
Abstract
Tumours with a high mutation burden exhibit considerable neoantigens and tumour-infiltrating lymphocytes. RNA editing by ADAR1 is a source of changes in epitope. However, ADAR1 expression in cancer cells and tumour-infiltrating lymphocyte levels in triple-negative breast cancer have not been well evaluated. We immunohistochemically examined ADAR1 expression in 681 triple-negative breast cancer patients and analysed their clinicopathological characteristics. We also analysed basal-like tumours using The Cancer Genome Atlas data. Among the 681 triple-negative breast cancer patients, 45.8% demonstrated high ADAR1 expression. Tumours with high ADAR1 expression exhibited high tumour-infiltrating lymphocyte levels, considerable CD8 + T lymphocyte infiltration, high histological grade and high expression of interferon-related proteins, including HLA-ABC, MxA and PKR. Among patients with lymph node metastasis, those with high tumour-infiltrating lymphocyte levels and low ADAR1 expression demonstrated the best disease-free survival. The Cancer Genome Atlas data analysis of basal-like tumours revealed significant positive correlation between ADAR1 and CD8B expression and positive association of high ADAR1 expression with immune responses and apoptosis pathways. We detected high ADAR1 expression in half of the triple-negative breast cancer patients. In addition to DNA mutations, RNA editing can be related to neoantigens; hence, we need to explore non-synonymous mutations exclusively found using RNA sequencing data to identify clinically relevant neoantigens.
Keywords
Introduction
Triple-negative breast cancer (TNBC) accounts for ~15% of all breast cancers and are associated with high histological grade and aggressive clinical behaviour. These cancers are defined by the absence of expression of oestrogen receptor (ER), progesterone receptor (PR) or human epidermal growth factor receptor 2 (HER2). 1 Since TNBC lacks a therapeutic target, patients with this type of breast cancer do not benefit from molecularly targeted treatments such as endocrine therapy or trastuzumab. 2 Recently, a growing body of evidence suggests that these patients are potential candidates for immunotherapy. 3
The use of immunotherapy has markedly altered the field of anti-cancer treatment. 4 Tumours with a high mutation burden are known to have considerable neoantigens and tumour-infiltrating lymphocytes (TILs). 5 Tumour mutation burden is mainly analysed by assessing mutation rates using DNA sequencing data. However, RNA editing is another source of alterations in amino acid sequences and epitopes. The frequency of RNA editing in many types of tumours has been explored using The Cancer Genome Atlas (TCGA) data, and a substantial amount of mutational load due to RNA editing has been detected. 6 The adenosine deaminase acting on RNA (ADAR) family of editases is a group of enzymes responsible for converting an adenosine into an inosine (A-to-I) in structured or double-stranded (ds) RNAs; this is the most prevalent form of RNA editing in mammals. Cellular functions and regulations can be altered by A-to-I editing through changes in messenger RNA (mRNA) splicing, stability, localisation and translation as well as interference with the binding of regulatory RNAs. 7 With the improvement in sequencing and analysis technologies, researchers have studied RNA editing events using RNA sequencing data.6–9
In humans, the ADAR family comprises ADAR1, ADAR2 and ADAR3, which share repeated copies of dsRNA-binding domains and a catalytic adenosine deaminase domain. 10 Among them, ADAR1 is the major contributor to RNA editing in cancer, especially in breast. Anantharaman et al. 11 have demonstrated that breast cancer cells show elevated ADAR1 but reduced ADAR2 mRNA levels compared to normal cells. ADAR3 has demonstrated no deaminase activity in vitro. 10 ADAR1 regulates the editing frequency and number of edited sites.6–8 ADAR1 mRNA expression is significantly positively correlated with the RNA editing level. 7 RNA sequencing analysis has revealed that ADAR1 is among the top 5% of upregulated genes in relapsed lobular breast cancer. 10 Fumagalli et al. 7 have demonstrated elevated ADAR expression in breast cancer compared with that in matched normal tissues, which occurs because of an aberrantly high copy number. They have also demonstrated that ADAR expression and editing are associated with type I interferon response in the tumour environment. 7 We have previously studied the expression of human leukocyte antigen (HLA)-ABC and MxA, which is known to be induced by interferon signalling, in TNBC and have identified a significant correlation between TIL levels and HLA-ABC/MxA expression in tumour cells.12,13 Despite evidence suggesting that ADAR1 expression in cancer tissue is associated with elevated interferon signalling, the prognostic significance and relationship between ADAR1 expression in cancer cells and TIL levels in TNBC have not yet been well evaluated. We examined ADAR1 expression using immunohistochemistry and analysed the clinicopathological characteristics, including TIL levels and expression of other interferon-related proteins, of high ADAR1-expressing TNBCs. We also analysed basal-like tumours using TCGA data to evaluate the relationship between ADAR1 and CD8 gene expression and to characterise tumours with high ADAR1 expression.
