
Abstract
Patients with breast cancer along with metastatic estrogen and progesterone receptor (ER/PR)- and human epidermal growth factor receptor 2 (HER2)-negative tumors are referred to as having metastatic triple-negative breast cancer (mTNBC) disease. Although there have been many new treatment options approved by the Food and Drug Administration for ER/PR-positive and Her2/neu-amplified metastatic breast cancer, relatively few new agents have been approved for patients with mTNBC. There have been several head-to-head chemotherapy trials performed within the metastatic setting, and much of what is applied in clinical practice is extrapolated from chemotherapy trials in the adjuvant setting, with taxanes and anthracyclines incorporated early on in the patient's treatment course. Select synergistic combinations can produce faster and more significant response rates compared with monotherapy and are typically used in the setting of visceral threat or symptomatic disease. Preclinical studies have implicated other possible targets and mechanisms in mTNBC. Ongoing clinical trials are underway assessing new chemotherapeutic strategies and agents, including targeted therapy and immunotherapy. In this review, we evaluate the standard systemic and future treatment options in mTNBC.
Keywords
Background
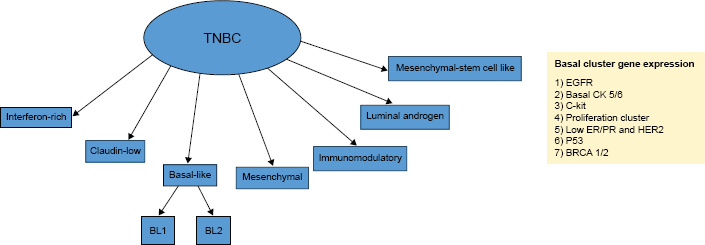
With 246,660 new diagnoses and 40,450 deaths projected for 2016, breast cancer remains the most commonly diagnosed and the second leading cause of cancer-related deaths among women in USA. 1 Although most patients will be diagnosed with localized breast cancer, ~6% of patients will present with de novo metastatic disease and ~10%–40% of patients with localized breast cancer will relapse systemically (as opposed to locally).2,3 The prognosis of patients with metastatic breast cancer (mBC) is heterogeneous and can range from several months to many years depending upon many factors, including, but not limited to, estrogen and progesterone receptor (ER/PR) status and human epidermal growth factor receptor 2 (HER2) receptor status.2,3 Metastatic tumors that are ER/PR negative and HER2 negative are characterized as being triple negative and, although not considered synonymous, are generally thought to consist of tumors, which harbor a basal-like molecular subtype (Fig. 1). Most new treatment options for mBC recently approved by the Food and Drug Administration (FDA) are only effective for ER/PR-positive or HER2-positive metastatic tumors, and relatively few new agents have been approved for the subset of patients with metastatic triple-negative breast cancer (mTNBC). Single-agent chemotherapy continues to serve as the backbone of mBC treatment. The lack of efficacious therapy within this cohort, combined with the propensity to develop visceral or central nervous system (CNS) metastasis (as opposed to more indolent bone or soft tissue predominant metastases), has translated into an overall survival (OS) that has remained stagnant over the past 20 years.4–6 As a result, patients with mTNBC continue to have a considerably worse OS when compared to their mBC counterparts. The purpose of this review is to perform a comprehensive evaluation of the principles of systemic treatment, compare standard systemic palliative options, and highlight the promising approaches in ongoing clinical trials in mTNBC.
Principles of Treatment
Although mTNBC encompasses a unique subset of patients, the therapeutic approach mimics that of other subsets of patients with mBC (Fig. 2). As opposed to patients with localized breast cancer where the primary goal of treatment is cure, treatment of mBC focuses on prolonging the progression-free survival (PFS) and OS and improving the quality of life (QOL) through the reduction or stabilization of tumor burden and other cancer-related symptoms.7–9 Due to the palliative intent, it is critical that an individualized approach is taken that incorporates patient, disease, and treatment-related factors, including an individual oncologist treatment preference.

Systemic treatment algorithm for mTNBC.
Given the lack of prospective data showing an improvement in OS among patients with mBC who are treated with combination rather than single-agent chemotherapy 10 and the lack of a well-validated, consensus-derived surrogate endpoint, 11 the choice between chemotherapy strategies is typically dependent upon many factors, including the degree of tumor burden, rate of disease progression, site of metastasis, organ involvement and function, cancer-related symptoms, and residual toxicities from prior therapies. 12 Taking these variables into account, clinicians often use combination chemotherapy in mBC only when it has been determined that the patient is in need of significant treatment response or stabilization in a relatively short amount of time. 13 While minimizing the burden of disease outside the CNS reduces the risk of CNS metastases, systemic chemotherapy is relatively ineffective at treating CNS disease.
