
Abstract
Background
The incidence of chondrosarcoma is increasing every year, and the treatment and prognosis of patients with high-grade chondrosarcoma are becoming more and more important. Nomogram is a tool that can quickly and easily predict the overall survival of tumor patients. Therefore, the development and validation of a nomogram to predict overall survival in patients with high-grade chondrosarcoma was desired.
Methods
We retrospectively collected 396 patients with high-grade chondrosarcoma from the Surveillance, Epidemiology, and End Results (SEER) database from 2004 to 2015. Randomly divided into model and validation groups, the best cut-off values for age and tumor size grouping were derived by using X-tile software. Then, independent prognostic factors for high-grade chondrosarcoma were derived by SPSS.26 univariate and multivariate Cox analyses analysis in the model group, and the model was evaluated by using R software, using C-indix and ROC curves, and finally these independent prognostic factors were included in Nomogram.
Results
396 patients were randomly assigned to the modelling group (n = 280) or the validation group (n = 116). Age, tissue-type, tumor size, AJCC stage, regional expansion and surgery were identified as independent prognostic factors (p < 0.05) which further combined to construct a nomogram. The C-index of internal validation for overall survival(OS) was 0.757, while the C-index of external validation for overall survival(OS) was 0.832. Both internal and external calibration curves show a good agreement between nomogram prediction and actual survival.
Conclusion
In this study, we established age, tumour size, AJCC stage, tissue type, surgery and tumor extension as independent prognostic factors for high-grade chondrosarcoma and constructed a nomogram to predict 3- and 5-year survival rates for high-grade chondrosarcoma.
Introduction
Chondrosarcoma is the second most common histological type of primary bone sarcoma and accounts for 20% of primary bone malignancies.1,2 The estimated annual incidence of chondrosarcoma is 0.5 per 100,000 patients. 3 It was first described in 1939 by Lichtenstein and Jaffe.4,5 The World Health Organization classifies chondrosarcomas as benign, intermediate, or malignant cartilaginous tumors. 6 Conventional chondrosarcomas account for more than 80% of chondrosarcomas and include the central, periosteal, and peripheral subgroups. 7 Chondrosarcomas are a group of different types of malignancies with distinct histopathological features characterized by the production of cartilage matrix. 8
Most chondrosarcomas are slow growing, rarely metastasize, and adequate surgery can lead to a good prognosis. 9 However, because of the poor sensitivity of high-grade chondrosarcoma to radiotherapy and chemotherapy, adequate surgical resection may be the better option. Depending on the pathological lesion, chondrosarcoma splits into central chondrosarcoma in the intramedullary space and peripheral chondrosarcoma on the bone surface. The prognosis of chondrosarcomas is closely related to histological grade. Low-grade chondrosarcomas have abundant cartilage matrix and low cell density, are easily localized and have a good prognosis after surgical resection. However, high-grade tumors have little cartilage matrix, high cell density, and are prone to metastasis, leading to poor prognosis. 2
Many studies have found that age, tumor size, tumor extension and surgery are independent prognostic factors for chondrosarcoma.10–12 Arshi et al. showed that tumor size and surgery were independent prognostic factors for chondrosarcoma of the spine. 13 Chondrosarcoma with metastatic disease has a very poor prognosis. A study by Wang et al. found that tumor grade, tumor size, and surgery were independent factors in the prognosis of patients with chondrosarcoma with metastatic disease. 14
Nomogram is a convenient statistical tool that help to our clinicians, such as predicting outcomes for individual patients.9,15 However, a nomogram has not been used to predict the prognosis of patients with high-grade chondrosarcoma and independent prognostic factors, although it has been shown to have a large number of prognostic factors. Nomogram is a convenient statistical tool that helps clinicians in predicting outcomes for individual patients. In order to use a nomogram, separate scales are first created for each independent prognostic factor using proper statistical tools. Following this, the integer value for each prognostic factor is calculated by matching individual scales to a standard scale (e.g. 0 – 10). All the values are then added to have a total score, which is then matched to the scales of 3-year and 5-year survival rates, again formulated using proper statistical tools. The intersection points of the total score along the survival rate scale provide estimates of survival for each patient.
