
Abstract
Objective
Children with acute lymphoblastic leukemia (ALL) may be at increased risk of psychiatric disorders. This study analyzed the incidence of psychiatric disorders in children with ALL in South Korea.
Methods
Using nationwide claims data for January 2009 to March 2016, we identified three major psychiatric disorders (depression, anxiety and stress/adjustment disorder) among children diagnosed with ALL. We analyzed the incidence of psychiatric disorders before and after ALL diagnosis.
Results
Overall, 2160 children diagnosed with ALL were identified. Seventy-five children (3.5%) were diagnosed with at least one major psychiatric disorder from 1 year before ALL diagnosis to the last follow-up point (range: 42.5–111.5 months). Of these, 70 (93.3%) patients were identified after ALL diagnosis, with the incidence peaking 1 year after ALL diagnosis. Depression, anxiety and stress/adjustment disorders were diagnosed in 30 (1.4%), 15 (0.7%) and 30 (1.4%) patients, respectively.
Conclusions
Among pediatric patients with ALL, most psychiatric disorders were identified after the diagnosis of leukemia, and psychiatric disorder incidence differed according to patient age and time since ALL diagnosis. Timely screening for and proper management of mental disorders are needed during all stages of ALL treatment.
Keywords
Introduction
Acute lymphoblastic leukemia (ALL) is the most common childhood and adolescent cancer, accounting for 25% of all cases. 1 The survival rate of pediatric ALL has substantially improved with treatment intensity adjustment based on the risk group in which a patient is classified. 2 Whereas allogeneic hematopoietic stem cell transplantation is used for very high-risk patients, stronger chemotherapeutic regimens are usually administered in recurrent ALL. 3 Although treatment duration differs according to risk group, treatment can last over 2 to 3 years. These intensive and prolonged therapies for pediatric ALL may increase the risk of psychiatric distress and various physical complications. Notably, chemotherapy affects emotional function in children with ALL and treatment with corticosteroids causes behavioral and psychological problems, such as mood swings, irritability, anxiety and depression. 4
Psychiatric distress can impair treatment compliance and quality of life in pediatric patients with cancer. Although one study reported that pediatric ALL patients experience similar emotional difficulties to those of their peers, 5 other studies have shown that approximately 10% to 30% of pediatric ALL patients experience psychiatric disorders.6,7 Moreover, some children experience emotional distress that occurs during their treatment and continues after treatment has ended.4,8 These results suggest that longitudinal studies are needed to observe the pattern of and identify potential risk factors for mental disorders in children with ALL. Previous studies are limited by small sample sizes or the use of cross-sectional designs. Therefore, we designed a nationwide population-based longitudinal study to analyze the pattern of psychiatric disorders in children with ALL using claims data from South Korea. The study aim was to analyze the incidence of depression, anxiety and stress/adjustment disorders using longitudinal analysis from the point of diagnosis of pediatric ALL.
Materials and methods
Using the International Classification of Diseases, Tenth Revision (ICD-10) code for ALL (C91.0), we identified a cohort of children with ALL (aged 0–18 years) using the Health Insurance Review and Assessment Service (HIRA) claims data for January 2009 to March 2016. The HIRA claims data are derived from the national medical insurance system, which covers 90% of the South Korean population. 9 We identified three main psychiatric disorders in this cohort using ICD-10 codes: depression (F32 and F33), anxiety (F40 and F41) and stress/adjustment disorder (F43). The flowchart describing selection of the study population is shown in Figure 1. The types of treatment for mental disorders were identified using the corresponding codes for medication (antipsychotic drugs, antidepressants, mood stabilizers and antianxiety drugs) and psychotherapy (individual psychotherapy: NN011–NN013, group psychotherapy: NN021–NN023 and family therapy: NN031–NN032). We evaluated treatment intensity using the number of psychotherapy and medication prescriptions.
