
Abstract
Study Design:
Retrospective Cohort Study.
Objectives:
Ossification of the posterior longitudinal ligament (OPLL) reveals heterotopic ossification in the spinal ligament. OPLL also tends to ossify ligaments and entheses throughout the body. However, hallmarks of sacroiliac (SI) joint ossification and its variation in OPLL have not been clarified. Here, we investigated the morphological changes in SI joints in individuals with and without OPLL.
Methods:
We included 240 age- and sex-matched patients (OPLL+, 120; OPLL−, 120) in the study. SI joint variations were classified into 4 types: Type 1, normal or small peripheral bone irregularity; Type 2, subchondral bone sclerosis and osteophyte formation; Type 3, vacuum phenomenon; and Type 4, bridging osteophyte and bony fusion. Type 4 was further divided into 3 subgroups as previously described. Interactions between the ossified spinal region in OPLL and morphological changes in the SI joint were evaluated.
Results:
SI joint ankylosis occurs more frequently in patients with OPLL (51.7%) than in those without (non-OPLL) (33.3%). The SI joint vacuum phenomenon (49.2%) was the main finding in non-OPLL. SI joint ankylosis in OPLL was characterized by anterior bridging and intra-articular fusion. OPLL patients with multilevel ossification tend to develop degeneration and ankylosis of the SI joints.
Conclusions:
OPLL conferred a high risk of SI joint ossification compared with non-OPLL, and patients with extensive ossification had a higher rate of SI joint ankylosis. Understanding SI joint variation could help elucidate OPLL etiology and clarify the phenotypic differences in the SI joint between OPLL and other spinal disorders.
Keywords
Introduction
Spinal ligament ossification is a type of heterotopic ossification that occurs throughout the spine. Ossification of the posterior longitudinal ligament (OPLL) is characterized by progressive ossification of the posterior longitudinal ligament (PLL), causing severe neurological problems, such as myelopathy and/or radiculopathy. 1 OPLL has also been associated with other paraspinal ligament disorders, such as diffuse idiopathic skeletal hyperostosis (DISH) and ankylosing spondylitis (AS).2-9 Although OPLL, DISH, and AS share the features of bone proliferation and heterotopic ossification in the spine, the hallmarks of bone proliferation in the spine are dissimilar.
Our previous study demonstrated that more than half of the patients with cervical OPLL had coexistent OPLL in the thoracolumbar region. 10 Cervical OPLL predominantly affects men at a ratio of 2:1 to 3:1. 11 Conversely, patients with cervical OPLL coexisting in the thoracolumbar spine were significantly more often women. 10 DISH also predominantly affects men at a ratio varying from 2:1 to 7:1.12,13 The middle to lower thoracic spine in DISH is frequently ossified and introduces bony ankylosis, predominantly in men. 12 We also found that patients with DISH carried bony bridging and ankylosis not only in the anterior longitudinal ligament (ALL) of the spine but also in the sacroiliac (SI) joint. 14 On the other hand, AS is a common rheumatic disease affecting the spine and SI joints, predominately in men, and sacroiliitis is its earliest manifestation.15,16
The SI joint is the largest axial joint in the human body, linking the spine and the pelvis.17,18 It is stabilized by strong ligaments and ensures mobility between the sacrum and the iliac bone. 18 Those ligaments enclose the cartilaginous parts of the SI joints and represent a major site of entheses. 19 Degeneration of the SI joint is characterized by joint space narrowing, osteophytes, subchondral sclerosis, cysts, vacuum phenomena, and ankyloses.20,21 SI joint and spinal ankylosis (so-called “bamboo spine”) are considered a hallmark of AS. Moreover, SI joint bridging was strongly associated with entheseal reactions in other parts of the body. The presence of SI joint bridging indicates an intensive general entheseal process in the skeleton. 22 We previously showed that SI joint involvement in DISH is characterized by radiographic osteophytes, para-articular bony bridging, and coexistent osteoarthritis. 14 In contrast, intra-articular bony fusion, erosion, and sclerosis in the SI joint are frequently observed in AS. 14 Although patients with OPLL, DISH, and AS have a general tendency toward ossification in the spine and other skeletal entheses, we found no study that has addressed the morphological changes in the SI joint and their variation in patients with OPLL.