Materials and methods
Patient and tissue specimens
We evaluated 681 TNBC patients whose resected tissues were obtained by surgeries conducted between 2004 and 2010 at Asan Medical Center. In this group, 472 of the 681 patients did not present with lymph node metastasis and received four cycles of adjuvant anthracycline and cyclophosphamide (AC: adriamycin, 60 mg/m2 and cyclophosphamide, 600 mg/m2). The remaining 209 patients presented with lymph node metastasis and were treated with four cycles of AC, followed by either four cycles of paclitaxel (175 mg/m2) or four cycles of docetaxel (75 mg/m2). In total, 550 patients (80.8%) received radiotherapy. The median follow-up period was 78.3 months. All patients were chemotherapy-naïve and radiotherapy-naïve preoperatively. Clinical information was obtained from medical records and pathology reports from the surgery. Exemption from informed consent after the de-identification of information was approved by the Institutional Review Board of Asan Medical Center.
Histological evaluation
Haematoxylin and eosin–stained slides were reviewed by two pathologists (H.J.L. and G.G.) and were histopathologically analysed for TILs (defined as the percentage of stroma of invasive carcinoma that is infiltrated by lymphocytes in 10% increments), 14 histological grade, tumour size, pT stage, pN stage and lymphovascular invasion. The histological type was defined based on the 2012 WHO classification criteria, and the histological grade was assessed using the modified Bloom–Richardson classification. 15
Tissue microarray construction and immunohistochemistry
Formalin-fixed, paraffin-embedded tissue samples were evaluated using a tissue-arraying instrument, as previously described. 16 Each sample was arrayed in three 1-mm-diameter cores to minimise tissue loss and mitigate tumour heterogeneity effects. Tissue microarray sections were stained using an automatic immunohistochemical staining device (Benchmark XT; Ventana Medical Systems, Tucson, AZ, USA). Antibodies to target ADAR1 (1:200 dilution; HPA003890; Atlas Antibodies, Stockholm, Sweden), MxA (1:1000; ab95926; Abcam, Cambridge, UK), double-stranded RNA (dsRNA), activated protein kinase (PKR, 1:400; ab32052; Abcam), CD8 (1:200; DAKO, Glostrup, Denmark) and HLA-ABC (1:1600; ab70328, EMR8-5; Abcam) were used. 12 As controls for ADAR1, cell blocks from human breast cancer cell lines were used (Supplementary Figure S1). 13
ADAR1, MxA, PKR and HLA-ABC intensities were evaluated as a four-value intensity score (0, 1, 2 and 3). The percentages of nuclear ADAR expression, membranous and/or cytoplasmic expression of HLA-ABC and cytoplasmic MxA and PKR expression were also evaluated. An ‘immunoreactive score’ was generated as the product of the intensity and percentage of positive cells. Immunoreactive scores for ADAR1, MxA and PKR were dichotomised based on the mean protein expression value. We categorised HLA-ABC expression in tumour cells as one of the three levels, as previously described (strongly positive, expression in >75% of tumour cells; weakly positive, expression in 25%–75% of tumour cells and negative, loss of expression in >75% of tumour cells). 17
The immunostained tissue microarray slides for CD8 were scanned using a digital microscopy scanner (Pannoramic 250 FLASH; 3DHISTECH Ltd., Budapest, Hungary). The numbers of CD8 + cells in tissue microarray cores were counted using the NuclearQuant module of Pannoramic Viewer 1.15.2 (3DHISTECH Ltd.).