The Surveillance, Epidemiology and End Results (SEER) database is an extensive and unparalleled database of cancer in the United States. 16 This study aimed at improving the prediction accuracy for prognosis in high-grade chondrosarcomas by formulating and validating the Nomogram for high-grade chondrosarcoma using the basic information of patients obtained from the SEER database.
Methods
Database
Information on 19,201 patients with bone tumors was collected from the SEER database, with inclusion criteria as follows:(1) Patients who were diagnosed with chondrosarcoma between 1975 and 2016; (2)The sixth edition of AJCC staging was adopted; (3)high-grade chondrosarcomas (tumor grade III & IV); Exclusion criteria were: (1) tumour tissue type and tumour size were not clear; (2) tumor grade I or II or unknown grade of tumor; (3)loss to follow-up; (4) unclear data on type of treatment received (surgery, chemotherapy or radiotherapy).
Study population
Finally, 396 patients with high-grade chondrosarcoma from 2004 to 2015 were selected in Figure 1 Flow chart of the research methodology.
Statistical analysis
All of the data in this study were downloaded from SEER*-Stat Software (version 8.3.9).The total number of people were randomly grouped into modelling group(n = 280) and verification group(n = 116) using R software(R Statistical Software Ver 4.0.3). The X-tile program, which was used to determine the optimal threshold for several prognostic factors in a cohort of breast cancer patients, was used to clearly define the optimal threshold for tumor size. 17
Kaplan-meier survival analysis and Cox regression analysis were performed by SPSS software(IBM SPSS Statistics 26).p < 0.05 was considered statistically significant. Kaplan-meier survival analysis and Cox regression analysis were used to analyze patients' age, sex, race, tissue type, tumour size, AJCC (6th edition) TNM staging, surgery, radiotherapy, chemotherapy and tumor extension. OS was regarded as the primary endpoint and was defined as the time in months from diagnosis to death due to any cause. The independent prognostic factors that we established were surgery, tumor size, tumor grade, tissue type, AJCC stage (6th edition)and age while the Tn was not statistically significant in the validation group.
The models were predicted and calibrated with C-index, AUC of ROC and calibration curve, and the modelling group was validated with a validation group.
Results
Patient baseline characteristics
Characteristics of patients with high-grade chondrosarcoma.

In our study, data on 396 patients with high-grade chondrosarcoma were collected including 240 patients (60.6%) with grade III and 156 patients (39.4%) with grade IV. And 396 patients were randomly divided into the modelling group 280 cases (70%) and the validation group 116 cases (30%). We found that the 215 patients with Chondrosarcoma tissue type and NOS accounted for 54.3%. There were 132 patients with Dedifferentiated chondrosarcoma, accounting for 33.3% of the total. 54.0% of high-grade chondrosarcoma patients were in the four limb bones and 38.4% in the trunk bones.As described in other literature,chondrosarcomas in the skull were rare, accounting for 7.6%.There were 385 patients (97.2%) with AJCC stage N stage N0, and most patients chose surgical treatment in 367 patients (92.7%), while most patients did not receive radiotherapy and chemotherapy, accounting for 76.8% and 76.8%, respectively, which is somewhat different from previous literature describing radiotherapy and chemotherapy as independent prognostic factors.
Survival analysis and Validation model
We used X-tile software to determine the optimal cutoff for tumor size and age, as shown in Figure 2. A and B are the best cutoff for the age grouping as determined by the X-tile software, C and D are the best cutoff for it determined tumor size grouping.
In the modelling cohort, we divided the tumor size into three groups, tumour sizes smaller than 71 mm, 72–98 mm, and larger than 99 mm. We divided the age into the following three groups, less than or equal to 49 years old, 50–74 years old, and greater than or equal to 75 years old.