Therefore, the aims of the current study were 2-fold. One was to elucidate the variation in SI joint changes in a patient with OPLL. The second was to explore the association between OPLL ossification severity and SI joint variation with the aim of better understanding the hallmarks of bone proliferation in the spine and SI joint in patients with OPLL.
Materials and Methods
This study analyzed and compared the characteristics of SI joint variation in 2 different types of spinal disorders. The first included 120 patients (79 men, 41 women; mean age 71.4 years) with cervical OPLL, who were allocated to the OPLL+ group. The other included 120 age- and sex-matched patients (81 men, 39 women; mean age 71.3 years) with degenerative spinal disease without OPLL, who were allocated to the OPLL− group (Table 1). All patients were diagnosed in our university hospital based on the findings of plain radiographs and computed tomography (CT) images of the whole spine. This study was approved by the ethics committee at Toyama University Hospital.
Demographic Data of the Patients With Ossification of the Posterior Longitudinal Ligament and the Controls.

Abbreviations: OPLL, ossification of the posterior longitudinal ligament.
As previously reported, morphological changes of the SI joint were divided into 4 types based on CT findings: Type 1, normal or small peripheral bone irregularity; Type 2, subchondral bone sclerosis and osteophyte formation; Type 3, vacuum phenomenon of the SI joint; and Type 4, bridging osteophyte and bony fusion of the SI joint. Type 4 was further classified into 3 subgroups depending on the site of bony ankylosis, as previously described: anterior para-articular bridging (Type 4A), posterior para-articular bridging (Type 4B), and intra-articular ankylosis (Type 4C). 14 CT images of the whole spine and SI joint were evaluated by 2 orthopedic surgeons (NTCT and YY).
In patients with OPLL, the severity of the ossified lesions in the whole spine was evaluated using our previously published ossification index (OS-index). 10 In short, the index is determined by the sum of the number of vertebral bodies and intervertebral discs where OPLL is present. When the ossification area covers from the vertebral body level to the intervertebral disc level, the number of ossified lesions of each vertebral body level and intervertebral disc level is counted. The maximum OS-index is 14 in the cervical spine. The OS-index in the thoracic spine ranges from 0 to 24, and that in the lumbar spine from 0 to 11. The OPLL+ patients were also divided into 3 groups based on the severity of the ossification: Grade 1, OS-index <10; Grade 2, OS-index 10-19; Grade 3, OS-index ≥20 (Figure 1). The patients were also divided into the following 2 groups according to the OPLL region: OPLL only in the cervical spine (C group) or in multilevel spinal regions (M group). 10 The relationship was determined by comparing the region of OPLL and SI joint change.
