
Abstract
Background
This study aimed to determine the prevalence and risk factors of anxiety and depression among orthopaedic oncology patients, their quality of life and coping strategies.
Methods
This cross-sectional study recruited patients from the outpatient orthopaedic oncology clinic at a tertiary institution. Data were collected from self-report questionnaires: Hospital Anxiety and Depression Scale Hospital Anxiety Depression Scale, World Health Organization Quality of Life (WHOQOL-BREF) and Brief Coping with Problems Experienced (Brief COPE). Risk factors were analyzed with multiple logistic regression.
Results
191 patients were recruited. The median age was 39.4 years old (IQR 35.0). 29.8% had anxiety, 16.2% had depression, and 15.2% had mixed anxiety and depression. Quality of life median scores differed significantly between patients with anxiety and no anxiety and patients with depression and no depression (p < 0.001). Patients with mixed anxiety and depression had a more inferior quality of life (p < 0.001). Age, psychological health and radiotherapy were inversely associated with anxiety. Physical and psychological health were significantly associated with less depression. Ongoing chemotherapy was significantly associated with anxiety and depression. The commonest coping strategies were denial, behavioural disengagement, venting and self-blame.
Conclusion
Anxiety and depression are prevalent among orthopaedic oncology patients. Patients with mixed anxiety and depression had a more inferior quality of life. Patients with ongoing chemotherapy had higher risks of anxiety and depression. The commonest coping strategies were denial, behavioural disengagement, venting and self-blame. Psychosocial evaluation followed by appropriate psychiatric referrals and consultations could be established to facilitate orthopaedic oncology patients during their course of treatment.
Introduction
Cancer patients often experience various psychological distresses, resulting from the emotional stress of living with the illness and the course of treatment, disease progression, fear of recurrence and hindrance to daily living due to physical limitations. 1 A large-scale study involving 4500 cancer patients documented a prevalence of psychological distress ranging from 29% to 43%. 2
Anxiety and depression affect the quality of life, treatment adherence, disease progression and pain tolerance. Age, sex, cancer type, metastasis and ongoing treatment are common risk factors associated with psychological problems.3,4
As the disease progresses, the quality of life worsens significantly. 5 Felder-Puig et al. showed a lower frequency of marriage, more unsatisfactory academic performance in school and lower employment status among cancer patients. 6
Coping involves an individual’s cognitive and behavioural attempts to manage a stressor. 7 Coping with cancer requires more skills, enabling patients to adjust their emotions to life-changing diagnoses and long-term complications. 8
Numerous studies have demonstrated tremendous deterioration in psychological health amongst breast, prostate, lung, head and neck cancer patients.2,9-11 To date, there was scarce literature on psychological distress among orthopaedic oncology patients. This study was carried out to determine the prevalence of anxiety and depression amongst these patients, including the risk factors, quality of life and coping strategies.
Methods
We conducted a prospective cross-sectional study involving orthopaedic oncology patients who attended the outpatient clinic in a single tertiary institution from June 2015 to May 2016. By considering 95% as the power of the study, an absolute significance level set at 5% and estimated proportion of psychological distress among cancer patients of 0.11, 12 the minimum sample size required was 180 participants including 20% drop out rate. Inclusion criteria were (1) female and male gender; (2) aged between 18 and 65 years old; and (3) malignant and locally aggressive benign tumours. The study excluded new referrals and patients with dementia, mental retardation, prior psychiatric illnesses, or severe medical illnesses. Ethical approval was obtained (MECID NO: 201,411–774).
In the orthopaedic oncology outpatient clinic, there were patients with various diagnoses, that is, benign or malignant primary soft tissue tumours, benign or malignant primary bone tumours, skeletal metastases and tumour-like conditions. Therefore, purposive sampling with a homogenous sampling method was employed to include eligible respondents in this study. The respondents were screened according to age and type of tumour by referring to the outpatient cards on the day of follow-up. Informed consent was obtained.
The study protocol comprised of four sections in a structured questionnaire: (A) Socio-demographic and clinical data; (B) Hospital Anxiety Depression Scale (HADS); (C) World Health Organization Quality of Life- Brief version (WHOQOL-BREF) and (D) the Brief Coping with Problems Experienced (Brief COPE).