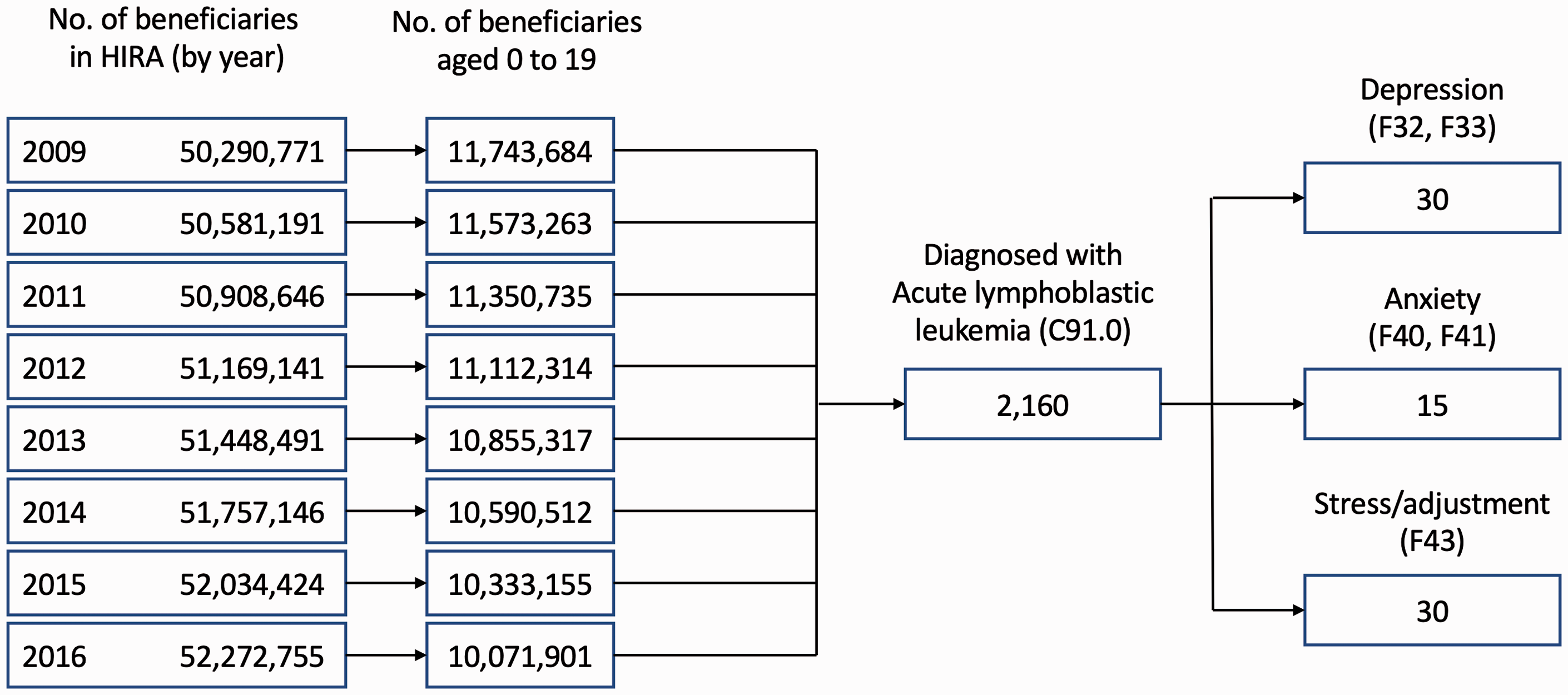
Flowchart of patient selection.
We analyzed the incidence of psychiatric disorders and observed the longitudinal incidence pattern according to the time of ALL diagnosis. We reviewed data starting from 1 year before ALL diagnosis to focus on the changes in psychiatric disorders around the time of ALL diagnosis. Descriptive statistics were used to describe the frequency of psychiatric disorders. We plotted density curves to illustrate the timing of mental disorders over the course of leukemia diagnosis. The density curves show the probability of each mental illness; the area under the curve = 100%. All statistical analyses were performed using R 3.0.2 software (www.r-project.org). Comparisons between and within groups were conducted using the chi-square test or Fisher exact test. This study was approved by the institutional review board of our institution (IRB No. AJIRB-441) and the requirement for informed consent was waived because we analyzed deidentified claims data. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement guidelines. 10
Results
A total of 2160 children with ALL were identified from the South Korean HIRA claims data for January 2009 to March 2016. Of the total, there were 1276 (59.1%) male patients. The follow-up time ranged from 42.5 to 111.5 months. Seventy-five (3.5%) of the pediatric ALL cases were coded with a psychiatric disorder at least once from 1 year before ALL diagnosis until the last follow-up. Among the children with a psychiatric disorder, the median age was 6 years (range, 3.0–18.0) and there were 41 (54.7%) male patients. The incidences of psychiatric disorders among male and female patients with ALL were 3.2% and 3.8%, respectively. The frequencies of psychiatric disorders are summarized in Table 1. The incidence in the groups aged 0 to 4 years, 5 to 9 years, 10 to 14 years and 15 to 18 years was 1.8%, 2.3%, 5.4% and 7.3%, respectively. Psychiatric disorders were more frequent in older (10–18 years) patients than in younger (0–9 years) patients (6.2% vs 2.0%). Depression, anxiety and stress/adjustment disorders were identified in 30 (1.4%), 15 (0.7%) and 30 (1.4%) patients, respectively.
