
Abstract
Objective
The study aim was to examine the effect of a psychological intervention on patients with psoriasis vulgaris.
Methods
Participants in this prospective study were 205 patients with psoriasis vulgaris, 104 who received a psychological intervention (study group) and 101 who received routine nursing care (control group). An additional 291 healthy subjects formed a non-psoriasis group. The Symptom Checklist-90 (SCL-90), Generic Quality of Life Inventory (GQOLI), Self-Rating Depression Scale (SDS) and Self-Rating Anxiety Scale (SAS) were used to evaluate psychological status and quality of life.
Results
There were significant differences in SCL-90 and GQOLI scores between the study and non-psoriasis groups. After treatment, the study group showed significantly improved scores on the SCL-90 and GQOLI compared with the control group. Scores on the SDS (mean ± standard deviation: 31.99 ± 4.54 vs. 44.08 ± 4.52) and SAS (28.36 ± 4.52 vs. 40.14 ± 6.33) were improved in the study group. In addition, patients in the study group showed higher satisfaction rate and compliance rate than those in the control group.
Conclusion
Psychological intervention may be beneficial for improving quality of life and the therapeutic efficacy of drugs in patients with psoriasis.
Introduction
Psoriasis is a common inflammatory skin disease with an incidence of 0.12% in China. 1 Most patients with psoriasis (approximately 60%) are diagnosed between the ages of 20 to 30 years. 2 Owing to cosmetic disfigurement, the chronic nature of the disease and the high incidence of relapse, patients with psoriasis are susceptible to depression and suicidality. 3 The psychological status of patients has an effect on the progression and prognosis of psoriasis. 4 , 5 Therefore, psychological intervention may be beneficial in the management of psoriasis.
In this study, we investigated the efficacy of psychological intervention after drug treatment for patients with psoriasis vulgaris. We aimed to determine whether such an intervention could improve the life of patients with psoriasis vulgaris.
Patients and methods
Patients
We enrolled inpatients with psoriasis who had been admitted to the Department of Dermatology of the Second Affiliated Hospital of Xi’an Jiaotong University from March 2013 to August 2017. Written informed consent for research was obtained from each patient, and the study was approved in November 2012 by the institutional human experiment and ethics board of the Second Affiliated Hospital of Xi’an Jiaotong University (No. 2012-453, Xi’an, Shaanxi Province, China). Psoriasis was diagnosed based on the criteria of psoriasis vulgaris. 6 Patients with other skin disorders were excluded from the study. All intervention group patients (study group) received a course of narrow-band ultraviolet B phototherapy (10 times, a single dose of 0.3–0.5 J/cm2 once every 2 days). They were orally given Xiaoyin Granules (Shaanxi Kanghui Pharmaceutical Co. Ltd., Shaanxi Province, China). All patients’ Psoriasis Area and Severity Index scores were recorded before and after treatment. We also enrolled a group of healthy subjects as non-psoriasis controls (non-psoriasis group).
Control group
The psoriasis control group received regular nursing and were advised to consume high-calorie, high-protein diets and to avoid allergy-inducing food.
Study group