Socio-demographic data included age, gender, ethnicity, marital status, education level, occupation and presence of family support. Clinical data collected comprised of type and site of cancer, duration of illness, staging, metastasis, recurrence, numbers of surgery and treatment modalities.
The Hospital Anxiety Depression Scale (HADS) is a brief questionnaire specifically designed to screen for anxiety and depression. It has 14 items with responses scored on a scale of 0–3 (3 indicates higher symptoms frequencies). It is subdivided into anxiety subscale (HADS-A) and depression subscale (HADS-D), containing seven items. Scores for each subgroup (anxiety and depression) range from 0 to 21, with scores categorized as normal 0–7; or abnormal 8–21. Scores for the entire scale range from 0 to 42, with higher scores indicating more distress. 13
WHOQOL-BREF consists of 26 items and examines four domains on quality of life (QOL). The domains are physical health (7 items), psychological health (6 items), social relationships (3 items) and environment (8 items). Items are rated on a 5-point Likert scale in which the lowest score is one, and the highest score is 5. The domain scores are scaled positively; that is, higher scores denote a higher quality of life. Three items are compulsory to be reversed before scoring, namely, items 3, 4 and 26. The transformed score for each domain is derived from the summation of raw scores. 14
The Brief COPE is designed to examine various coping strategies used by respondents in response to stress. The Brief COPE comprises 14 scales, which assess the degree to which a respondent utilizes a specific coping strategy. Each scale has two items, with total scores ranging from 2 (minimum) to 8 (maximum). Higher scores denote higher utilization of the specific coping strategy. The total score on each scale is derived from the summation of its items. No reverse scoring is required. These scales include active coping, planning, positive reframing, acceptance, humour, religion, emotional support, instrumental support, self-distraction, denial, venting, substance use, behavioural disengagement and self-blame. Respondents rated on a 4-point Likert scale ranging from 1 ‘I have n't been doing this at all’ to 4 ‘I 've been doing this a lot’. 15 All three questionnaires have been validated.13-15
During clinic follow-ups, respondents were first interviewed on socio-demographic characteristics. Clinical information was obtained from case notes. The HADS, WHOQOL-BREF and Brief COPE were self-administered by patients in the presence of the primary investigator.
Data analysis was performed using the Statistical Package for the Social Sciences (SPSS) version 22.0 (SPSS, Inc., Chicago, IL, USA). An independent t-test was used to examine the mean difference in the quality of life score. Simple logistic regression was first conducted to screen important independent variables for the multivariate analysis to analyze the association between socio-demographic data, clinical factors and quality of life domains with psychological disorders. From the simple logistic regression results, independent variables with a p-value <0.25 were included in the stepwise multiple logistic regression analysis. Statistical significance was set at 0.05.
Results
Socio-demographic and clinical characteristics
Socio-demographic characteristics of orthopaedic oncology patients (N = 191).

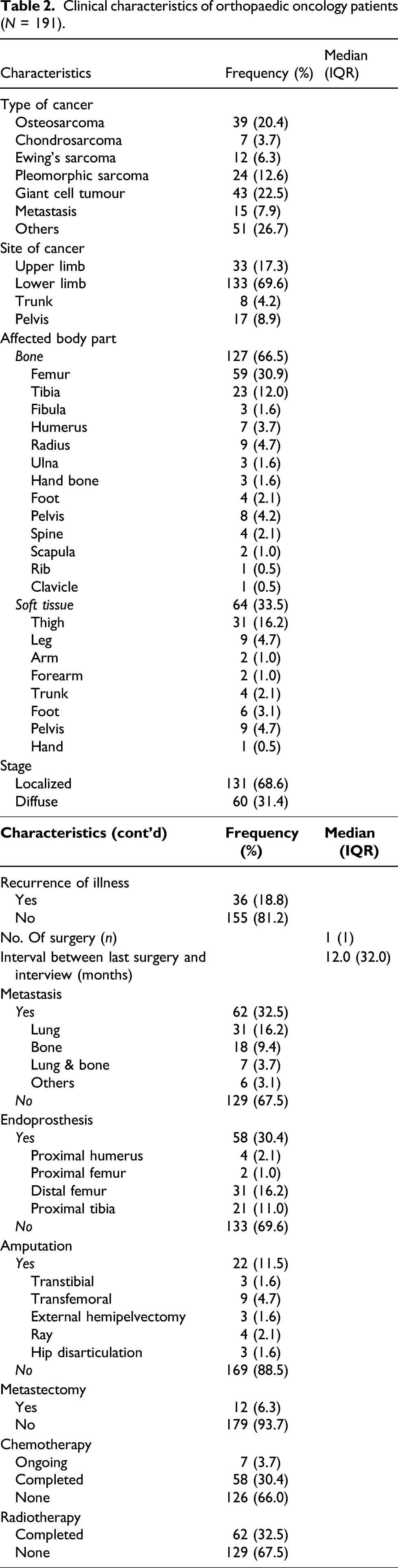
Clinical characteristics of orthopaedic oncology patients (N = 191).