Incidence of psychiatric disorders in children with ALL.

ALL, acute lymphoblastic leukemia; CI, 95% confidence interval.
*P value of incidence comparison between different age groups.
**P value of incidence comparison between the three psychiatric disorders.
The frequency of psychiatric disorders before and after ALL diagnosis is shown in Table 2. Seventy children were identified as having a psychiatric disorder (93.3%) after their ALL diagnosis. The proportions of depression and stress/adjustment disorder cases were relatively higher after ALL diagnosis than before ALL diagnosis. There was a significant difference between depression, anxiety and stress/adjustment disorders after ALL diagnosis (P = 0.024), but not before ALL diagnosis. The frequencies of each psychiatric disorder showed significant differences between before and after ALL diagnosis (depression, P < 0.001; anxiety, P = 0.009; stress/adjustment disorder, P < 0.001).
Psychiatric disorders before and after the diagnosis of ALL (N = 2160).

ALL, acute lymphoblastic leukemia; CI, 95% confidence interval.
*P value of incidence comparison between the three psychiatric disorders.
**P value of incidence comparison between psychiatric disorders before and after ALL diagnosis.
The overall incidence of psychiatric disorders peaked at 1 year after the diagnosis of ALL. In children younger than 5 years, the incidence of psychiatric disorders showed a delayed peak at approximately 3 years after ALL diagnosis (Figure 2a). Children aged 15 to 18 years had a higher incidence of psychiatric disorders than children of other ages. The incidence density plot for each psychiatric disorder is shown in Figure 2b. The incidence of depression was higher than that of the other psychiatric disorders at 1 year after ALL diagnosis. The incidence of depression and anxiety peaked again after 5 years after ALL diagnosis.

Frequency densities of psychiatric disorders stratified by (a) age group and (b) psychiatric disorder (the area under the density curve for each line is 1).
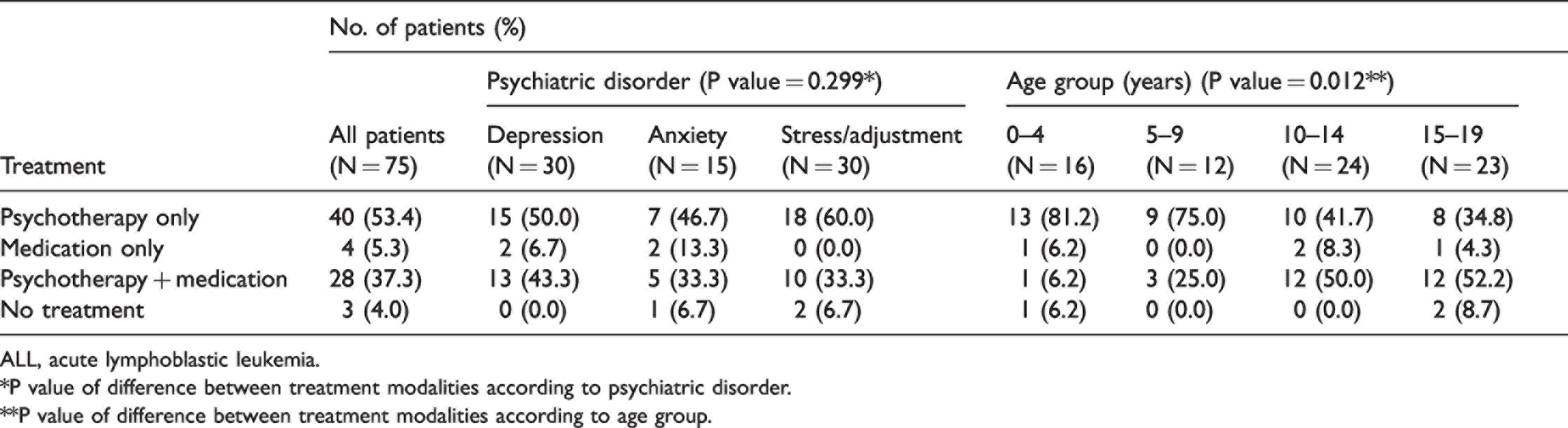
The treatments for psychiatric disorders are shown in Table 3. Seventy-two children (96.0%) were treated for psychiatric disorders with medication and/or psychotherapy. Of patients, 40 (53.4%), 4 (5.3%) and 28 (37.3%) were treated with psychotherapy only, medication only, and both treatments, respectively. There was no significant difference between treatment modalities according to psychiatric disorder, but treatment modality showed significant differences according to age group (P = 0.012). The number of prescriptions for psychotherapy and medication are summarized in Table 4. There was a significant difference between the number of prescriptions for psychotherapy and medication (P = 0.013).