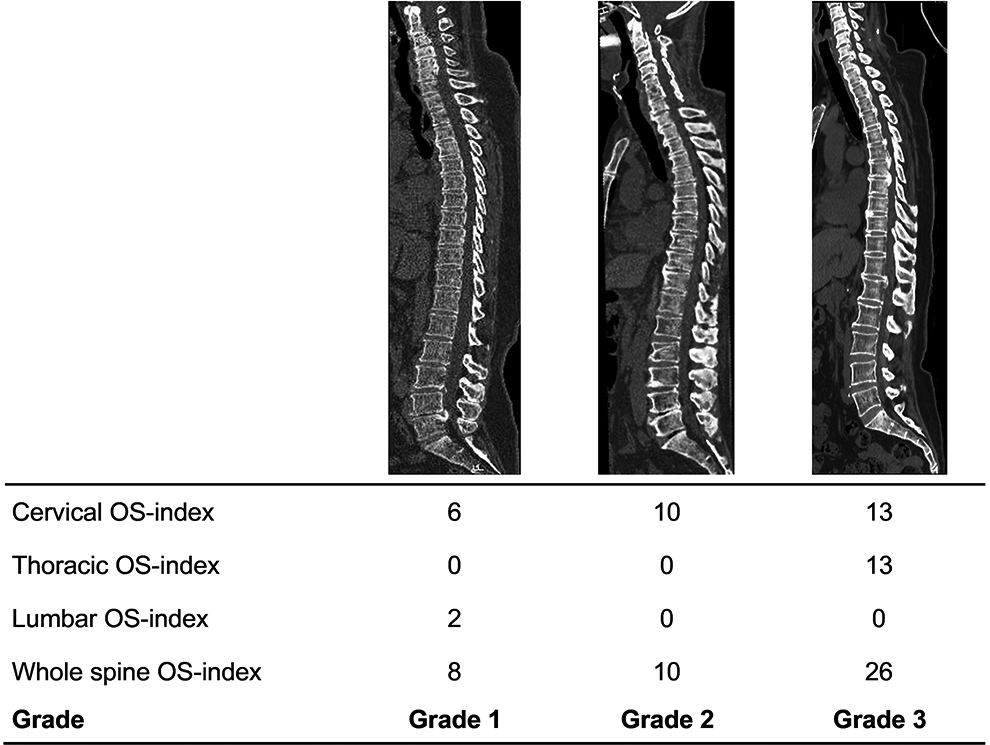
Representative sagittal computed tomography images of ossification of the posterior longitudinal ligament Grades 1, 2, and 3 of the OS-index. OS indicates ossification.
Statistical Analysis
The data is presented as the mean value ± standard deviation. We employed Student’s unpaired t-test for the statistical analysis of the difference in age and a 1-way analysis of variance followed by Tukey’s post hoc test to compare the OS-index between the SI joint classification groups. We used the chi-squared test for the statistical analysis of the difference in sex, the type of SI joint variation between OPLL+ and OPLL− group, between the C group and the M group, and between the OS-index grades. Excel statistical software (Statcel version 4; OMS, Tokorozawa, Japan) was used for the analysis, and P < 0.05 was considered as statistically significant.
Results
Both the OPLL+ and OPLL− groups presented SI joint degeneration, such as osteophyte formation (Type 2), SI joint vacuum phenomenon (Type 3), and SI joint fusion (Type 4). Type 1 involvement of the SI joint in both groups is a rare finding, and the majority of other cases were associated with SI joint degeneration more severe than Type 2 (Figure 2). There were significant differences in the prevalence of SI joint variation between the 2 groups (P < 0.01). Anterior and posterior bridging and fusion of the SI joint (Type 4) were detected frequently in the OPLL+ group (51.7%) compared with the OPLL− group (33.3%). Conversely, the SI joint vacuum phenomenon (Type 3) was the most frequent change in the OPLL− group (49.2%). In addition, there were significant differences in the ankylosis subclassification between the OPLL+ and OPLL− groups (P < 0.001). Anterior bridging of the SI joint (Type 4A) was the most common finding (82.9%) in the OPLL− group (Figure 3). On the other hand, anterior bridging (Type 4A; 33.9%) and intra-articular fusion (Type 4C; 56.5%) of the SI joint were mainly identified in the OPLL+ group.
