
Abstract
In the past decades, the oncogenic role of fibroblast growth factor receptor 2 has been demonstrated in a number of cancer types. However, studies have reported contradictory findings concerning the correlation between fibroblast growth factor receptor 2 expression and prognosis in solid tumors. To address this discrepancy, we performed a meta-analysis with 18 published studies (2975 patients) retrieved from PubMed, EMBASE, and Web of science. Data were extracted and computed into odds ratios. The results showed that fibroblast growth factor receptor 2 overexpression was significantly associated with decreased 3-year overall survival (odds ratio = 1.93, 95% confidence interval: 1.30–2.85, p = 0.001) and 5-year overall survival (odds ratio = 1.62, 95% confidence interval: 1.07–2.44, p = 0.02) in patients with solid tumors. Subgroup analysis revealed that high fibroblast growth factor receptor 2 expression was also associated with poor prognosis of gastric cancer, hepatocellular carcinoma, and esophageal cancer, but not correlated with pancreatic cancer. In conclusion, fibroblast growth factor receptor 2 overexpression is correlated with decreased survival in most solid tumors, suggesting that the expression status of fibroblast growth factor receptor 2 is a valuable prognostic biomarker and a novel therapeutic target in human solid tumors.
Introduction
Recently, fibroblast growth factors (FGFs) and fibroblast growth factor receptors (FGFRs) have become a research hotspot; FGFRs are members of the receptor tyrosine kinase family and encode transmembrane tyrosine kinase receptors which are involved in signaling by interacting with FGFs. The regulation of the FGF signaling pathway is critical for normal human growth; indeed, genetic alterations of FGFRs reportedly enhance downstream signaling, which are related to cell proliferation, differentiation and migration, and fundamental to embryonic development, wound healing, and angiogenesis.1–5 The FGFR2 gene is located on chromosome 10q26 and functions as FGFR; it is activated by ligand binding, which results in dimerization and autophosphorylation of the endocellular domains of receptors and receptor-related adaptors. 6 Keratinocyte growth factor receptor (KGFR) is mainly found in epithelial cells throughout the gastrointestinal tract, and activated by keratinocyte growth factor (KGF), which is predominantly synthesized by mesenchymal cells and also known as FGFR2 IIIb. 7 The K-sam gene, originally identified in the gastric cancer KATO-III cell line, is usually amplified in the malignant phenotype of gastric cancer such as poorly differentiated adenocarcinoma, mucinous adenocarcinoma, and signet-ring cell carcinoma.8,9 KGFR and K-sam are encoded by the FGFR2 gene.7,10
Multiple studies have assessed the relationship between FGFR2 overexpression and human solid tumors, including gastric cancer,11–18 pancreatic cancer,19–22 esophageal cancer,23,24 hepatocellular carcinoma,25,26 colorectal cancer, 27 breast cancer, 28 and glioma. 29 However, the prognostic value of FGFR2 overexpression in some human solid tumors is inconclusive, and no consensus has been reached. Studies suggested that high FGFR2 level is associated with favorable outcome in patients with gastric cancer, 18 pancreatic cancer, 19 and glioma. 29
Accordingly, we performed a comprehensive meta-analysis to appraise the prognostic value of FGFR2 overexpression in human solid tumors. The aim of this meta-analysis was to assess the association of high FGFR2 expression with survival in human solid tumors, illustrating the clinical value of FGFR2 as a potential therapeutic target and prognostic indicator for solid tumor patients.
Materials and methods
This meta-analysis was performed according to the statement for reporting systematic reviews and meta-analyses. 30 Previously published studies were summarized and analyzed in this study; therefore, ethics approval was not necessary.