TCGA and Cancer Cell Line Encyclopedia data
TCGA data portal was used to download the breast cancer data. 18 In total, 84 cases of basal-like breast cancer were analysed according to the PAM50 predictor. We downloaded level-3 gene expression data derived from an Agilent custom 244K whole-genome microarray and somatic mutation data obtained using exome sequencing from Illumina Genomic Analyzer. Gene expression levels were median-centred by genes.
Gene Set Enrichment Analysis (GSEA) was performed using javaGSEA v2.2.4, with gene sets derived from the Kyoto Encyclopedia of Genes and Genomes pathway database. 19 Basal-like tumours were dichotomised based on the mean ADAR1 gene expression value.
ADAR mRNA expression of eight breast cancer cell lines using GeneChip Human Genome U133 Plus 2.0 Array included in cancer cell line encyclopedia (CCLE) was analysed (Supplementary Figure S1).
Statistical analysis
All statistical analyses were conducted using SPSS statistical software (version 18; SPSS, Chicago, IL, USA) or R (https://www.R-project.org/). The chi-square test, log-rank test, Spearman’s correlation and forward conditional Cox proportional hazards regression model were used to evaluate the data. All tests were two-sided, and p < 0.05 was considered statistically significant.
Results
ADAR1 expression in TNBCs
ADAR1 was expressed in tumour cell nuclei (Figure 1 and Supplementary Figure S1). The breast cell lines with relatively high ADAR mRNA expression (SK-BR-3, ZR-75-1, BT-20 and BT-474) show high ADAR1 protein expression, while the cell lines with low ADAR mRNA expression (T-47D and MCF-7) show low ADAR1 protein expression (Supplementary Figure S1). Among 681 TNBCs examined, ADAR1 expression was evaluable in 679 tumours, of which 311 (45.8%) showed a high ADAR1 expression. TIL levels assessed in whole-section slides were higher in tumours with high ADAR1 expression (median: 30.0; interquartile range (IQR): 10–60) than in those with low ADAR1 expression (median: 20.0; IQR: 5–60, p = 0.022). Tumours with high ADAR1 expression also demonstrated more CD8 + T lymphocyte infiltration (median, 435.0; IQR: 164.3–869.2) in the 0.6-mm tissue microarray core than those with low ADAR1 expression (median: 232.7; IQR: 86.0–536.6; p < 0.001). The histological grade and expression of interferon-related proteins, namely, HLA-ABC, MxA and PKR, were significantly higher in tumours with high ADAR1 expression than in those with low ADAR1 expression (Table 1).

Representative figures of ADAR1 expression in breast cancer. (a) Tumour cells show nuclear positivity for ADAR1. (b) Tumour cells are negative for ADRA1 (immunohistochemistry, 400×).
Clinicopathological characteristics of patients with breast cancers according to ADAR1 expression levels.

HLA: human leukocyte antigen; LN: lymph node; TIL: tumour-infiltrating lymphocyte.
p values calculated by χ2 test or Fisher’s exact test.
Bold values denotes the significance level of 5% (p < 0.05).
Prognostic significance of ADAR1 expression in TNBCs
Because standardised adjuvant chemotherapy differs between patients having tumours with lymph node metastasis and those without lymph node metastasis, we analysed the prognostic significance of ADAR1 expression according to the presence or absence of lymph node metastasis. In the patient group without lymph node metastasis who were treated with adjuvant anthracycline-based chemotherapy, ADAR1 expression exhibited no prognostic significance in disease-free survival (Figure 2(a), p = 0.720). In the patient group with lymph node metastasis who were treated with adjuvant anthracycline- and taxane-based chemotherapy, patients with high ADAR1 expression demonstrated poorer disease-free survival than those with low ADAR1 expression; however, this difference was not statistically significant in univariate and multivariate analyses (Table 2, Figure 2(b), p = 0.109 and 0.147, respectively).