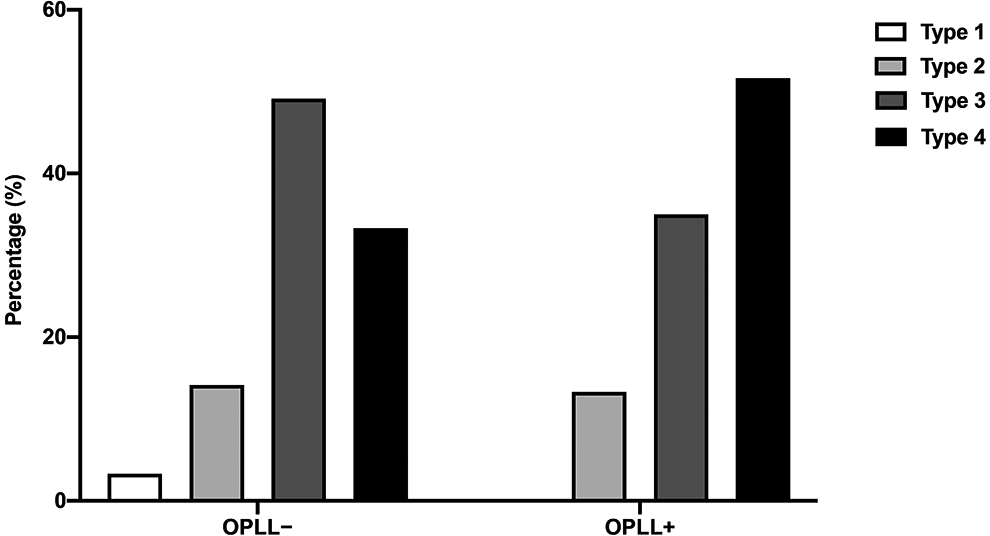
Prevalence of sacroiliac joint variation in patients with ossification of the posterior longitudinal ligament and controls.
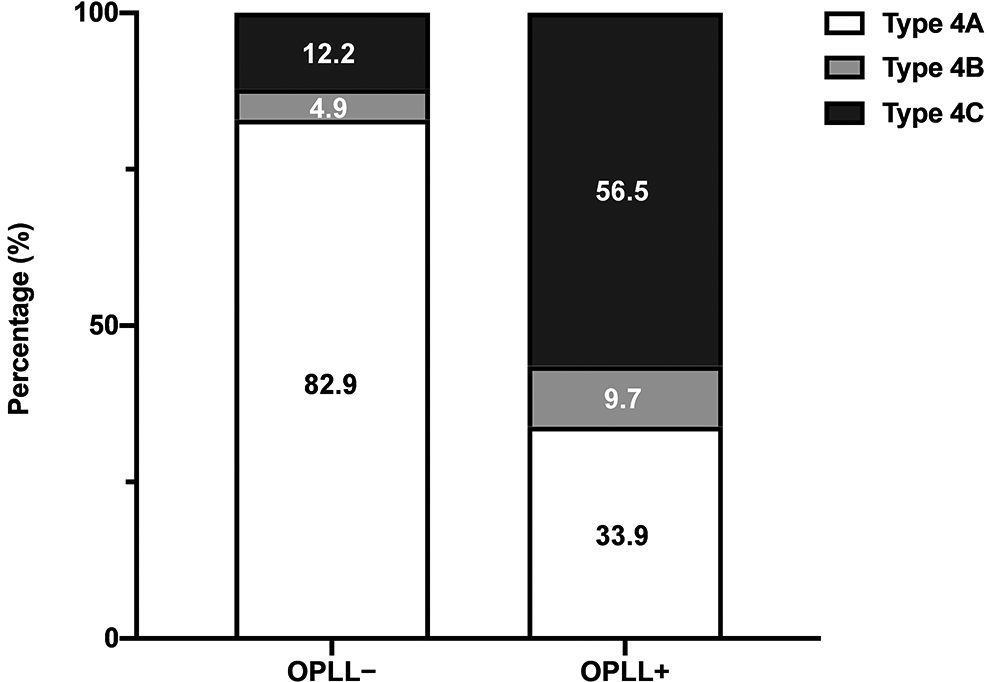
Prevalence of sacroiliac joint ankylosis in patients with ossification of the posterior longitudinal ligament and controls.
Approximately 60% of patients with cervical OPLL had coexistent OPLL in the other spinal regions (Table 2). Statistically significant differences were found in the SI joint classification and also in the Type 4 subclassification between the C group and the M group. The M group had a higher prevalence of SI joint Type 3 and Type 4 than the C group. Among those with Type 4 subclassification, no significant differences were found between the M group and the C group (Table 2).
The Relationship Between the Region of OPLL and SI Joint Variation.