Search strategy
A thorough search of PubMed, Web of Science, and EMBASE was performed to retrieve studies measuring FGFR2 expression and survival in patients with solid tumors from 1996 to January 2017. The search terms included “FGFR2” or “Fibroblast growth factor receptor 2” or “KFFR” or “Keratinocyte growth factor receptor” or “K-sam,” or “Fibroblast growth factor receptor 2,” and “neoplasms” or “cancer” or “tumor” or “malignancy” or “carcinoma” or “survival” or “prognosis.” Results were restricted to human studies of solid tumors. A total of 1812 entries were identified. Inclusion criteria were measurement of FGFR2 by immunohistochemistry (IHC) or fluorescent in situ hybridization (FISH), availability of survival data for at least 3 years, and English language for publication. The reference lists of relevant articles were scanned and additional studies of potential interest were retrieved for further analysis. Inter-reviewer agreement was assessed by the Cohen’s kappa coefficient. Any disagreement between assessors was resolved by consulting a third investigator until a final consensus was reached.
Endpoints of interest
The primary endpoints were OS at 3 and 5 years. Tumors were classified by FGFR2 expression status, using the cut-offs defined in various studies.
Data collection process and quality assessment
The included studies were assessed independently by two investigators (G.L. and Z.J.H.): references, country, cancer type, patient number, median age, gender, follow-up duration, and cut-off value for FGFR2 positivity. OS data were extracted from the tables or Kaplan–Meier curves for both FGFR2 negative and positive groups. The reports included in this meta-analysis were all cohort studies. To identify high-quality studies, each publication was scored based on the Newcastle–Ottawa (NOS) system. 31 This scale ranges from 0 to 9 stars, with studies showing a score ⩾6 considered to be methodologically sound. A consensus NOS score for each item was achieved by discussion.
Data synthesis
The relative survival rates at 3 and 5 years, respectively, between the experimental and control groups were expressed as odds ratios (ORs) and 95% confidence intervals (CIs). Sensitivity analysis was performed for different analytical methods and cut-offs to define FGFR2 expression and NOS score for quality evaluation of the included studies.
Statistical analysis
Data were extracted from the primary publications and analyzed with the RevMan 5.3 analysis software (Cochrane Collaboration, Copenhagen, Denmark). OR estimates were weighted and pooled using the Mantel—Haenszel random-effect model. Statistical heterogeneity was evaluated by Cochran’s Q and I2 statistics. Differences between the subgroups were assessed in accordance with the Cochrane Handbook for Systematic Reviews of Interventions. Two-sided p < 0.05 was considered statistically significant.
Results
Search results and study characteristics
A total of 18 studies with a total of 2975 patients were included in this meta-analysis (Figure 1). The main characteristics of the included studies are shown in Tables 1 and 2. Eight studies evaluated gastric cancer,11–18 three assessed pancreatic cancer,19,20,22 two focused on esophageal cancer23,24 and hepatocellular carcinoma,25,26 and one each evaluated colorectal cancer, 27 breast cancer, 28 and glioma. 29 The studies were conducted in six countries, including Japan, China, Korea, America, Singapore, and the United Kingdom, and published between 1996 and 2016.

Flow diagram of the meta-analysis process.
Characteristics of the included studies.