The study group received a series of patient intervention programs, which are summarized as follows. First, patients’ misperceptions about psoriasis were eliminated by effective communication between patients and doctors via a science lecture. Second, patients were encouraged to participate in physical activities such as exercise, sports, games and dance for 1 hour every day. The exercises involved muscle relaxation, which helps to relieve stress and anxiety. Third, patients communicated with each other to help mitigate their loneliness. Finally, patients received encouragement that enabled them to obtain substantial family and social support, such as emotional support and language support, to help them to overcome their feelings of inferiority.
Observations
Psychological status was rated using the Symptom Checklist-90 (SCL-90), the Self-Rating Depression Scale (SDS) and the Self-Rating Anxiety Scale (SAS). The Generic Quality of Life Inventory (GQOLI) was used to evaluate quality of life. The SCL-90 7 consists of 90 items that measure a wide range of psychiatric symptomatology related to feelings, emotions, thoughts, consciousness, behaviour, living habits, interpersonal relationships and sleep. There are ten factors, or psychological symptom dimensions. Responses are scored in terms of the number of positive items on the primary dimensions (with scores not less than 2) and scores on each factor are calculated. A large number of positive items is associated with a higher score on each factor; higher scores indicate worse psychological health. Scores greater than 2 (beyond the normal average score) for a particular item suggest psychological problems in that area. The 74 GQOLI 8 items assess physical, psychological, social and material indicators. The first three indicators contain five factors each and the material indicator contains four factors. Together with an overall quality of life factor, there are 20 factors in total. Higher scores on this scale indicate better quality of life. The SAS 9 comprises 20 questions scored on a Likert scale of 1 to 4 (none or a little of the time, some of the time, a good part of the time and most of the time). Higher scores correspond to higher anxiety levels. The SDS 10 comprises 20 items scored on a Likert scale ranging from 1 to 4 (a little of the time, some of the time, a good part of the time and most of the time). Scores greater than 50 indicate depression; higher scores represent more severe depression.
The SCL-90, GQOLI, SAS and SDS instruments were scored by 11 nurses and doctors (trained in the use of these instruments) at 1 week before medical and intervention treatment and 1 month after medical and intervention treatment. The mean length of hospitalization was recorded. Degree of patient satisfaction was scored using Likert scales ranging from 1 to 5 (1 = very unsatisfactory; 2 = unsatisfactory; 3 = moderate; 4 = satisfactory; 5 = very satisfactory).
Statistical analysis
Data analysis was performed using SPSS Statistics for Windows, Version 17.0 (SPSS Inc., Chicago, IL, USA). Student’s t-tests and the chi-square tests were used to compare SCL-90, GQOLI, SAS and SDS scores, hospitalization length and patient satisfaction between the different groups. Statistical significance was set at P < 0.05.
Results
Study subjects
A total of 205 inpatients with psoriasis were enrolled in the study (Figure 1). This cohort of patients consisted of 131 men and 74 women, with a mean age of 30.3 ± a standard deviation of 7.24 years (range, 16–65 years). The mean time from diagnosis to treatment initiation was 2.5 years (range, 0.5–29 years). Sixteen patients had a family history of psoriasis. The study group contained 104 patients and the control group comprised 101 patients. The non-psoriasis group comprised 291 healthy subjects (212 men and 79 women), with a mean age of 29 ± 6 years (range, 20–50 years).