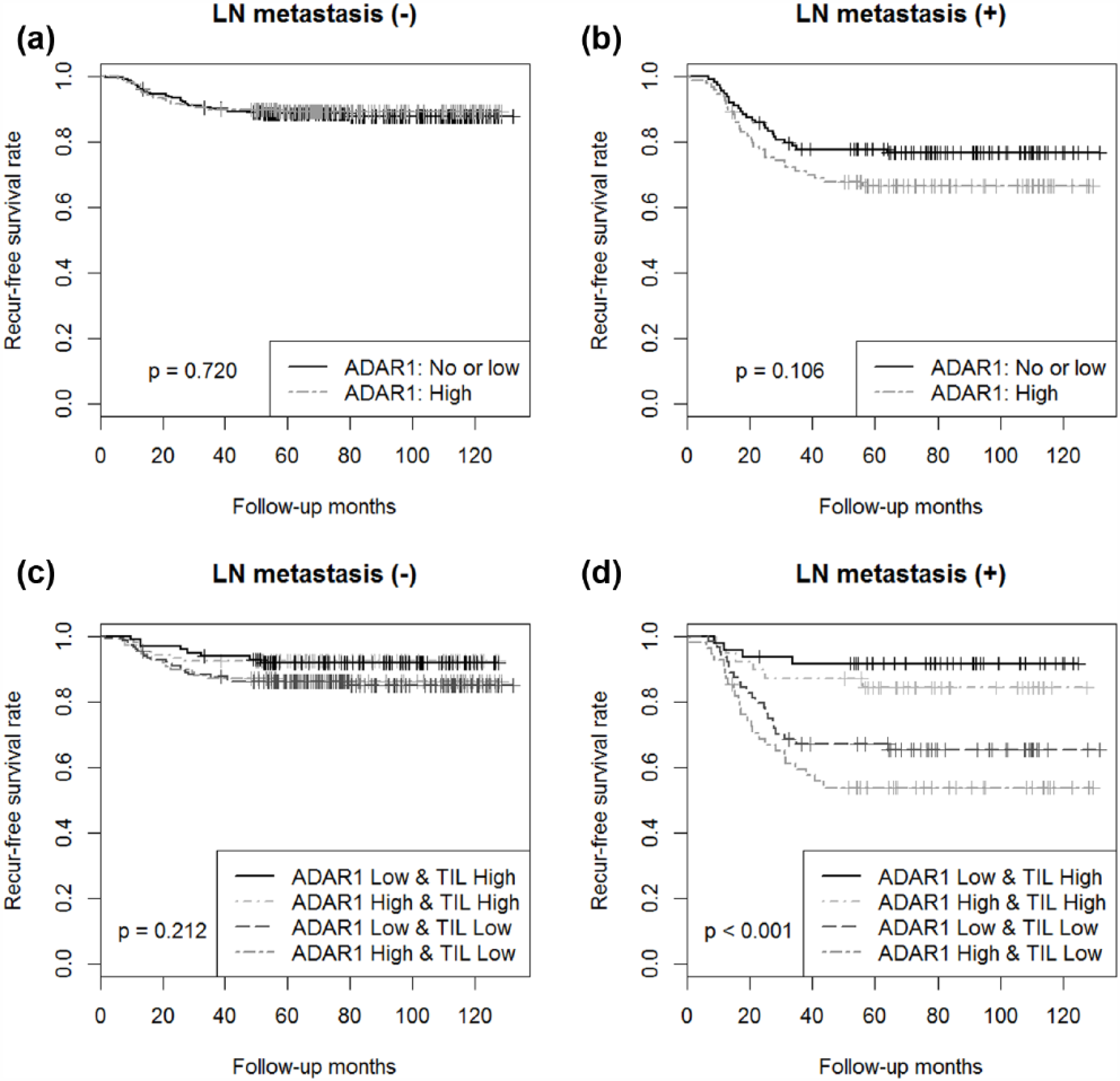
Kaplan–Meier disease-free survival curves according to ADAR1 expression. (a) In the patient group without lymph node metastasis, ADAR1 expression exhibited no prognostic significance in disease-free survival. (b) In the patient group with lymph node metastasis, patients with high ADAR1 expression demonstrated worse disease-free survival, but this was not statistically significant. (c) In the patient group without lymph node metastasis, patients with a high TIL levels tended to demonstrate favourable clinical outcomes, regardless of ADAR1 expression. (d) In the patient group with lymph node metastasis, patients with low TIL levels and high ADAR1 expression demonstrated worst outcomes.