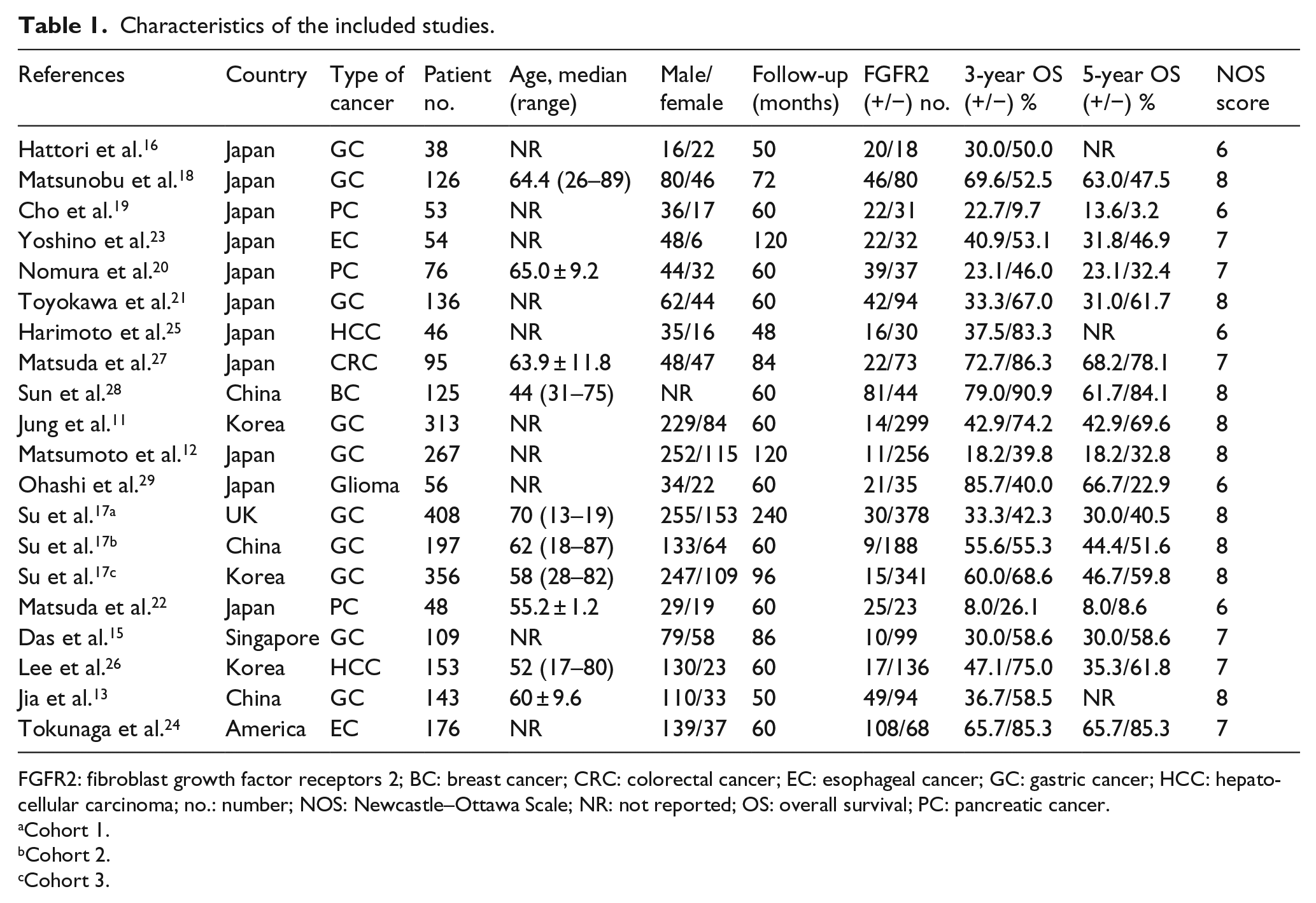
FGFR2: fibroblast growth factor receptors 2; BC: breast cancer; CRC: colorectal cancer; EC: esophageal cancer; GC: gastric cancer; HCC: hepatocellular carcinoma; no.: number; NOS: Newcastle–Ottawa Scale; NR: not reported; OS: overall survival; PC: pancreatic cancer.
Cohort 1.
Cohort 2.
Cohort 3.
Evaluation the cut-off value for FGFR2 by IHC and FISH in the selected studies.

FGFR2: fibroblast growth factor receptors 2; BC: breast cancer; CEP10: chromosome enumeration probe 10; CRC: colorectal cancer; EC: esophageal cancer; FISH: fluorescence in situ hybridization; GC: gastric cancer; HCC: hepatocellular carcinoma; IHC: immunohistochemistry; no.: number; NR: not reported; PC: pancreatic cancer; IRS: Immunoreactive Score.
Cohort 1.
Cohort 2.
Cohort 3.