Treatments by psychiatric disorder and age group in children with ALL.
ALL, acute lymphoblastic leukemia.
*P value of difference between treatment modalities according to psychiatric disorder.
**P value of difference between treatment modalities according to age group.
Prescription frequency of treatments for psychiatric disorders in children with ALL.

ALL, acute lymphoblastic leukemia.
P-value between the number of prescriptions for psychotherapy and medication.
Discussion
In this study, the incidence of psychiatric disorders among children with ALL younger than 18 years was 3.5%, and female children showed a higher incidence than male children. The observed incidence may be low because claims data may not reflect undiagnosed cases. However, we were unable to compare our results with those from previous studies because data are lacking on the incidence of psychiatric disorders in a similar clinical setting. In the general population, the prevalence of depressive among children aged 3 to 17 years in the United States is approximately 3.9%. 11 According to reports from South Korea, the prevalence of childhood depression ranges from 0.15% to 2%. 12 We found the incidence of depression to be 1.4% from 1 year before ALL diagnosis to the time of the last follow-up. Although we cannot directly compare our results with prevalence data from the general population, our data suggest that a portion of children with ALL experienced psychiatric distress from the time of their ALL diagnosis, through treatment and during follow-up.
The incidence of psychiatric disorders differed across age groups and was higher in older children. This age-dependent increase in the incidence of psychiatric disorders may reflect age-dependent differences in reality perception ability. Younger children (<10 years) may have a limited ability to understand the diagnosis of leukemia and the prolonged and painful treatment process associated with ALL. Moreover, younger children may not be capable of adequately expressing their physical and psychological symptoms. In contrast, teenagers are more likely to express their anxiety about death and problems with adjusting to school life, and to experience depressed mood, than younger children. Thus, teenagers are more likely to be diagnosed with psychological distress. Further, parents of children with ALL possibly neglect their psychological state because they are more concerned about their children’s physical health.
The density plot showed that most psychiatric disorders were identified after the diagnosis of ALL, and the incidence of psychiatric disorders peaked within 1 year after ALL diagnosis. These findings suggest that the diagnosis and treatment of ALL increase the risk of psychiatric disorders. There are several possible reasons for the development of psychiatric disorders peaking during this period. Painful diagnostic and therapeutic procedures, such as bone marrow examination, spinal tapping and catheter insertion (Hickmann or chemoport), can induce anxiety and posttraumatic stress disorder. 13 Intensive administration of anticancer drugs during the first year can increase the psychological stress and depressive mood that accompany chemotherapy-related acute side effects. 14 The use of corticosteroids, which are administered almost daily during the initial 4 weeks of chemotherapy as a remission-inducing regimen and for ≥2 years, may also contribute to the development of psychiatric disorders.15,16 Finally, the ALL diagnosis itself can induce psychiatric distress. Before the ALL diagnosis, only five children were identified as having psychiatric distress, which seems a relatively low incidence rate compared with that found in studies of adults with malignancies.17,18 During the period of diagnosis, cancer-related symptoms and diagnostic procedures can be risk factors for psychiatric disorders. However, children with ALL may show limited understanding of their serious diagnosis. The rapid progressive nature and fast diagnosis of ALL could be one reason for the rarity of psychiatric disorder during this period.