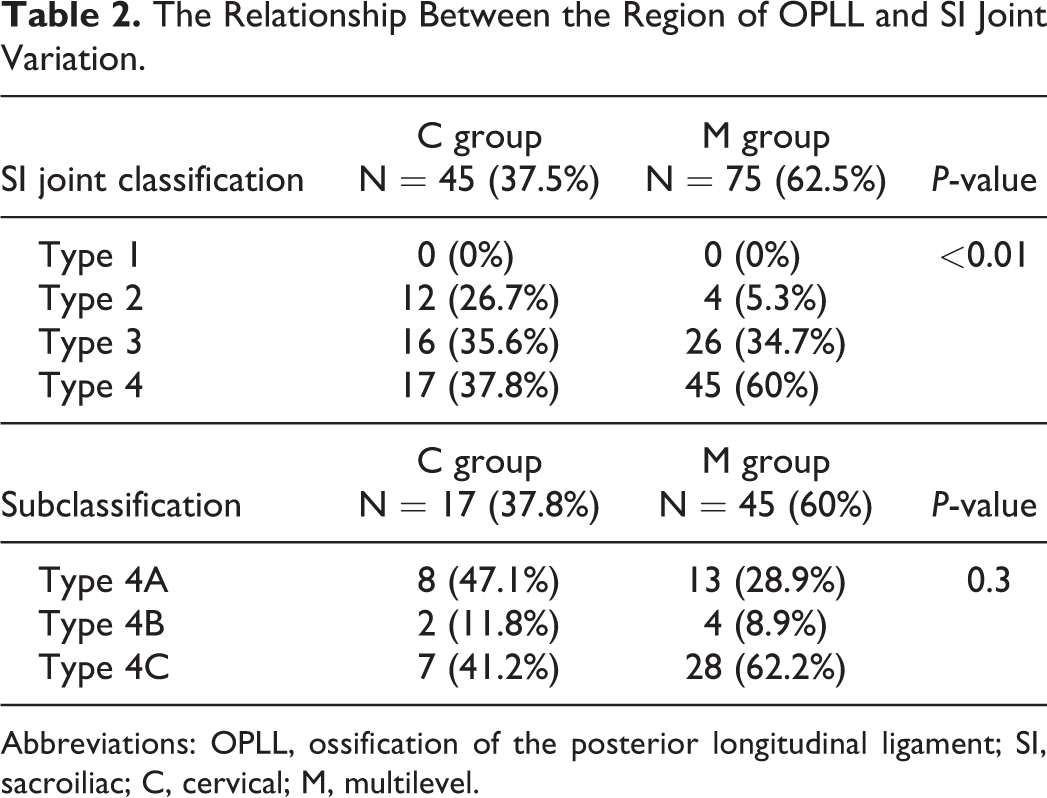
Abbreviations: OPLL, ossification of the posterior longitudinal ligament; SI, sacroiliac; C, cervical; M, multilevel.
The average OS-index was 10.7 ± 6.2, and it ranged from 1 to 34. The OS-index of the whole spine appears to correlate with the morphological changes of the SI joint. Patients with OPLL who have SI joint fusion (Type 4) present a significantly higher OS-index compared with those with Type 2 (Figure 4). However, there were no differences between the OS-index and the subclassification of Type 4. We also found that the SI joint tended to show a high rate of bony bridging and intra-articular fusion in patients who had OS-index Grade 2 or Grade 3 (Table 3).