Association of FGFR2 with OS
There were 18 studies reporting 3-year OS data. Results demonstrated that FGFR2 overexpression in the human tumor tissue was associated with decreased survival of solid tumor patients (OR = 1.93, 95% CI: 1.30–2.85, p = 0.001) (Figure 2). There was significant heterogeneity among the 18 studies included (p = 0.0001, I2 = 62%); therefore, we proceeded to perform a subgroup analysis to assess whether different cancer types lead to this heterogeneity. Eight reports provided 3-year OS data for gastric cancer, three for pancreatic cancer, two for hepatocellular carcinoma, and two for esophageal cancer. In a stratified analysis by solid tumor type, FGFR2 overexpression was associated with unfavorable clinical outcome in gastric cancer (OR = 1.90, 95% CI: 1.14–3.07, p = 0.009) (Figure 3(a)), hepatocellular carcinoma (OR = 4.67, 95% CI: 1.99–10.92, p = 0.0004) (Figure 3(c)), and esophageal cancer (OR = 2.46, 95% CI: 1.30–4.65, p = 0.006) (Figure 3(d)). However, no association was found between FGFR2 overexpression and 3-year OS in pancreatic cancer (OR = 1.66, 95% CI: 0.42–6.53, p = 0.47) (Figure 3(b)).

The association between expression level of FGFR2 and 3-year overall survival (OS).

Subgroup analysis of 3-year OS by FGFR2 expression in different tumor types: (a) gastric cancer, (b) pancreatic cancer, (c) hepatocellular carcinoma, and (d) esophageal cancer.
There were 15 studies reporting 5-year OS data. Results indicated that FGFR2 overexpression in the human tumor tissue was associated with reduced survival of solid tumor patients (OR = 1.62, 95% CI: 1.07–2.44, p = 0.02) (Figure 4). There was significant heterogeneity among the 15 studies included (p = 0.0009, I2 = 59%); therefore, we performed a subgroup analysis to explore whether different cancer types lead to this heterogeneity. Six reports provided 5-year OS data for gastric cancer, three for pancreatic cancer, and two for esophageal cancer. In a stratified analysis by solid tumor type, FGFR2 overexpression was associated with unfavorable clinical outcome of gastric cancer (OR = 1.77, 95% CI: 1.04–3.03, p = 0.04) (Figure 5(a)) and esophageal cancer (OR = 2.60, 95% CI: 1.37–4.94, p = 0.006) (Figure 5(c)). However, there was no association of FGFR2 overexpression with 5-year OS in pancreatic cancer (OR = 1.04, 95% CI: 0.37–2.91, p = 0.94) (Figure 5(b)).