Cox proportional hazard regression model of disease-free survival in the patients with triple-negative breast cancers with lymph node metastasis based on clinicopathological variables.

CI: confidence interval; HR: hazard ratio; LVI: lymphovascular invasion; TIL: tumour-infiltrating lymphocyte.
Bold values denotes the significance level of 5% (p < 0.05).
We further analysed the prognostic significance according to the combination of TIL levels and ADAR1 expression. In the patient group without lymph node metastasis, patients with high TIL levels tended to exhibit better clinical outcomes than those with low TIL levels, regardless of ADAR1 expression (Figure 2(c), p = 0.212). In the patient group with lymph node metastasis, patients with high TIL levels exhibited better disease-free survival than those with low TIL levels, but the survival curves were further separated by ADAR1 expression levels in tumour cells (Figure 2(d), p < 0.001). Patients with low TIL levels and high ADAR1 expression exhibited the worst outcomes.
Analysis of TCGA data
To explore the relationships among DNA mutation load, RNA editing and TIL levels, we analysed the total number of DNA mutations and ADAR1 and CD8B gene expression levels in 84 basal-like tumours using TCGA data. As previously demonstrated, no correlation was noted between the total number of DNA mutations and CD8B gene expression (Figure 3(a), p = 0.054). 13 However, a statistically significant positive correlation was present between ADAR1 and CD8B gene expression levels (Figure 3(b), correlation coefficient = 0.264, p = 0.016). The total number of DNA mutations was not correlated with ADAR1 expression (p = 0.366).

Correlations of CD8B gene expression with (a) the total number of mutations and (b) ADAR1 expression in 84 basal-like tumours using TCGA data.
To analyse the biological characteristics of tumours with high ADAR1 expression, we conducted a GSEA of basal-like tumours with a high/low ADAR1 expression. The major groups or ‘gene sets’ with high ADAR1 expression were associated with immune responses, such as ‘cytosolic DNA-sensing pathway’, ‘antigen processing and presentation’, ‘T-cell receptor signalling pathway’, ‘natural killer cell–mediated cytotoxicity’, ‘toll-like receptor signalling pathway’, ‘chemokine signalling pathway’, ‘B cell receptor signalling pathway’ and ‘Janus kinase/signal transducer and activator of transcription (JAK/STAT) signalling pathway’ (Table 3, Supplementary Figure S2). ‘Apoptosis’ was the 15th enrichment pathway for tumours with high ADAR1 expression.
Differentially regulated pathways in basal-like tumours with high ADAR1 expression.

NES: normalised enrichment score; FDR: false discovery rate; RIG-I: retinoic acid-inducible gene I; JAK/STAT: Janus kinase/signal transducer and activator of transcription.