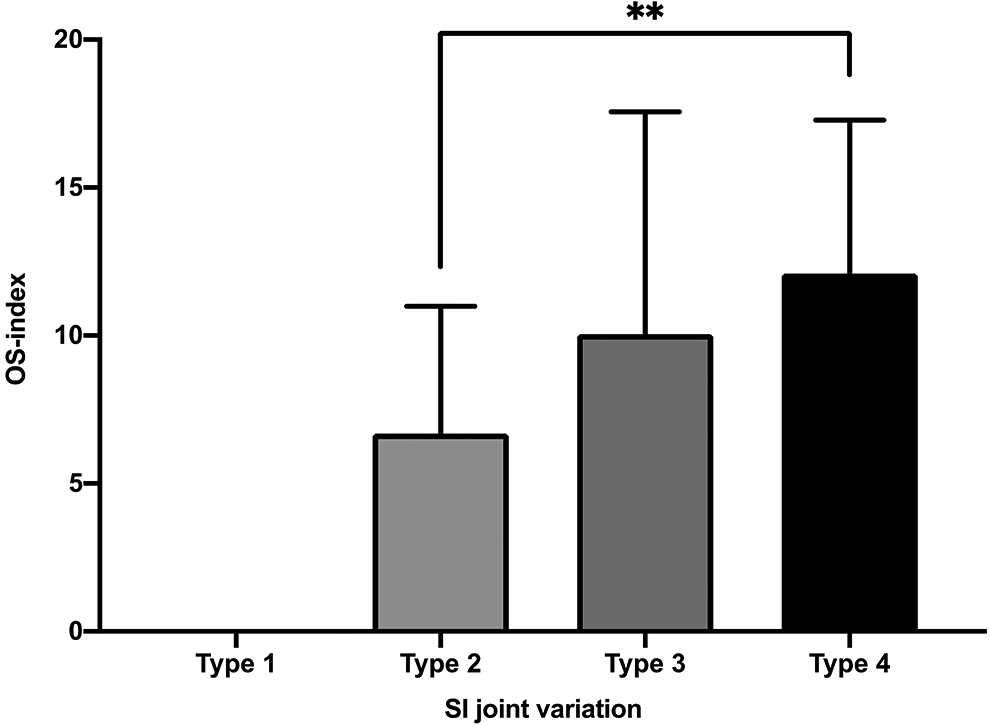
The OS-index of the whole spine is associated with SI joint variation. **P < 0.01; OS indicates ossification; SI, sacroiliac.
The Relationship Between OS-Index Grade of the Whole Spine and SI Joint Variation.
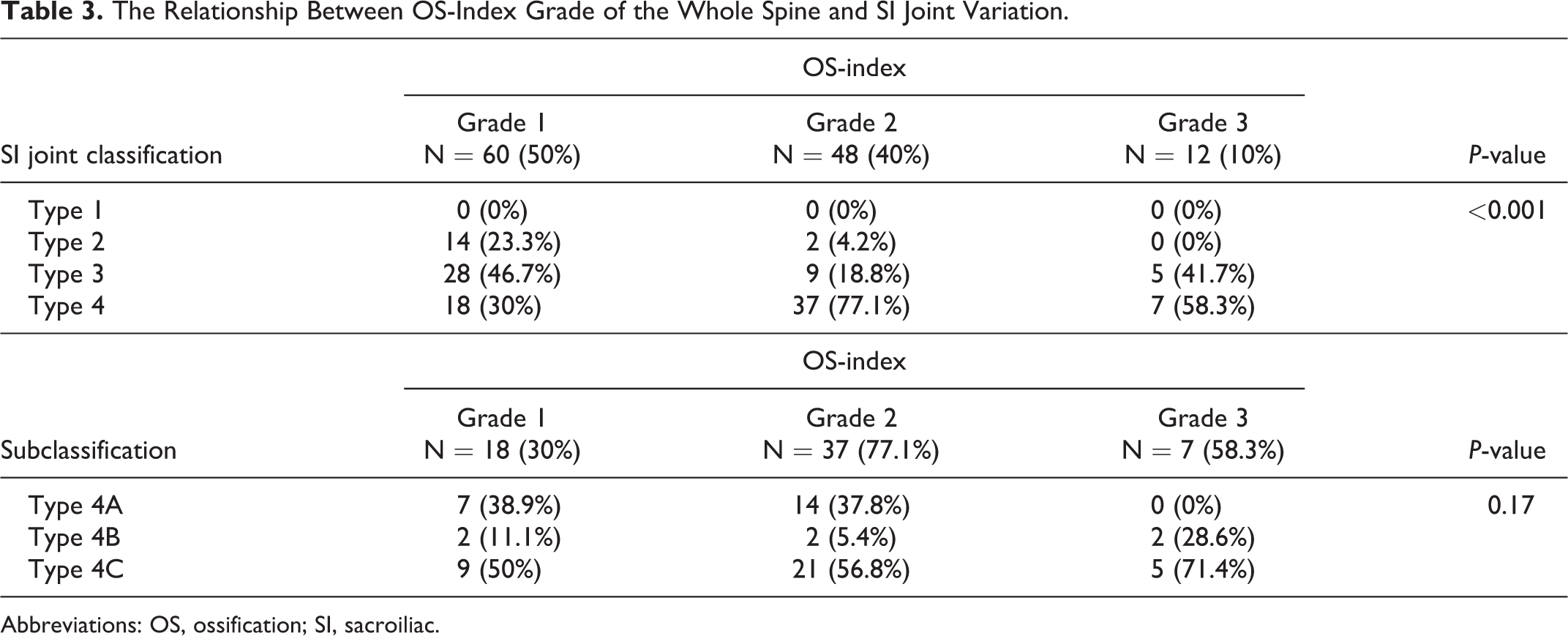
Abbreviations: OS, ossification; SI, sacroiliac.
