
Abstract
Purpose
To compare the surgical outcomes of modified expansive open-door laminoplasty (EOL) (C4-C6) and traditional EOL (C3-C7) in patients with cervical spondylotic myelopathy (CSM).
Methods
One hundred and two CSM patients were retrospectively recruited from Fujian Medical University Union Hospital between March 2012 and December 2019. Seventy-one patients with CSM underwent modified EOL, and 31 patients underwent traditional EOL. The primary endpoint was axial symptoms.
Results
Patients who underwent modified EOL had a significantly lower incidence of axial symptoms (odds ratio: 0.273; 95% confidence interval: 0.184-0.691; p = .002). The length of hospital stay (p = .263), and intraoperative blood loss (p = .402) were not significantly different between the groups. Significantly more postoperative drainage was observed in patients who underwent modified EOL (p < .001), while the cost of hospitalization in patients treated with traditional EOL was higher (p = .011). There were significant differences between modified and traditional EOL for the changes in range of motion (p < .001), modified Japanese Orthopaedic Association score (p = .001), and the Nurick grade (p = .014), while the changes of visual analogue scale (p = .250), and the neck disability index (p = .134) were not significantly different between the groups.
Conclusion
This study found modified EOL may decrease the incidence of axial symptoms in patients with CSM compared to traditional EOL.
Brief introduction
Cervical spondylotic myelopathy (CSM) is a common degenerative and debilitating disorder that leads to significant neurological deficits and is the leading cause of spinal cord dysfunction worldwide. 1 CSM is the most severe cervical disease and accounts for nearly 10-15% of cervical spondylosis. 2 This condition is a result of chronic compression of the spinal cord due to structural degeneration of intervertebral joints in the cervical spine, which leads to secondary, chronic, and progressive damage to the spinal cord, resulting in impaired spinal cord function. 3 Patients with CSM present with neck pain, limb dysfunction, mobility restriction, incontinence, and quadriparesis. Delayed or improper treatment of CSM is associated with progressive, irreversible nerve damage.4–6
The surgical treatment of CSM is increasing rapidly, and CSM-related hospitalizations account for 4.04 per 100,000 person-years.7,8 Surgical treatment for CSM aims to decompress the spinal cord via the expansion of the spinal canal. An anterior approach is used for patients with one or two segments with CSM, while a posterior approach is used when three or more segments are involved or when the patient has developmental canal stenosis. 9 Expansive, open-door laminoplasty (EOL) uses the “bowstring principle” of the cervical the spinal cord to move the cervical spinal backward through an open door. Posterior compression of the spinal cord is directly relieved via EOL, and anterior compression is also relieved, which could cause the compressed cervical spinal cord to be decompressed for ≥ 3 segments involved. 10 A previous study reported axial symptoms of CSM after EOL as neck, shoulder, and back pain accompanied by distension, stiffness, heaviness or muscle spasms. 11 A prior study found both C4-C7 single door cervical dilatation with total C3 laminectomy and C3-C6 single door cervical dilatation with retention of the C7 spinous process can reduce the incidence of axial symptoms by maintaining the stability of the posterior cervical muscle group and reducing the destruction of the posterior cervical muscle ligament complex. 12 This study aimed to compare the surgical outcomes of modified EOL (posterior approach at C4-C6) and traditional EOL in patients with CSM.
Materials and methods
Patients
One hundred and two patients with multi-level CSM who were treated at Fujian Medical University Union Hospital between March 2012 and December 2019 were included in this study. This study was approved by the Institutional Review Board of Fujian Medical University Union Hospital (2021KY165), and informed consent for all patients was signed prior to participation in the study. Patient records were retrospectively reviewed for preoperative symptoms of CSM, including neck stiffness, pain, limb fatigue, numbness, and walking instability. Physical examination findings such as decreased limb muscle strength, positive Hoffmann sign or positive dynamic Hoffmann sign, and compression of the cervical spinal cord on magnetic resonance imaging (MRI) were also extracted from the patient records. Preoperative cervical spine anteroposterior, lateral, hyperextension, and flexion x-rays were obtained for all patients. MRIs were obtained to confirm the diagnosis of CSM. Of the 102 patients included in this study, 71 underwent modified EOL and 31 underwent traditional EOL. One surgeon performed all of the surgeries in this study.