Perhaps the most critical variable to consider in making a treatment decision in mBC involves the assessment of the patient's Eastern Cooperative Oncology Group performance status (ECOG PS) or Karnofsky performance status, especially if the clinician determines that the treatment is likely to cause more harm than benefit or significantly decreases QOL. Preexisting treatment-related toxicities also play a role in the treatment selection, as side effect profiles and cumulative toxicities (ie, anthracyclines in patients with cardiac disease, microtubule inhibitors or platinums in patients with neuropathy, and platinum compounds in patients with chronic kidney disease or high frequency hearing loss) vary. Patients with progression of their disease within several months of treatment with a chemotherapeutic agent are often deemed to have resistance to that agent or class of agents. With this in mind, these patients are often sequentially treated with a chemotherapeutic agent, which has a different mechanism of action. As with any chronic disease requiring long-term follow-up and treatment, an approach in mBC incorporating patient preferences into the shared decision-making process is critical for patient compliance and QOL. For example, some patients may be willing to accept more risk in return for a greater response, whereas others desire a specific route of chemotherapy (orally vs intravenously) and a limited number of infusions or duration of infusions and frequency of phlebotomy, or a desire to avoid specific side effects, such as alopecia.
As opposed to the limited and fixed treatment duration that occurs in the curative intent setting, treatment duration for mBC is more individualized and potentially indefinite. Patients are typically continued on therapy until best response, disease progression, or significant toxicity. With regard to the concept of maintenance (continual) treatment, a 2011 meta-analysis analyzed 11 trials of 2,300 treatment-naive patients with mBC, some of which were mTNBC. Maintenance therapy when compared to intermittent treatment found that the former was associated with both an improved PFS and OS. 14 Another trial with 324 patients with mBC (<25% of which were mTNBC) who achieved at least stable disease on paclitaxel and gemcitabine (PG) were randomized to observation or maintenance PG chemotherapy until disease progression. 15 Maintenance chemotherapy resulted in a higher PFS rate at six months (60% vs 36%) and an improved OS (32 vs 24 months) but was associated with a higher incidence of grades 3–4 neutropenia (61% vs 0.9%) and grades 2–3 neuropathy (0.9% vs 0%). In an unplanned subset analysis, the improved survival was primarily seen among those women who were <50 years of age, had ER/PR-negative tumors, had previously responded to chemotherapy, and had predominantly visceral disease. Additionally, although >70% of the patients had ER/PR-positive tumors, >20% of the patients were endocrine naive. Based on this trial, it is generally recommended that young patients who are responding to treatment continue beyond best response, especially if they experienced limited associated treatment toxicity.
The decision to switch therapies in mBC may be due to serial changes in tumor markers, evidence of progressive disease on imaging (new metastasis or increasing size of previously documented metastatic lesions), and/or clinical deterioration during treatment (due to increasing disease-related symptoms, intolerable treatment toxicities, or declining performance status). Although response evaluation criteria in solid tumors (RECIST) is required by most clinical trials to assess for disease progression, clinicians could reasonably use similar thresholds before abandoning a given line of treatment. The RECIST defines PD as a 20% or more increase in the sum of measurable target lesions compared with the smallest sum previously recorded, the appearance of any new lesions, or the worsening of existing nontarget lesions, such as bone metastases. 16
Single-agent Chemotherapy
Due to the lack of high-quality comparative data, the most efficacious sequencing of chemotherapy agents in the treatment of mBC has yet to be defined. Despite several head-to-head chemotherapy trials within the metastatic setting, much of what is applied in clinical practice is extrapolated from chemotherapy trials in the adjuvant setting, with taxanes and anthracyclines incorporated early in the patient's treatment course (granted, they had not received similar therapy in the adjuvant setting).