Discussion
The present study demonstrated that the bony bridging and ankylosis of the SI joint (Type 4) occurred more frequently in the OPLL+ group compared with the OPLL− group. By contrast, the SI joint vacuum phenomenon (Type 3) was the main finding in patients with degenerative spinal disease without OPLL rather than SI joint ankylosis. Additionally, patients with OPLL with multilevel ossification or a high OS-index had a strong tendency to develop degeneration and ankylosis of the SI joints. Thus, the current study revealed a novel SI joint characteristic in patients with OPLL. These findings could provide valuable insight for understanding the tendency for heterotopic ossification in the spine as well as in the SI joint in OPLL.
Given OPLL and DISH share the standard features of a generalized ossification tendency in the paraspinal ligaments, OPLL has recently been recognized as one of the clinical features of DISH, which is characterized by ossification along the anterolateral aspect of vertebral bodies and peripheral entheses. Historically, Resnick et al showed that 50% of DISH cases were concomitant with OPLL, 2 and a retrospective multicenter study from the Japanese Organization of the Study for Ossification of the Spinal Ligament reported the DISH prevalence in patients with cervical OPLL was 48.7%, with older age as a significant correlating factor. 23 Sato et al 24 reported that OPLL plaque was contiguous with the ligamentous entheses to the vertebral body and to the deep layer of the PLL. Chen et al 25 indicated that OPLL might actually be a type of enthesophyte, or enthesopathy, of DISH.26,27 Given the sacroiliac joints are predominantly composed of fibrous connective tissues (fibrocartilage) and contain very little synovial fluid, these articulations can be considered entheses.28,29 Entheses could therefore represent a site of endochondral ossification, resulting in para-articular bony ankylosis of the SI joint. 30 Dar et al 22 studied 289 human male skeletons for the presence of SI joint bridging; they stated that SI joint bridging was strongly associated with “entheseal reactions” in other parts of the body. These features could explain why sacroiliac joint bridging occurs significantly more frequently in patients with OPLL as well as in DISH as a result of all-body entheseal reactions.
However, our current study showed that the SI joint fusion pattern was dissimilar between OPLL and DISH. Both anterior bridging (Type 4A; 33.9%) and intra-articular ankylosis (Type 4C; 56.5%) of the SI joint were mainly identified in patients with OPLL. On the other hand, we previously found that SI joint involvement in DISH was characterized by anterior bridging (Type 4A; 71.6%) rather than intra-articular ankylosis (Type 4C; 23%). OPLL and DISH share the features of bone proliferation and heterotopic ossification in the spine; however, we considered that the different underlying mechanisms might partially affect the phenotype of the SI joint ankylosis, meaning these 2 diseases should be in different disease categories. Further study is warranted to understand the meaning of the phenotypic variation of the SI joint, and the data will provide us with a new way to recognize the characteristics of bone proliferation and ossification in OPLL as well as in other spinal disorders, such as DISH and spinal degeneration.