The density plot showed delayed secondary peaks in the incidences of depression and anxiety disorders ≥5 years after ALL diagnosis. This suggests that the risk of psychiatric disorders persisted during the long-term follow-up period. Even after an ALL cure, factors such as chronic complications, fear of recurrence and difficulties catching up on academic work may cause depression or stress/adjustment disorder. 19 Therefore, healthcare providers must be diligent in screening for psychological distress in children long after their ALL diagnosis.
Many patients may refuse therapy for psychiatric disorders because of the stigma associated with mental illness. However, the claims data suggested that patients were willing to receive treatment: 96.0% of patients with a psychiatric disorder were treated with medication and/or psychotherapy. Parents’ awareness of and ability to address their children’s psychological distress may affect the high treatment rate for mental disorders. However, nearly 25% to 30% of patients were prescribed treatment only once, suggesting a lack of continuous treatment. These findings indicate the need to develop an appropriate management protocol to guide the type and duration of treatments for psychiatric disorders in children with ALL.
Of the Children's Oncology Group (COG) protocols, ALTE07C1 includes assessments for psychiatric disorders in children with cancer. This protocol recommends the evaluation of psychiatric disorders using a set of neuropsychological tests, such as the Behavioral Assessment System for Children (BASC) 20 , at 9, 30 and 90 months after a cancer diagnosis. However, there are time and cost barriers to thorough implementation of the COG program/guideline in the clinical setting. Simpler assessments, such as the red flag items of the BASC (e.g., a child says “I want to die”), may be more practical to detect psychiatric problems. In the claims data analyzed here, most psychiatric disorders were likely to be coded and managed after presentation of one of the red flag items. Screening timing for psychiatric disorders should be more frequent than that recommended by the COG program, particularly for high-risk age groups (>10 years). Future studies are needed to develop practical guidelines for managing psychiatric disorders for pediatric oncologists and family members of children diagnosed with ALL.
This study had several limitations. First, the follow-up time for the cohort ranged from 42.5 to 111.5 months, which limited the ability to observe the effect of pediatric ALL on the development of psychiatric disorders in adulthood. We could not identify in the claims data clinical and other parameters such as cancer subtype; risk group; treatment protocol; complication profile; patient’s educational status; and parental economic, psychiatric and educational status. Neither could we analyze the treatment time for psychiatric disorders because this could not be defined using the claims data. To overcome these study limitations, a multicenter collaborative prospective or retrospective study is needed that includes neuropsychological and behavioral assessments. Another study limitation was the lack of diagnosis validation. The ICD-10 codes alone do not guarantee that psychiatrists diagnosed the psychiatric disorders examined in this study, and we cannot exclude the possibility of misclassification bias. Moreover, the diagnosis of psychiatric disorders is challenging, particularly in children younger than 6 years. Additional studies with appropriate designs are needed to confirm the validity of the present findings. However, because of the stigma associated with mental illness in South Korea, psychiatric diagnoses are carefully coded following a psychiatric consultation. 21 Therefore, we believe that the psychiatric disorders officially coded in the Korean claims data are reliable. This study did not include other mental disorders, such as inattention–hyperactivity, social withdrawal and learning problems, so more studies are warranted to investigate these disorders.
In conclusion, most psychiatric disorders were identified after the diagnosis of ALL in children, and the incidence of psychiatric disorder differed according to patient age and the time since ALL diagnosis. Our results suggest that screening and appropriate management for psychiatric disorders are required immediately after an ALL diagnosis and during the follow-up period.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221075223 - Supplemental material for Psychiatric disorders among children with acute lymphoblastic leukemia in South Korea: a nationwide population-based longitudinal study
Supplemental material, sj-pdf-1-imr-10.1177_03000605221075223 for Psychiatric disorders among children with acute lymphoblastic leukemia in South Korea: a nationwide population-based longitudinal study by Jaesung Heo, Jun Eun Park, O Kyu Noh and Yunmi Shin in Journal of International Medical Research
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Bio & Medical Technology Development Program of the National Research Foundation funded by the Korean government (MSIT) (No. 2020M3A9E8024907).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.