Microtubule inhibitors
The class of chemotherapy agents commonly referred to as taxanes are among the most commonly used agents in mBC, especially when used as a single agent, and this class consists of drugs, such as docetaxel, paclitaxel, and nab-paclitaxel. Docetaxel can be administered either every three weeks or weekly on a three-week-on/one-week-off schedule (Table 1). 17 In a randomized trial including only patients receiving adjuvant as opposed to palliative chemotherapy, weekly three-week-on/one-week-off schedule was associated with a significantly improved disease-free survival compared to the every three-week schedule. 18 Though it is generally considered to be safe and well tolerated, docetaxel is associated with the risk of fluid retention that can be reduced by steroid premedication, more myelosuppression (most notably neutropenia), and gastrointestinal toxicities, such as stomatitis, nausea, vomiting, and diarrhea. 19 Paclitaxel can also be administered either every three weeks or weekly on a three-week-on/one-week-off schedule.17,20 The former schedule is typically recommended based on its associated OS superiority seen in a recent meta-analysis. 17 Since it is primarily renally excreted, patients with underlying mild-to-moderate liver dysfunction may be treated with paclitaxel. Paclitaxel when compared to docetaxel is associated with greater rates of associated treatment-related neuropathy and myalgia. Additionally, due to paclitaxel's cremophor mixture preparation, patients are at risk for developing rare but serious allergic reactions, which prompts at least the initial use of steroid premedication. Direct comparison of docetaxel and paclitaxel in patients with mBC who previously progressed after an anthracycline-based chemotherapy regimen revealed that docetaxel produced a significantly better median time to progression (TTP; 5.7 vs 3.6 months) and OS (15.4 vs 12.7 months).21,22 However, patients receiving docetaxel had significantly higher rates of both hematologic and nonhematologic toxicities.
Commonly used systemic treatments in metastatic triple-negative breast cancer. 102

Orally administered.
Similar to other taxanes, nab-paclitaxel has significant activity in mBC and is administered either weekly on a three-week-on/one-week-off schedule or every three weeks.23–25 Although more expensive, the side effect profile is similar to paclitaxel. However, nab-paclitaxel has a shorter infusion time and, due to its albumin-bound formulation, is associated with a lower risk of allergic reactions, which allows for the exclusion of steroid premedication and its associated risks of inducing hyperglycemia. In the Alliance trial, 22 799 previously untreated patients with mBC were randomized to the three-week-on/one-week-off schedules of either paclitaxel or nab-paclitaxel and found no difference in PFS or OS but found a higher rate of grade 3 or higher treatment-related toxicity in the nab-paclitaxel arm, including sensory neuropathy (27% vs 18%) and hematologic toxicity (55% vs 22%).
Eribulin, through its inhibition of tubulin and microtubule polymerization, was shown to have activity in heavily pretreated patients with mBC and was approved by the FDA in USA for patients who progressed after receiving two different systemic chemotherapy agents. Administered on days 1 and 8 of a 21-day cycle, eribulin is often associated with less neuropathy than other microtubule-directed agents and can be administered with dose adjustment for mild-to-moderate liver and kidney dysfunction. The activity of eribulin was shown in a Phase III trial of 762 patients who were randomly assigned to treatment with eribulin or to another chemotherapy agent selected based on the physician's and patient's choice.
26
Although the treatment with eribulin significantly improved OS (13.1 vs 10.6 months) in a heavily pretreated population, all-grade neutropenia was observed in 45% of patients (5% of which was grade 3 or 4 in severity), and peripheral neuropathy was found to be the most common adverse event leading to drug discontinuation (5% of patients). A randomized trial comparing eribulin with capecitabine in patients with mBC (~25% of which were TNBC) who had received prior anthracycline and taxane therapy found no difference between the treatment arms with regard to overall response rate (ORR: 11% vs 11.5%) or PFS (four months in each). Patients in the eribulin treatment arm had an OS that approached clinical significance when compared to those receiving capecitabine (15.9 vs 14.5 months;