Enthesopathy had long been considered as a rheumatic or metabolic disorder,26,27 categorized as inflammatory or noninflammatory. AS is a type of spondyloarthritis, which is characterized by enthesitis of the spine and SI joint.15,16 Sacroiliitis in AS includes joint erosions, joint space narrowing, sclerosis, and intra-articular ankyloses. 14 Given both AS and OPLL have a similar tendency toward SI joint intra-articular fusion, both diseases might have a similar etiology related to inflammatory-related enthesitis. We previously found that the serum level of high-sensitivity C-reactive protein (hs-CRP) in the patients with OPLL was higher than that in individuals without OPLL, indicating that systemic inflammation might be an important factor regarding the pathogenesis of OPLL. 31 Some other studies have reported that increased CRP was frequently observed in patients with painful axial AS and was correlated with both the activity and the functional severity of the disease.32,33 Furthermore, elevated serum hs-CRP levels have occurred simultaneously with inflammation at the SI joint. 34 Therefore, some combination of systemic factors might act on these degenerative changes simultaneously in the SI joint and in the vertebral column in OPLL. These findings give us a hypothesis that there is some form of an inflammatory basis for the progressive bone formation in the spine and SI joint in OPLL. Further studies will be necessary to provide evidence that systemic inflammation leads to excessive bone formation in the spine and SI joint in OPLL. However, the insight about the interaction between inflammation and bone formation might help us understand its etiology and develop a novel anti-inflammatory intervention that has therapeutic effects on bone formation and the progression of OPLL.
A previous study indicated that the extent of OPLL in the whole spine is significantly associated with the extent of the OS-index. 35 The present study revealed that patients with a high OS-index tended to show a high rate of bony bridging and intra-articular fusion of the SI joint. This finding could suggest that SI joint degeneration reflects a general ossified tendency in the spinal canal and indicates the severity of the ossified lesions. We also found that the SI joint in the patients with OPLL at multiple spinal levels showed a greater tendency toward bony ankylosis compared with patients with OPLL only in the cervical region. Although the process of ossification remains unknown, it has been well documented that prognosis and surgical outcomes are poorer in patients with multiple-region OPLL than in patients with cervical lesions alone, 36 and the increase in the area of ossified lesions affects the surgical results after laminoplasty.37,38 Therefore, it is clinically important to clarify the factors associated with the extent of ossification not only in the whole spine but also in the SI joint. Thus, understanding the SI joint variation in OPLL and other forms of spinal disease could be, at least in part, helpful in its diagnosis and decision-making for the surgical strategy and in the development of novel therapeutics to prevent the bone formation and progression of OPLL.
This study had several limitations. First, the number of patients was small, and this is a retrospective and observational cross-sectional study. More extensive prospective studies are needed to substantiate our results and determine whether such SI joint findings correlate with the development of OPLL in a particular individual. Second, we did not evaluate the relationship between systemic inflammation and OPLL regions or OS-index grade and SI joint degeneration. Furthermore, the presence of SI joint inflammation on magnetic resonance imaging was not determined. However, this study might provide a greater understanding of the pathological conditions with systematic inflammatory tendencies in human axial skeletons.
Conclusion
In summary, we have identified SI joint variation in patients with OPLL. We have shown that anterior bony bridging and ankylosis of the SI joint are more frequently observed among patients with OPLL and that OPLL patients with multilevel ossification or high OS-index had a strong tendency to develop degeneration and ankylosis of the SI joints. Clarification of the SI joint variation will lead to a better understanding of the etiology of OPLL and clarify the phenotypic differences between OPLL and other diseases that cause spinal ligament ossification.
Footnotes
Authors’ Note
This study was approved by the ethics committee at Toyama University Hospital (Clinical research number 21-22). Patients provided written consent for participation in this analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the Japan Society for the Promotion of Science (JSPS) KAKENHI Grant Number 20K18023. The funding body played no role in the design of the study or in the collection, analysis, or interpretation of data or writing of the manuscript.