Flow diagram of participants.
SCL-90 scores
There were no significant differences between the study and psoriasis control groups on gender, age, disease severity, education and drug response. Compared with the non-psoriasis group, the study group showed higher baseline scores on depression, anxiety, obsessive–compulsive, somatization, interpersonal relationships, horror and interpersonal sensitivity (P < 0.05; Table 1). However, there was no between-group difference in paranoid ideation and psychoticism scores. Psychological intervention led to a reduction in the scores on depression, anxiety, obsessive–compulsive, somatization, interpersonal relationships, horror and interpersonal sensitivity in patients with psoriasis (P < 0.05; Table 2).
Comparison of SCL-90 score distributions in the non-psoriasis and study groups (means ± standard deviations).

SCL-90, Symptom Checklist-90
Comparison of SCL-90 score distributions in the study and psoriasis control groups (means ± standard deviations).

SCL-90, Symptom Checklist-90
GQOLI scores
Patients with psoriasis and healthy subjects showed significant differences in somatic health, mental health, social function, material life, economic status and community service (P < 0.05; Table 3). After psychological intervention, these parameters were significantly improved (P < 0.05).
Group comparisons of GQOLI score distributions (means ± standard deviations).

aSomatic health, Mental health, Social functioning and Material life are GQOLI dimensions; data in these rows show subtotal scores for these dimension (the overall quality of life factor subtotal is not shown in this table). *P < 0.05 vs. the non-psoriasis group; △P < 0.05 vs. the psoriasis control group.
GQOLI: Generic Quality of Life Inventory.
SDS and SAS scores
At the time of hospitalization, patients in the study and psoriasis control groups showed comparable SDS and SAS scores (Table 4). Interestingly, after the psychological intervention, scores on both the SDS (31.99 ± 4.54 vs. 44.08 ± 4.52) and SAS (28.36 ± 4.52 vs. 40.14 ± 6.33) had decreased in the study group relative to the psoriasis control group (P < 0.01).
Group comparisons of SDS and SAS score distributions (means ± standard deviations).
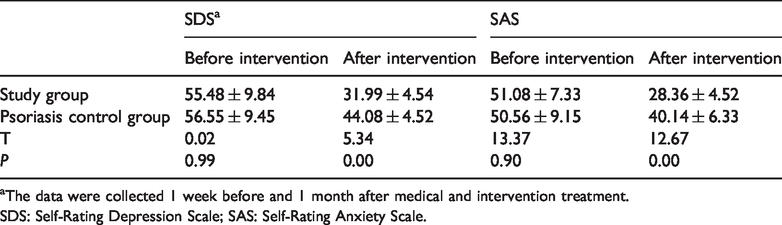
aThe data were collected 1 week before and 1 month after medical and intervention treatment.
SDS: Self-Rating Depression Scale; SAS: Self-Rating Anxiety Scale.
Hospitalization length and patient satisfaction
There were significant differences between the study and psoriasis control groups in hospitalization length, satisfaction rate and compliance rate (P < 0.05; Table 5).
Group comparisons of hospitalization length, patient satisfaction rate and compliance rate (means ± standard deviations).

*P < 0.05.
Discussion
Psoriasis is a persistent skin disease. Although it is not usually a life-threatening disorder, psoriasis can have a serious effect on psychological health. No effective prophylactic approaches are currently available for this disease. The use of psychological interventions for patients with psoriasis is receiving greater attention. There may be a link between psychological status and progression of psoriasis. 11 , 12 The quality of life of patients with psoriasis is affected by depression, 11 and patients often have very little knowledge about the disease. 13 Additionally, global scores on the SCL-90 are substantially higher in patients with psoriasis than in healthy controls. 7 Consistently, our data demonstrated that compared with non-psoriasis subjects, patients with psoriasis scored higher on several SCL-90 items, including depression, anxiety, obsessive–compulsive, somatization, interpersonal relationships, horror and interpersonal sensitivity. After psychological intervention, SCL-90 scores improved in patients with psoriasis. Moreover, the quality of life of patients with psoriasis, particularly regarding sleep, self-respect and learning, was improved by the psychological intervention.
Depression and anxiety may affect the immune system and consequently aggravate skin diseases. Therapy compliance and efficacy can be enhanced by psychological intervention. Therefore, it is important to resolve both somatic and psychological symptoms in patients with psoriasis. Anxiety is associated with skin injury in 40% of patients with psoriasis, and psychological intervention can help to reduce skin damage. 14 , 15 Abnormal emotion elicits the release of substance P and the proliferation of keratinocytes, which may contribute to the emergence of psoriasis. 16 The present findings show that after psychological intervention, the primary outcomes of anxiety and depression scores of study group patients were remarkably improved compared with psoriasis control group patient scores.
Our data also demonstrated a reduction in hospitalization length and an increase in patient satisfaction in the study group compared with the psoriasis control group. These were secondary outcomes. Our results suggest that psychological intervention accelerates the recovery of skin lesions. Therefore, psychological intervention could play an important role in treating psoriasis. However, the small sample size may have affected the statistical significance. Further clinical studies with large samples are needed to confirm the effectiveness of this type of psychological intervention for psoriasis.
Conclusions
Our data suggest that psychological intervention can increase the therapeutic efficacy of drugs and improve the quality of life of patients with psoriasis.