We have analysed all the factors by means of Kaplan-Meier survival analysis and the results are shown in the Figure 3. Indicating that tumour size, AJCC stage (6th edition), tissue type, age, whether surgery was performed, and regional extent were independent prognostic factors for high-grade chondrosarcoma (p < 0.05), while radiotherapy, chemotherapy, and tumour location were not significant. Kaplan-Meier curves for independent prognostic factors in high-grade chondrosarcoma. A-H are the Kaplan-Meier curves of age, AJCC stage (6th edition) TNM, tumour size, tissue-type, surgery and expansion.
Univariate Cox regression analysis in the training group.
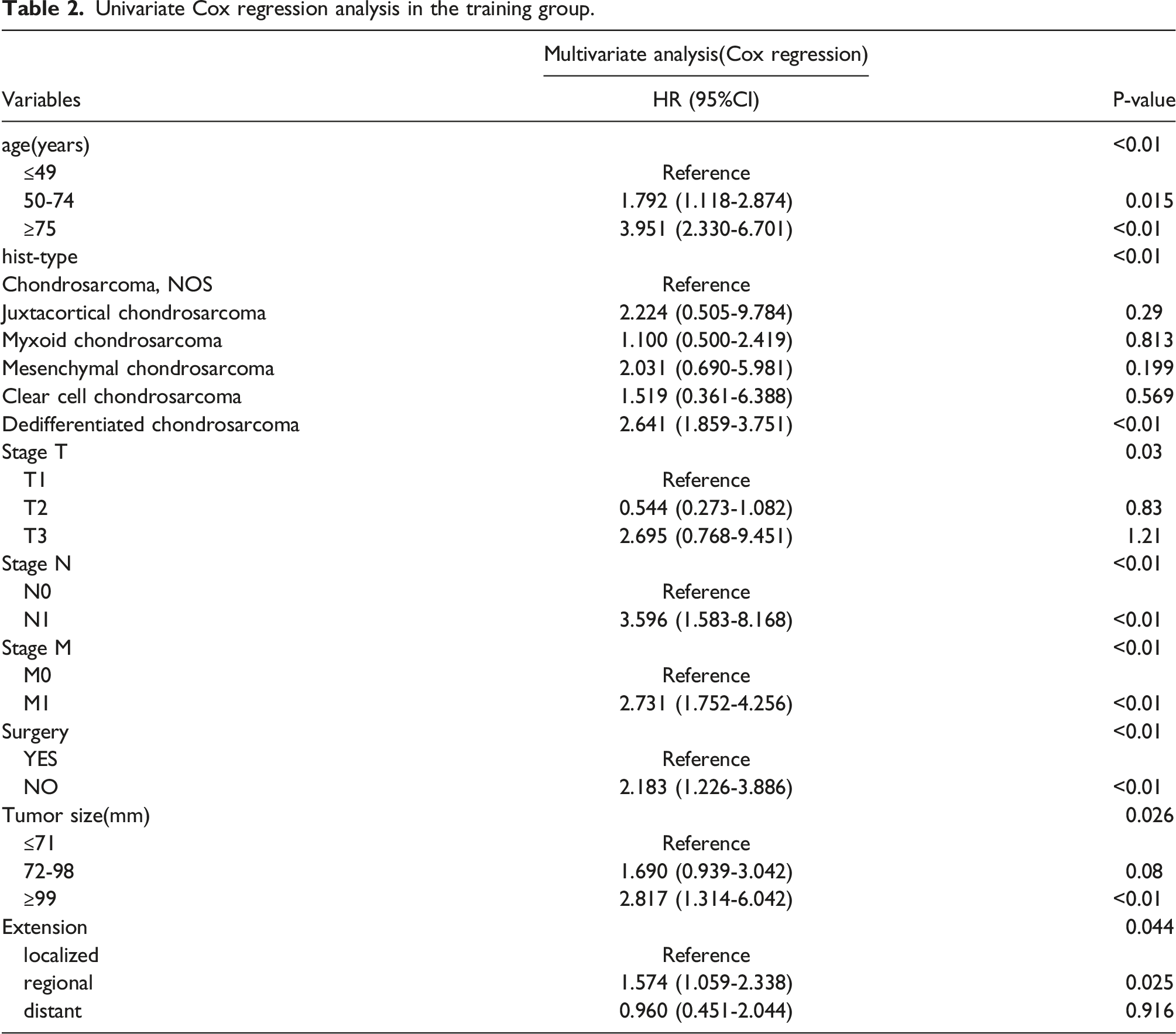
The study showed that age, tissue type, AJCC TNM stage, tumor size, tumor extension, and surgery were independent prognostic factors (p < 0.01).