Patients presenting with clinical symptoms and imaging findings of CSM at more than one consecutive vertebral level with a positive Hoffmann sign or dynamic Hoffmann sign and at least three vertebral segments with spinal cord compression that did not improve with conservative treatment were included in this study. The exclusion criteria are listed as follows: patients diagnosed with cervical spondylotic radiculopathy, cervical instability, or cervical spondylolisthesis, history of traumatic cervical vertebral or spinal cord injuries, metabolic bone disease, spinal tumors, tuberculosis, previous spinal surgery, and circulatory, respiratory, nervous, hematopoietic, or other complicated diseases.
Surgical procedures
In the modified EOL group, the patients were under general anesthesia delivered via tracheal intubation and intravenous access. The patient’s head was fixed in the prone position using a three-point neurosurgical head frame. The cervical spine was moderately flexed in a neutral position. Using a posterior approach, a longitudinal midline incision was made through the skin, subcutaneous tissue, and deep fascia to expose the neck muscles. The neck muscles were dissected, and the spinous processes were used as anatomical markers to locate the C3-C7 laminae. The laminae were exposed via subperiosteal dissection. The insertion of the cervical semispinales muscles at the C2 spinous process were preserved without dissection, and a laminectomy was performed at C3. Half of the cortical bone was retained on one side of the C4-C6 lamina, and the other side was completely cut open. The entry point of the ligamentum flavum at the upper margin of the C7 lamina was decompressed via sublaminal decompression. The compressed cervical spinal cord was observed to be swollen and pulsing. ARCH micro titanium plates were inserted into the laminae and the lateral blocks at the C4, C5, and C6 door sites, and two screws were used at each end for fixation. Autologous bone fragments were implanted in the gap between the C4-C6 gate axes. When the area was clean and bleeding had ceased, a negative pressure drainage tube was placed, and the incision was closed (Figure 1(a)). Surgical procedures in modified EOL group and traditional EOL group.
In the traditional EOL group, the same anesthesia delivery method and patient position were used. A longitudinal midline incision was also made using a posterior approach. The incision was made through the skin, subcutaneous tissue, and deep fascia to expose the neck muscles. The neck muscles were dissected, and the spinous processes were used as anatomical markers to locate the C3-C7 laminae. Part of the spinous processes were removed via spinous process shearing. The cortical bone was retained on one side of the C3-C7 laminae and opened on the contralateral side. The compressed cervical spinal cord was observed to be swollen and pulsing. An ARCH micro titanium plate was placed in the laminae and lateral plates were placed at C3, C4, C5, C6, and C7 and fixed with two screws at each end. Autologous bone fragments were implanted into the gap between the C3-C7 gate axes. When the area was clean and bleeding had ceased, a negative pressure drainage tubes were placed and the incision was closed (Figure 1(b)).
Postoperative management
All patients fasted for six hours postoperatively and were administered conventional analgesics for three days postoperatively. Diuretics and steroids were administered to reduce nerve root edema for five days postoperatively. The negative pressure drainage tube was removed on postoperative day 2 or 3 based on the volume of drainage. Rehabilitation began on postoperative day 2 when the patients were permitted to ambulate while wearing a neck brace. A rigid neck brace was worn for 4-6 weeks postoperatively. Follow-up visits were conducted at one, three, six, and 12 months postoperatively. Axial symptoms were treated via physical therapy, strategies to improve circulation, and strategies to relieve muscle spasms.
Outcomes
The primary outcome of this study was axial symptoms, which was defined as at least three of the following symptoms: neck pain with minor movements, neck stiffness, relief with a hot compress, or relief when laying in a supine position (Table S1).12,13 Secondary outcomes included the length of hospital stay, intraoperative blood loss, postoperative drainage volume, and cost of hospitalization. Other functional outcomes included the changes in range of motion (ROM), pain (measured using a visual analogue scale [VAS]), the neck disability index (NDI), the modified Japanese Orthopaedic Association (mJOA) score, and the Nurick grade.
Statistical analysis
Continuous variables are presented as mean (standard deviation) or median (interquartile range), and categorical variables are presented as event and proportion. Continuous variables were analyzed using a t test or the Kruskal-Wallis test, as indicated based on distribution. Categorical variables were analyzed using the adjusted chi-square test or Fisher’s method. Multivariate logistic regression analyses were used to determine the effects of modified EOL and traditional EOL on the risk of axial symptoms. Statistical significance was set at p < .05, and all p values are two-sided. All statistical analyses were conducted using SPSS version 13.0 statistical software (manufacturer name, Chicago, IL, United States).
Results
Baseline characteristics
The baseline characteristics of included patients.
