followed by concave distraction. (B) Radiographic example of the use of compression and distraction to correct the lumbosacral fractional curve with the ultimate goal to horizontalize L4. Compression will begin in the convexity of the fractional curve to drive lordosis. This will be followed by concave distraction. (C) Radiographic example of the use of compression and distraction to correct the lumbosacral fractional curve with the ultimate goal to horizontalize L4. Compression will begin in the convexity of the fractional curve to drive lordosis. This will be followed by concave distraction. Use of the kickstand rod to correct residual pelvic obliquity or coronal malalignment measured intraoperatively from the central sacral pelvic line (CSPL).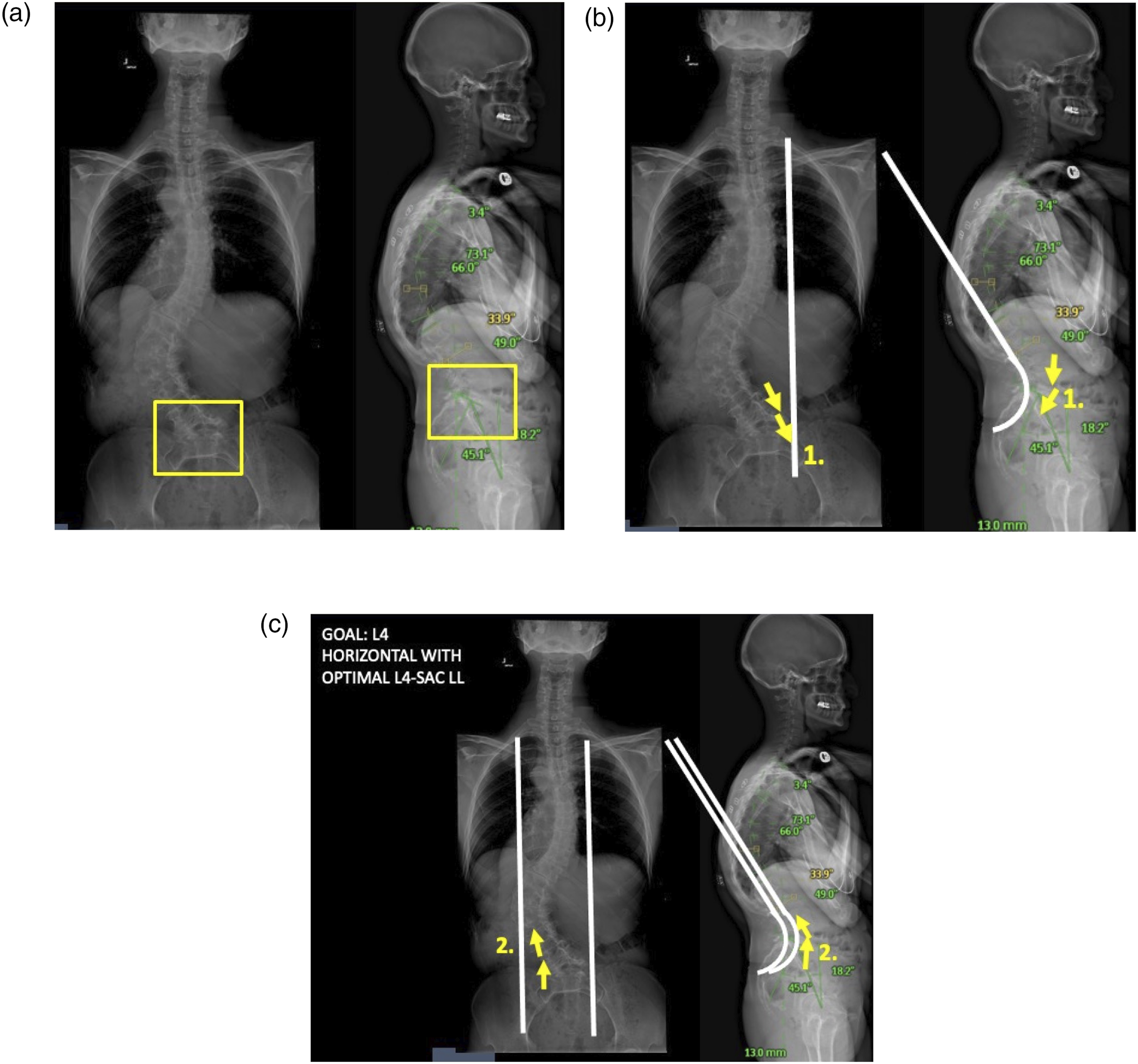
Conclusions
Detailed and thorough preoperative planning, patient optimization, and technical execution of ASD surgery is critical to obtaining a successful result while limiting complications. Although much improvement has occurred in the past two decades in this field, the use of big data, machine learning and artificial intelligence will likely revolutionize these components to ASD patients and their surgical reconstructions in a beneficial way going forward. Thus, we are on the cusp of a major revolution in the way ASD patients are evaluated preoperatively, and the way surgical decisions will be made in order to create more individualized modules of treatment. Additionally, increased use of intraoperative navigation aids, robotics and other assistive and enabling techniques and devices will provide more streamlined and reproducible implant placement and realignment methods confirmed during the procedure. As with any area of medicine or surgery, standardization of evaluation and treatment will provide decreasing variability and will likely improve outcomes and optimize the value equation of these major resource intensive surgical interventions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was organized and financially supported by AO Spine through the AO Spine Knowledge Forum Deformity, a focused group of international Adult Spinal Deformity experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Support was provided directly through AO Network Clinical Research.