The predictive ability of the modelling group model was then evaluated by calculating the C-index and calibration curve by R software, and the C-index of the modelling group model was 0.757. For the evaluation model using the c-index, previous studies reported that a c-index of less than 0.7 is of low accuracy, 0.7–0.9 is of moderate accuracy, and greater than 0.9 is of high accuracy.
The calibration curve was shown in Figure 4 (A, B) is the 3-year and 5-year validation curve of the modelling group, (C, D) is the 3-year and 5-year validation curve of the validation group. The dashed line represents an excellent match between the prediction (x-axis) and actual survival results (y-axis).The group was divided into three groups with the same sample size for both internal and external validation.The closer the distance from the point to the dashed line indicates the higher the prediction accuracy.
The calibration curve of the validation group indicates that the model has feasible prediction ability. For the evaluation of the prediction ability of the model, we also conduct the area under the curve (AUC) of the receiver operating characteristic (ROC) for further evaluation. General criteria for AUC (0.5–0.7: low but good for predicting stocks 0.7–0.85: average 0.85 to 0.95: very good 0.95–1: very good but generally unlikely). Our study showed a 3-year AUC index of 0.782 and a 5-year AUC index of 0.779. This indicates that the model in this study is relatively reliable.
The results obtained were shown in Figure 5, which is consistent with the previous evaluation results and proves that our modelling is relatively accurate. A and B are the area under the curve (AUC) of the receiver operating characteristic (ROC) of 3-year and 5-year survival rates.
The production of Nomogram
Finally, by integrating the prognostic factors from the COX analysis into the nomogram, the results were shown in Figure 6. Overall survival nomogram for patients with high-grade chondrosarcomas.
Discussion
Extensive literature have shown that metastasis, tumor grade, and surgery are independent prognostic factors for chondrosarcoma. 18 In addition, other clinical factors are able to influence the patient outcomes, for example, patient age, histological sub-types and so on. However, according to our review of relevant literature, no nomogram has been developed for high-grade chondrosarcoma. Nomograms have been used to predict survival in individual patients by combining all prognostic factors and calculating cumulative effects to predict three-year and five-year survival rate. We developed comprehensive nomograms from the data obtained in the SEER database to predict three-year and five-year OS rates in patients with high-grade chondrosarcoma.
For the independent prognostic factors of high-grade chondrosarcoma, survival analysis was performed using SPSS software, and it was concluded that tumor size, age, tissue type, AJCC stage, tumor extension, and surgery were independent prognostic factors. However, in the validation group, AJCC staging N stage did not show variability.We speculate that this may be due to the relatively small number of cases.The other independent prognostic factors were significant (p < 0.05). We found that the majority of patients were aged 50–75 years (50.5%), and there is some controversy about sex influence on the prognosis of high-grade chondrosarcoma.19,20
In this study, the sex ratio was approximately 1.62:1.We did not include gender as an independent prognostic factor. Therefore, whether gender is an independent prognostic factor remains to be further investigated.