Vinorelbine, a semisynthetic vinca alkaloid administered on days 1 and 8 of a 21-day cycle, is another commonly used mBC chemotherapy agent, as it not only has single-agent activity in heavily pretreated patients (ORR: 25%–45%) but is also associated with side effects, including nausea, constipation, peripheral neuropathy, and hair loss.28–34 Ixabepilone is another FDA-approved drug in the treatment of mBC and acts as a nontaxane tubulin-polymerizing agent that has activity in taxane-resistant patients.35–37 A clinical trial of patients with mBC (~25% of which were TNBC) who were previously exposed to anthracyclines and taxanes found that, although single-agent ixabepilone was associated with grades 3–4 peripheral sensory neuropathy in 14% of patients, it was also associated with an ORR of 19%, a PFS of 5.7 months, and an OS of 8.6 months. 37 However, in a trial comparing ixabepilone with paclitaxel and nab-paclitaxel, ixabepilone was found to be associated with a shorter PFS (7.6 vs 10 months) and OS (21 vs 26 vs 27 months) but a lower incidence of hematologic toxicity (12% vs 21% vs 51%) and equal rates of grades 3–4 sensory neuropathy (25%). 37 Despite a moderate adverse side effect profile compared to other taxanes or taxane-like agents, the utilization of ixabepilone is often limited secondary to the poor ECOG PS of the heavily pretreated mBC population. In fact, given its modest benefit and adverse effect profile, the agent was denied for approval in Europe. 38
Anthracyclines
With an ORR between 30% and 50%, the anthracyclines are one of the most active drug classes in breast cancer. However, their use in the metastatic setting is often limited secondary to concerns that exceeding cumulative dose levels from prior adjuvant chemotherapy will raise the risk of cardiotoxicity and, thus, is typically reserved for anthracycline-naive patients. Chemotherapy agents included within this class are doxorubicin and epirubicin, both of which are generally administered every three weeks,39–41 and pegylated liposomal doxorubicin, which is typically given every four weeks.40,41 All three anthracyclines can be given to patients with mild-to-moderate hepatic dysfunction. In the absence of comparative randomized trials, due to the perception of their improved tolerability, doxorubicin and epirubicin are typically given on weekly schedules. A trial of 509 patients with mBC (~50% had tumors that were ER negative), 56% of whom had previously received anthracyclines, patients were randomized to receive pegylated liposomal doxorubicin every four weeks or doxorubicin every three weeks. Compared with pegylated liposomal doxorubicin, doxorubicin resulted in a higher ORR (38% vs 33%) but similar PFS (7.8 vs 6.9 months) and OS (22 vs 21 months). 41 Patients treated with doxorubicin compared with liposomal doxorubicin had higher rates of cardiotoxicity (26% vs 7%), alopecia (66% vs 20%), nausea (53% vs 37%), vomiting (31% vs 19%), and neutropenia (10% vs 4%) but had lower rates of palmar-plantar erythrodysesthesia (2% vs 48%), stomatitis (15% vs 22%), and mucositis (13% vs 23%). As a result of this trial, pegylated liposomal doxorubicin was established as a noninferior alternative to the other anthracyclines, especially in patients desiring less frequent drug administrations, significant accumulated anthracycline dosages, or a slightly different side effect profile. With regard to the management of cardiac toxicity in clinical practice, metastatic patients who are responding to and tolerating therapy but are approaching the upward limit of the cumulative anthracycline dose (ranging from 450 mg/m2 for doxorubicin to >900 mg/m2 for epirubicin) can be considered for the iron chelator dexrazoxane. By reducing the number of metal ions that complex with anthracyclines and subsequently decreasing the formation of superoxide radicals, this agent can be used to reduce the risk of anthracycline-induced cardiac damage.
Although there has only been a small amount of data suggesting a difference in treatment-related outcomes in the metastatic setting between single-agent anthracyclines and taxanes, a recent meta-analysis comparing the two classes of chemotherapies showed a modest superiority among anthracyclines, with a slightly improved ORR (38% vs 33%) and PFS (seven vs five months). 41 However, the strength and clinical applicability of these results were limited due to trial heterogeneity, which included differences in taxane administration schedules and varying patient inclusion/exclusion criteria (ie, patients treated with taxanes in the adjuvant setting were excluded).