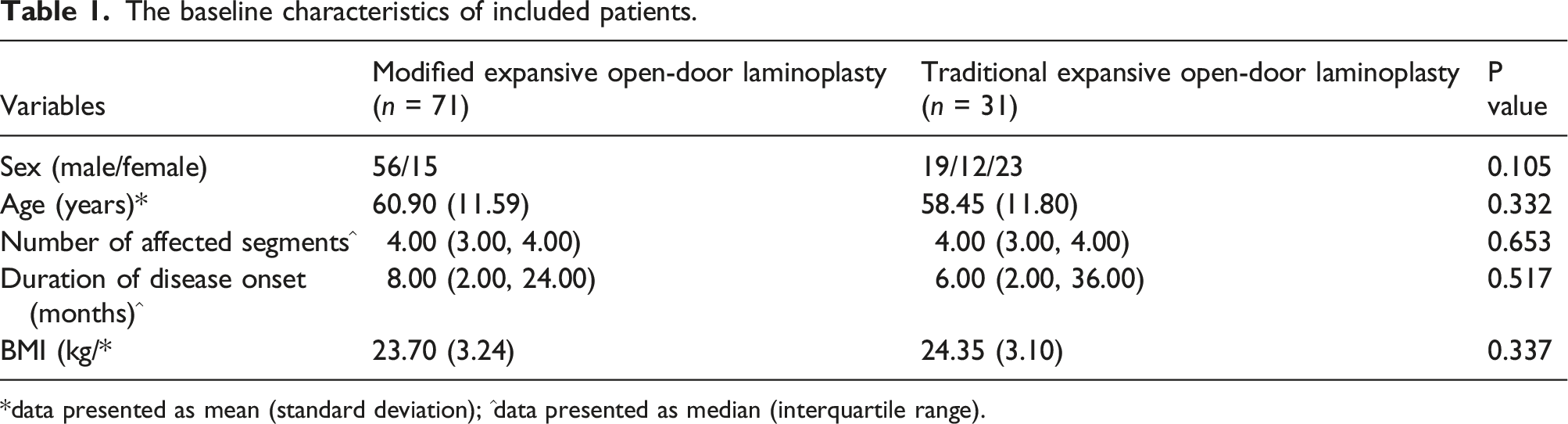
*data presented as mean (standard deviation); ^data presented as median (interquartile range).
Axial symptoms
Axial symptoms between modified and traditional expansive open-door laminoplasty.

^data presented as median (interquartile range).
Clinical outcomes
Intraoperative outcomes between modified and traditional expansive open-door laminoplasty.
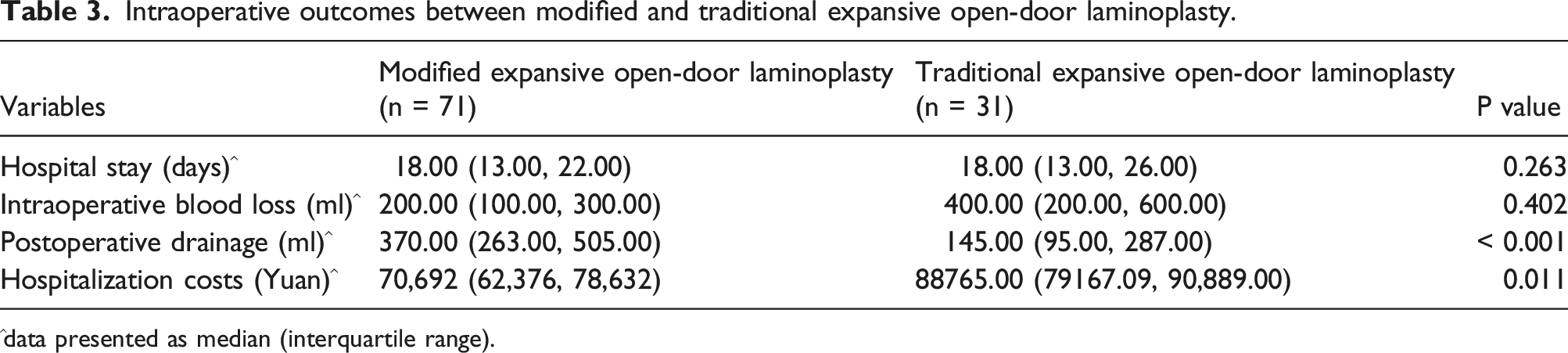
^data presented as median (interquartile range).
Functional outcomes
Surgical outcomes between modified and traditional expansive open-door laminoplasty (data presented as mean [standard deviation]).