Prevalence of psychological disorders
The prevalence of anxiety and depression in this cohort was 29.8% and 16.2%, respectively. 15.2% of patients had mixed anxiety and depression.
Quality of life
Quality of life median scores for each domain were significantly different between patients with and without psychological disorders (p < 0.001). The median score difference (difference of 6 scores) for anxiety was higher for physical and psychological health domains. For depression, a higher median score difference was observed in psychological (7 scores), physical and environmental (6 scores) domains.
Differences in quality of life domain scores between orthopaedic oncology patients with anxiety disorder and mixed anxiety and depression (N = 57).

*Mann–Whitney U test, significance level at p < 0.05.
Association of socio-demographic and clinical factors with anxiety disorder
Factors associated with anxiety disorder among orthopaedic oncology patients.

1Simple logistic regression.
2Multiple logistic regression.
The model reasonably fits well. Model assumptions are met. No interaction and multicollinearity problem was detected.
Association of socio-demographic and clinical factors with depression disorder

Factors associated with depression disorder among orthopaedic oncology patients.

1Simple logistic regression.
2Multiple logistic regression.
The model reasonably fits well. Model assumptions are met. No interaction and multicollinearity problem was detected.
Brief Cope with Problems Experienced (COPE) inventory scales
Differences in Brief Cope with Problems Experienced (COPE) inventory scales between orthopaedic oncology patients with psychological disorder and no psychological disorder (N = 191).
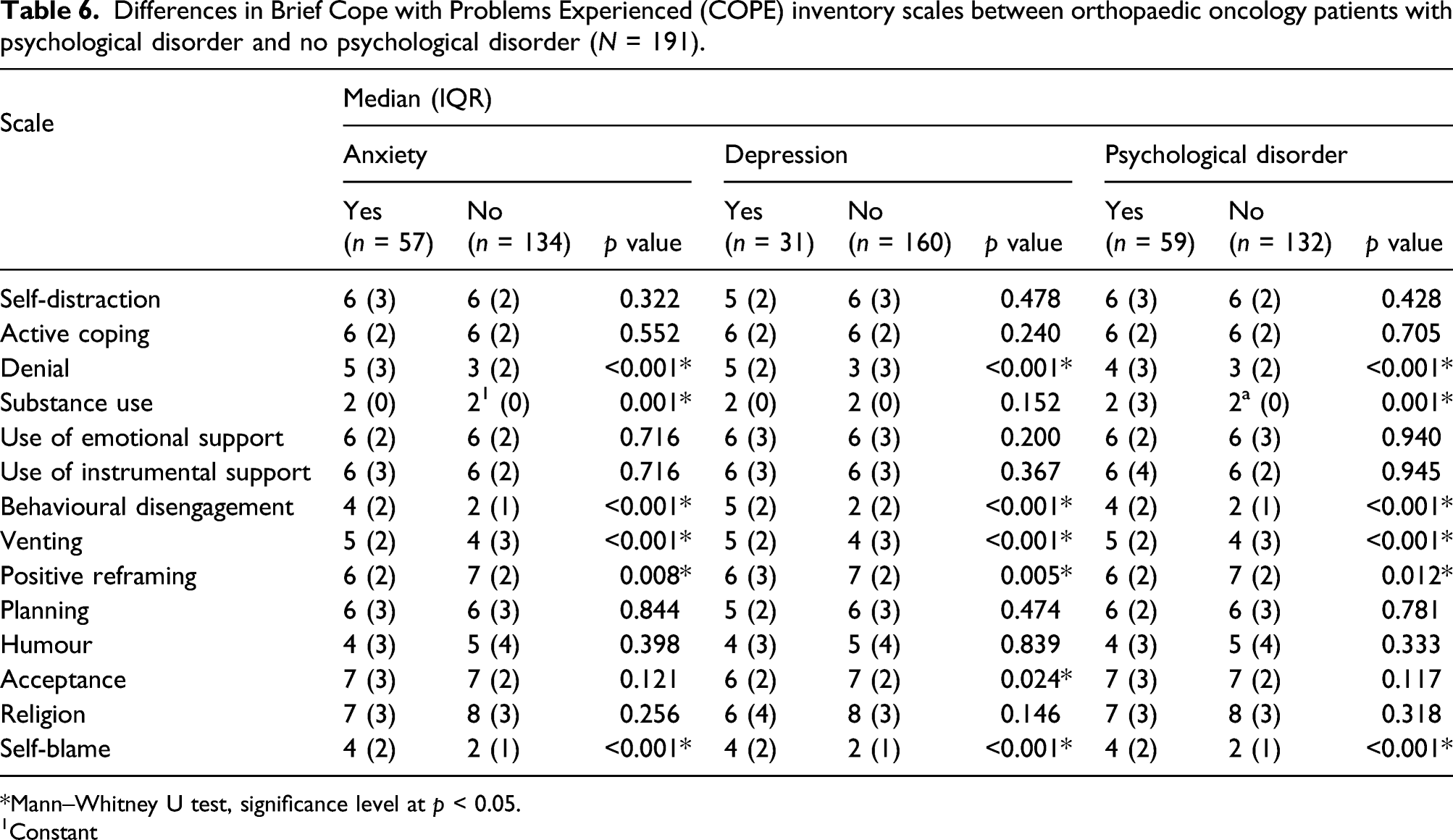
*Mann–Whitney U test, significance level at p < 0.05.
1Constant
Differences in Brief Cope with Problems Experienced (COPE) inventory scales between orthopaedic oncology patients with anxiety disorder and both anxiety and depression (N = 57).

*Mann–Whitney U test, significance level at p < 0.05.
Discussion