Discussion
The main target of A-to-I editing is Alu repeat sequences, which can form a double-stranded structure. 20 In addition to the highly repetitive Alu elements, ADAR1 can bind non-Alu dsRNA sequences, including 3′-untranslated regions and primary microRNAs and affect both their structure and activities.6,10 RNA editing alters amino acids, which can affect protein function, modulates alternative splicing by the generation or elimination of splicing sites and regulates transcript stability by modifying microRNAs and microRNA-binding sites.10,21 ADAR1 plays a role in regulating interferon responses: it suppresses the type I interferon response. 8 Upon viral infection, produced dsRNA induces an antiviral interferon response, and the expression of the interferon-inducible cytoplasmic version of ADAR1 increases. Cytoplasmic ADAR1 then edits all cytoplasmic RNAs and reduces the interferon response to limit self-damage. Thus, RNA editing by ADAR can dynamically control the interferon response. 21 In fact, human ADAR1 gene mutations are associated with upregulated interferon-stimulated gene expression in patients with Aicardi–Goutières syndrome. ADAR1 deletion in mouse models also causes an elevated interferon response. 21 ADARs are known to be important regulators of normal development, and A-to-I RNA editing is an important contributor to cancer pathogenesis. 10 In an analysis of 4480 cancers using TCGA data, ADAR expression has been associated with both ADAR copy number and signal transducer and activator of transcription 1 (STAT1) expression, which is a proxy for type I interferon response. 7 We confirmed the positive correlation between the expression of ADAR1 and other interferon-inducible proteins, namely, HLA-ABC, MxA and PKR, in TNBCs. ADAR1 expression was also positively correlated with TIL levels.
Although ADAR1 expression was positively correlated with TIL levels, patients with high ADAR1 expression demonstrated a worse disease-free survival rate than those with low ADAR1 expression. We have previously shown that high TIL levels and high MxA expression in TNBCs were associated with favourable clinical outcomes.12,22 Conversely, Fumagalli et al. 7 have demonstrated that ADAR silencing in breast cancer cell lines (MDA-MB-231, MCF-7 and BT-474) is associated with a statistically significant decrease in cell proliferation and increase in cell apoptosis, suggesting the role of ADAR in cell proliferation and apoptosis. We performed a GSEA study and demonstrated that tumours with high ADRA1 expression are associated with immune responses and the apoptosis pathway. These results might be because of the independent effect of type I interferon response and ADAR amplification. 7
A-to-I editing can be an important parameter for cancer treatment strategies because its levels are deregulated during cancer and can promote cancer progression. 21 Analysis using TCGA data demonstrated that RNA editing is abundant in many types of human cancers. Several reports have also revealed that RNA editing rates are higher in tumour samples of breast, thyroid and lung cancer than in normal tissue. However, in chromophobe renal cell carcinoma, renal papillary cell carcinoma and metastatic melanoma, A-to-I editing levels are reduced in tumour tissues.6,10 The downregulation of ADAR1 expression in metastatic melanoma promotes tumour growth and cell proliferation. 10 In oesophageal squamous cell carcinoma, ADAR1 has been identified as an oncogene and negative predictor of overall survival. 10 Therefore, studies exploring the possibility of the modulation of ADAR and downstream molecular activity are warranted to develop novel therapeutic modalities.
The discovery of neoantigens is an important research topic for developing personalised immunotherapies using a vaccine or adoptive antigen-specific T-cell therapy. 23 In general, tumour mutational load is positively correlated with the number of neoantigens, TIL levels and T-cell diversity.24,25 We analysed TCGA data of basal–like breast cancers defined by PAM50 subtype predictors, because basal-like breast cancers are highly concordant with TNBCs defined by immunohistochemistry (concordance rate: ~75%), and basal-like breast cancers that are not triple negative show similar genomic features to those of basal-like TNBCs. 26 However, in the basal-like breast cancers assessed using TCGA data, we could not identify a positive correlation between CD8 gene expression and the total number of DNA mutations. In this study, we analysed the relationship between CD8B and ADAR1 gene expression and noted a positive correlation between these two genes. Given that RNA editing, in addition to DNA mutations, can be related to changes in epitope, we need to consider non-synonymous mutations exclusively found in RNA sequencing data to identify clinically relevant neoantigens.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT & Future Planning (2015R1C1A1A02036484 and 2016R1D1A1B03935367) and the Korean Health Technology R&D Project, Ministry of Health & Welfare (HI17C0337).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.