Antimetabolites/others
Capecitabine, a 5-fluorouracil (5-FU) prodrug and pyrimidine antimetabolite that inhibits thymidylate synthetase, is an oral chemotherapy agent administered on a two-week-on/one-week-off schedule.42–44 Due to the ease of administration and comparable efficacy and tolerability compared to other agents, it is commonly used in the first-line metastatic setting. Compared to many other agents used in the treatment of mBC, capecitabine has a greater degree of CNS penetration and can be used in the setting of liver dysfunction. Capecitabine is also associated with a unique side effect profile, including minimal alopecia and neuropathy, but sometimes with dose-limiting adverse effects, including palmar-plantar erythrodysesthesia and diarrhea. 44 Two multicenter Phase II trials, one of which used cyclophosphamide, methotrexate, and 5-FU (CMF) as a comparison arm, looked at capecitabine in the first-line mBC (prior adjuvant treatment with anthracycline and taxane) and not only demonstrated its comparative superiority but also reported an ORR between 28% and 30%, a TTP between four and five months, and a median OS between 15 and 20 months.43,44
Although less commonly used, single-agent gemcitabine also has activity in mBC45–47 but appears to be associated with an inferior TTP and OS when compared to weekly epirubicin. A pyrimidine antimetabolite that inhibits DNA synthesis, gemcitabine, is associated with limited side effects, including mild alopecia and gastrointestinal toxicity, such as constipation. Thrombocytopenia is common in pretreated patients and can be a severe dose-limiting adverse effect. Another less commonly used single agent in the treatment of mBC is the topoisomerase II inhibitor etoposide, which is administered orally daily for days 1–21 of a 28-day cycle. Although it produces an ORR of ~30% in heavily pretreated patients, it can also be associated with significant hematologic and gastrointestinal toxicities.48,49
Combination Chemotherapy
Combination chemotherapy is uncommonly used in the treatment of mBC, but select combinations have been shown to be effective in producing swifter and more significant responses compared with single-agent chemotherapy. Notably, at the expense of tolerability and to our knowledge, there are no data demonstrating an improvement in patient survival using combination rather than single-agent therapy prescribed in a sequential fashion. However, several combinations of systemic chemotherapy have been associated with improved survival outcomes in the metastatic setting compared with nonsequential single-agent therapy alone. These combinations include capecitabine and docetaxel (vs docetaxel alone; OS: 14.5 vs 11.5 months), gemcitabine and paclitaxel (vs paclitaxel alone; OS: 18.6 vs 15.8 months), and capecitabine and ixabepilone (vs capecitabine alone; PFS: 5.8 vs 4.2 months).
In a large randomized trial, 700 patients with mBC were randomized to receive doxorubicin plus paclitaxel, doxorubicin, or paclitaxel with crossover allowed upon progression. The combination of doxorubicin plus paclitaxel resulted in a greater ORR (47% vs 36% vs 34%) and a longer TTP (eight vs six vs six months) but produced no difference in OS (22 vs 19 vs 22 months).
50
A recent meta-analysis analyzed 43 trials (9,742 women) that primarily included anthracycline- and/or taxane-based combination chemotherapy trials and with ~55% treatment naive in the metastatic setting. The analysis showed an improvement in OS with combination compared with single-agent therapy (hazard ratio [HR] 0.88, 95% confidence interval [CI] 0.83–0.93,
Although more toxic than sequential single-agent treatment or nonanthracycline-containing combinations, anthracycline-based chemotherapy regimens are associated with an ORR of ~60% in previously untreated patients with mBC. In a meta-analysis of eight trials and 3,000 patients looking at taxane plus anthracycline regimens compared with nontaxane anthracycline-containing combinations, an anthracycline plus taxane combination resulted in a higher ORR (57% vs 46%) but no difference in OS. 31 Other anthracycline-based regimens include doxorubicin plus cyclophosphamide (ORR: 47%–54%, OS: 21.5 months), 51 epirubicin with cyclophosphamide and fluorouracil (ORR: 45%–55%, OS: 18.9 months), 52 doxorubicin with docetaxel plus cyclophosphamide (ORR: 77%, OS: 20.5 months), 53 and doxorubicin plus paclitaxel or docetaxel (ORR: 40%, OS: 20.6 months). 54