Previous studies of chondrosarcoma have shown that anatomical location, tumour size and stage can be independent prognostic factors for patients with chondrosarcoma.21,22 Similar to these literature, we demonstrate that tumour size and AJCC stage (6th edition) are independent prognostic factors for high-grade chondrosarcoma.Regarding anatomical location, we found that chondrosarcomas in 214 patients (54%) were in the limbs, 152 patients (38.4%) were in the skull, and only 30 patients (7.6%) were in the trunk. 23 However, we couldn’t confirm anatomical position as independent prognostic factors for high grade chondrosarcoma, this does not agree with that of other literature, 24 Whether anatomic location is an independent prognostic factor for high-grade chondrosarcoma needs further study.
Tissue type has always been an important factor of disease, and Chondrosarcoma is no exception. Our study showed that the histological type of chondrosarcoma was NOS in 215 (54.3%) patients.There were 132 patients (33.3%) with Dedifferentiated chondrosarcoma. In our study, tissue type was identified as an independent prognostic factor for high-grade chondrosarcoma. In the multivariate cox analysis, the significance of Dedifferentiated chondrosarcoma was p < 0.01, which was consistent with the previous reports of related literature.
Surgery has been the main treatment for chondrosarcoma. Our study showed that 362 patients (96.7%) underwent surgical treatment, and the significance of univariate survival analysis was p < 0.01, which was similar to the results reported in other literature.
Radiotherapy and chemotherapy were not established as independent prognostic factors for high-grade chondrosarcoma, and Wagner, M. J et al. also failed to establish radiotherapy and chemotherapy as independent prognostic factors.16,25 Gao Z et al., established adjuvant radiotherapy as an independent influencing factor in their study whether radiotherapy and chemotherapy can predict the prognosis of high-grade chondrosarcoma needs further study.26–29 Chen et al.found that radiotherapy was worse for low-grade chondrosarcoma patients and had a better trend for high-grade chondrosarcoma patients. 28 In their study of high-grade chondrosarcoma, age of diagnosis, pathological grade, tissue grade, tissue type, SEER stage, tumor size, and surgical resection were identified as independent prognostic factors, 26 similar to our study, indicating the reliability of our study.
Moreover, the case age at diagnosis update included in our study is more reliable for predicting the prognosis of high-grade chondrosarcoma. In study of Song K, Lin K, Kang H,et al.,they collected information on 450 patients with spinal chondrosarcoma from the SEER database and were used using Univariate log-rank and multivariate Cox analysis to identify age, histological subtype, grade, tumor size, stage and surgical status as independent prognostic factors for spinal chondrosarcoma.
Finally, there are some limitations in this study. 1. The number of cases screened in this study is relatively small, which may affect the accuracy of the predicted results to some extent. 2. This study excluded all patients with unclear information (such as AJCC staging, tumor size, chemotherapy, surgery, etc.). If this nomogram is to be used, the relevant information of the patients must be clear.
Conclusion
In this study, we established age, tumour size, AJCC stage, tissue type, surgery and tumor extension as independent prognostic factors for high-grade chondrosarcoma and constructed a nomogram to predict 3- and 5-year survival rates for high-grade chondrosarcoma. Having nomograms can make us faster and more convenient patient survival analysis and prognosis, which is of great help to our clinicians.
Footnotes
Author contributions
(I) Conception and design: Y Sun, Y Li, G Gao; (II) Administrative support:G Gao,L Nong; (III) Provision of study materials or patients: Y Sun,C Ouyang; (IV) Collection and assembly of data: Y Sun,C Ouyang,M Jiang; (V) Data analysis and interpretation: Y Sun, Y Zhang; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Ethical approval
The SEER program database is publicly available and contains no unique identification for patients such as name, date of birth, or Social Security number. Analysis of the deidentified data from the Surveillance, Epidemiology, and End Results (SEER) program was exempt from medical ethics review. All procedures performed in studies involving human participants were in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study. The authors affirm that human research participants provided informed consent for publication of the images in Figure(s) 1, 2, 3, 4, 5 and 6.