The prevalence of anxiety and depression is 29.8% and 16.2%, respectively. Derogatis et al. examined 215 newly admitted cancer patients and found that 18% had depression while 7% had anxiety. 16 The prevalence of anxiety in our sample was four times higher despite the respondents being outpatients who were supposed to have lower anxiety tendencies than the newly warded patients, as in Derogatis’ study. This is similar to a report by Ng et al., who reported the prevalence of depression as 10.8%.12. However, the prevalence in our study was still higher than other studies using HADS, which were 16%–23% for anxiety and 9%–12.5% for depression.17-19
This considerable high prevalence could be due to the substantial loss of mobility or appearance-related changes caused by the disease progression or surgery. Most cancer treatments can cause moderate to severe disfigurement. Changes in physical appearance can have detrimental impacts on emotional, social and economic aspects of the patients’ lives. They also portray as a constant reminder of the disease. Looking visibly different from other members of the society causes them to have lower self-esteem, raised the level of anxiety or depression, difficulty in social interactions and social withdrawal.20,21 Physical disability and disfigurement suffered by patients may hamper them from indulging in physical activities, thus contributing to psychological disorders. 22 Furthermore, fear of a potential amputation in the treatment process will add more emotional distress to the patient.
The prevalence of mixed anxiety and depression was 15.2% in our study. Mixed anxiety and depression are more prevalent in the stomach, pancreatic, head and neck, and lung cancers but less common in breast cancers. 23
Age was inversely correlated to anxiety in our study. Younger patients tend to have more emotional problems, probably due to insecurities and interruptions in active daily living. Older patients have more life experiences and are more willing to accept physical impairments. They are generally more prepared to accept illnesses and adhere to treatment.11,24,25 In clinical practice; this highlights the importance of identifying psychological problems among younger patients.