For patients who are not candidates for anthracyclines, taxane-based regimens are typically administered. Given the lack of complete cross-resistance between paclitaxel and docetaxel, the alternative agent to the one used in the adjuvant setting is typically administered. For chemotherapy-naive patients, the choice between taxanes is commonly based on the toxicity profiles. Gemcitabine can be administered with paclitaxel (ORR: 41%) 55 or at a lower dose when combined with docetaxel (ORR: 43%). 56 Although these regimens have not been compared head-to-head, previous single-agent experience suggests that the combination of gemcitabine plus docetaxel produces greater hematologic toxicities. Another commonly used taxane-based combination includes capecitabine and docetaxel every 21 days, which is associated with an ORR of 42%, improves OS when compared with single-agent docetaxel, and demonstrates comparable efficacy with gemcitabine plus docetaxel (PFS: 8.2 vs 8.2 months). 57 Meanwhile, ixabepilone in combination with capecitabine has an ORR of 35%. Although rarely administered for mBC due to its inferiority to single-agent capecitabine (ORR: 20% vs 20%; OS: 18 vs 22 months), the previously mentioned CMF combination can be used in patients who cannot tolerate the toxicity or oral administration of capecitabine. 58
Most breast cancers that arise in the setting of a germline mutation in the tumor suppressor breast cancer susceptibility gene 1 (
Future Directions
The epidermal growth factor receptor (EGFR) is commonly overexpressed in mTNBC. However, three Phase II clinical trials evaluating the efficacy of the anti-EGFR monoclonal antibody cetuximab in combination with chemotherapy demonstrated only a modest beneficial treatment effect.66–68 Although angiogenesis inhibitors (ie, bevacizumab) have shown to improve OS in other cancer types and marginally improve PFS in mBC, there have not been prospective data demonstrating an improvement in OS among patients with mTNBC.69–71
Clinical trials looking at targeted agents and chemotherapeutic, hormonal, immune strategies in metastatic triple-negative breast cancer (mTNBC). 72

Gene expression profiling studies have suggested that mTNBC might be preferentially sensitive to the inhibition of the protooncogene Src. Although combination therapy trials are currently ongoing, dasatinib, a potent orally available inhibitor of the Src family kinase, was tested in an early phase study of mTNBC and yielded a CBR of 9.2%. 78 Due to its activity in the setting of ER/PR-positive tumors that have developed hormone resistance, there is a developing interest in DNA methyltransferase and histone deacetylase (HDAC) inhibitors in mTNBC as preclinical studies have suggested that the inhibition of these mechanisms could result in re-expression of a functional ER mRNA and protein. Currently, clinical trials evaluating the HDAC inhibitor vorinostat in combination with chemotherapy are underway to test the drug's efficacy among patients with mTNBC. 79
Several preclinical and early phase studies have implicated other possible chemotherapeutic strategies and targetable pathways in mTNBC, for which clinical trials are currently underway (Table 2 and Fig. 3).72,80–97 One of these targets is the androgen receptor, for which there have been some data on its ability to predict chemotherapy sensitivity and prognosticate patient outcomes.98–100 Although there have only been preclinical and early phase studies looking at androgen receptor blockers as a targeted agent in mTNBC, larger clinical trials are currently ongoing.
72
Despite the widespread use and success among patients with other tumor types, there is limited data to suggest a therapeutic benefit from immune checkpoint inhibitors, vaccines, or chimeric antigen receptor T-cell therapy in mBC.
101
Schematic overview of the therapeutic targets that are currently being tested in clinical trials among patients with mTNBC.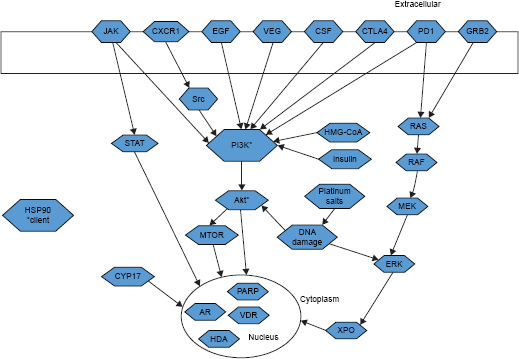
Conclusion
The management of patients with mTNBC can be quite complex and often requires consideration of many different patient-, tumor-, and therapy-related factors in order to tailor the treatment and optimize the care. Although there have been many new agents approved for mBC over the past 20 years, the treatment options for the subset of patients with mTNBC remain somewhat limited. It is unclear how much the difference in survival among these patients is secondary to the inherent aggressive biology of mTNBC, rather than the availability of effective treatment. Nonetheless, more research is needed to further understand this complex disease and its involved genomic signatures and signaling pathways, with the ultimate goal of improving the long-term outcomes of this subset of patients compared to that of other patients with mBC.
Author Contributions
Conceived and designed the experiments: SBZ, HT, and KG. Analyzed the data: SBZ, HT, and KG. Wrote the first draft of the manuscript: SBZ, HT, and KG. Contributed to the writing of the manuscript: SBZ, HT, and KG. Agree with manuscript results and conclusions: SBZ, HT, and KG. Jointly developed the structure and arguments for the paper: SBZ, HT, and KG. Made critical revisions and approved final version: SBZ, HT, and KG. All authors reviewed and approved of the final manuscript.