Complications
No patients experienced C5 nerve root paralysis, incision infection, or cerebrospinal fluid leakage. The postoperative drainage in modified EOL group was mainly fluid.
Discussion
In this study, patients who underwent modified EOL had a lower risk of axial symptoms than those in the traditional EOL group. Modified EOL was associated with greater postoperative drainage and less cost of hospitalization, while it associated with a significantly improved ROM, mJOA, and Nurick than traditional EOL. Traditional EOL included a single open door cervical canal enlargement at C3-C7, while a C4-C6 single open door cervical canal enlargement was performed with a C3 laminectomy and the preservation of the C7 spinous process during modified EOL. Both procedures allow the cervical spinal cord to drift backwards to relieve anterior compression while directly relieving the posterior compression of the cervical spine.
This study found the incidence of axial symptoms was lower in the modified EOL group, which is consistent with the results of a previous study. 11 The progression of axial symptoms was not related to the improvement of postoperative neurological function. Potential mechanisms for the progression of axial symptoms are injuries to nerves in the neck during surgery, 14 injuries to the posterior cervical muscles during surgery,15,16 disuse atrophy of the neck muscles during postoperative rehabilitation, postoperative changes in ROM of the cervical spine, or changes in the curvature of the cervical spinal cord. An improved EOL method was introduced to improve the progression of axial symptoms. This method consists of a C3-C6 cervical extended-canal plasty with preservation of the C7 spinous process, a C3 laminectomy and C4-C7 laminoplasty, and spinoplasty of the spinal canal with the spinous ligament complex preserved. In this study, modified EOL included a C4-C6 open-door expansive cervical vertebroplasty with a C3 laminectomy and preservation of the C7 spinous process as the cervical semispinalis muscle plays an important role in maintaining the stability of the posterior neck. The C3 single door procedure of traditional EOL was changed to a C3 laminectomy to decompress the cervical spinal cord, avoid the destruction of the cervical semispinalis muscle insertion site on the C2 spinous process and facilitate the field of vision at C4-C6. This method maintains the stability of the muscle group at the posterior part of the neck and the function of neck extension. As the C7 spinous process is attached to the trapezius muscle, rhomboid muscle, superior posterior serratus muscle, splenius capitis muscle, splenius cervicis lampus muscle, cervical ligament, and other muscle and ligament tissues, the preservation of this structure may improve the integrity of the posterior cervical ligament complex.17,18
The length of hospital stay, and intraoperative blood loss were not significantly different between the groups in this study. Patients who underwent modified EOL had significantly more postoperative drainage than those who underwent traditional EOL. Moreover, we noted the cost of hospitalization in patients treated with traditional EOL was more expensive than modified EOL, which could be explained by shortening the number of levels plated from 5 to 3 with significant savings on consumables. In this study, while the postoperative improvement in ROM was significantly greater in the modified EOL group, VAS and NDI were not significantly different between the groups. These findings indicate that both modified and traditional EOL result in similar stability.19–21 Modified EOL may have led to a greater improvement in ROM as this method involved preserving the unilateral paraspinal musculature, reattaching the semispinalis cervicis, and preserving the C7 spinous process. 22
This study is not without limitations. First, as this is a retrospective study, selection and recall biases are inevitable. Second, the analysis based on smaller number of included patients, and conclusions should be verified in further large-scale study. Third, the rehabilitation after surgery were not addressed, which might affect the prognosis of CSM. Fourth, the improvement of the dural sac before and after surgery using MRI were not investigated. Fifth, whether the presence of retraction of C6/7/T1 were not assessed. Last, the surgical outcomes were not compared between patients with specific preoperative characteristics.
Conclusion
Modified EOL is associated with a reduced risk of axial symptoms. Modified EOL is also associated with increased postoperative drainage and less cost of hospitalization. Moreover, the ROM, mJOA score, and Nurick grade showed greater improvement in patients treated with modified EOL. Large-scale, prospective studies are needed to verify the findings of this study and compare the treatment effects of modified and traditional EOL between patients with CSM with specific preoperative characteristics.
Supplemental Material
Supplemental Material - Clinical outcomes of modified versus traditional expansive open-door laminoplasty for cervical spondylotic myelopathy: A single-institution experience
Supplemental Material for Clinical outcomes of modified versus traditional expansive open-door laminoplasty for cervical spondylotic myelopathy: A single-institution experience by Zhitao Shangguan, Gang Chen, Wenge Liu, and Jiandong Li in Journal of Orthopaedic Surgery
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: 5th batch of key discipline construction of Union Hospital affiliated to Fujian Medical University; 07203002.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.