Linden et al. found that females were two times more prone to psychological distress. 11 Females are found to favour spiritual practices and religious coping. 26 Men may initially perceive cancer as a less threatening event. 11 Another study reported otherwise; men were more emotionally distressed because men do not use the social support they received as effectively as females. 27 Based on our findings, gender is not an absolute risk factor for psychological disorders.
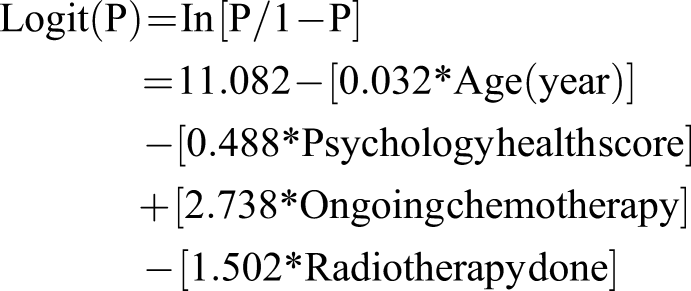
Ongoing chemotherapy was a risk factor for both anxiety and depression. Our findings were consistent with what is reported in other studies.28-30 During chemotherapy, patients experience substantial emotional disturbances due to the adverse effects of chemotherapy, such as hair loss, uncertainties about the effectiveness of treatment, and concurrent psychosocial problems. 31
The median scores for all domains of quality of life were significantly lower in patients with emotional distress. Those with mixed anxiety and depression had an even lower rate of life scores. Although most patients could function normally, return to work and live relatively symptom-free lives, musculoskeletal tumours and treatment can result in physical and psychological problems. This affects patients’ quality of life and, in return, results in higher levels of emotional distress, which is perpetuated in a vicious cycle. This study shows that psychological health is significantly associated with anxiety, while physical health and psychological health is significantly associated with depression.
Denial, behavioural disengagement, venting, acceptance and self-blame were common coping strategies in our study. Our findings were consistent with a study conducted to examine the coping strategies among 141 breast cancer patients who underwent outpatient chemotherapy. 32
To the best of our knowledge, there are limited related studies on orthopaedic oncology patients. Paredes et al. studied the trends of emotional distress of 36 sarcoma patients from diagnostic to treatment phases and their coping mechanisms. The authors reported 25% and 11.1% of patients had clinical anxiety and depression. 33 Tang et al. reported that approximately 30% of 76 patients with extremity sarcoma had anxiety with or without depression, leading to inferior physical function, quality of life and pain. 34 However, these studies had a smaller sample size. These studies only reported on one or two aspects; for instance, a report by Paredes et al. only encompassed the prevalence of psychological distress and coping strategies while Tang et al. only on prevalence and quality of life. This current study reported on most psychological distress among patients, associated risk factors, their quality of life and coping strategies.
However, there are several limitations. This study was conducted among outpatients in a single institution. The findings may differ if both outpatients and inpatients were included. A non-randomized sampling method was utilized due to the strict criteria in respondent recruitment. The cross-sectional study design offered information only at one point in time; therefore, the findings only reflect the patient’s psychological state on the day of the interview. A longitudinal cohort study on the trends of psychiatric distress during treatment may provide more information. The questionnaires used were self-reported. Although respondents may try their best to be truthful, answers given may be exaggerated and largely depends on the patients’ mood during the interview. Usage of more structured interview such as Structured Clinical Interview for DSM Disorders (SCID) may prevent this issue. The consumption of antidepressant or anxiolytic drugs among patients were not investigated in this study.
Conclusion
Anxiety and depression are prevalent among orthopaedic oncology patients. Patients with mixed anxiety and depression have a more inferior quality of life. Age, psychological health score, chemotherapy and radiotherapy are potential risk factors. Denial, behavioural disengagement, venting, acceptance and self-blame were common coping strategies used. The awareness of high prevalence of anxiety and depression among orthopaedic oncology patients should be raised among healthcare providers. Psychosocial evaluation of orthopaedic oncology patients and assessment of potential risk factors should therefore be done on a routine basis. Appropriate psychiatric referrals and consultations could be established to facilitate patients during their treatment course.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.