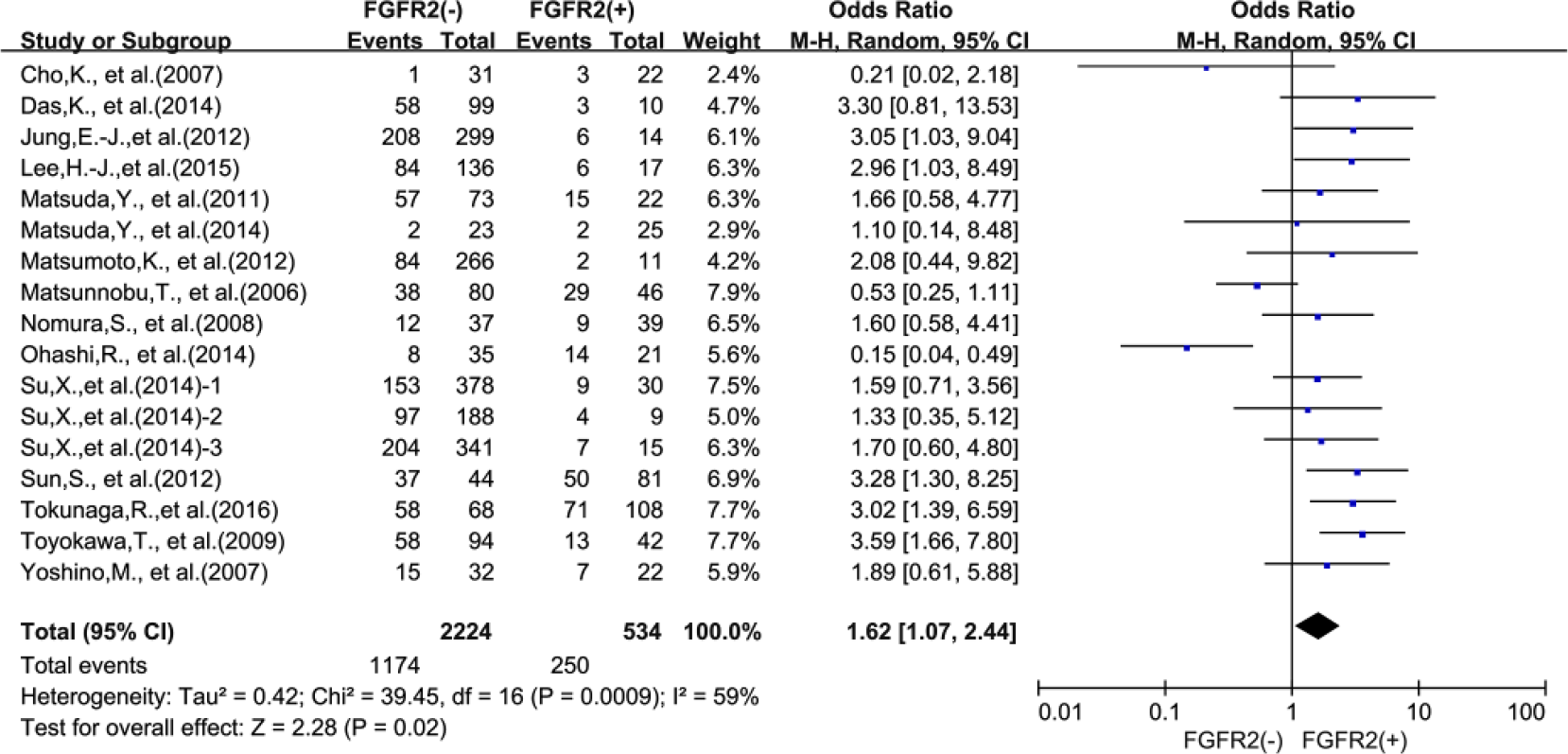
The association between expression level of FGFR2 and 5-year overall survival (OS).

Subgroup analysis of 5-year OS by FGFR2 expression in different tumor type: (a) gastric cancer, (b) pancreatic cancer, and (c) esophageal cancer.
Publication bias
Funnel plot analysis suggested that there was no statistical evidence for publication bias in this meta-analysis (data not shown).
Discussion
Over the past decades, researchers have invested much effort to identify new prognostic markers for improved clinical decision-making regarding therapy and outcomes. The prognostic value of FGFR2 expression has been investigated extensively in multiplies cancers. However, the prognostic value of FGFR2 overexpression in solid tumors remains controversial, as existing studies are often small with conflicting results. By summarizing the findings of published studies, we aimed to evaluate the indicated relationship to provide useful information for clinical decision-making in solid tumors.
To our knowledge, this is the first systematic review to provide an in-depth analysis of FGFR2 overexpression in relation with OS of patients with solid tumors. We systematically evaluated survival data of 2975 solid tumor patients included in 18 different studies. Our meta-analysis suggested that FGFR2 overexpression was a biomarker of reduced prognosis in human solid tumors, with similar 3- and 5-year OS results. Concerning solid tumor types, high FGFR2 expression in tumor tissues was associated with poor OS in gastric cancer, hepatocellular carcinoma, and esophageal cancer, but not pancreatic cancer. Taken together, these findings suggested that elevated FGFR2 expression is correlated with poor survival in most solid tumors. The inconsistent results among different solid tumor types indicate that further studies are warranted to clarify the underlying mechanism and role of FGFR2 in the pathogenesis of human solid tumors, as well as its prognostic value.
This meta-analysis has several pivotal implications. First, it revealed that FGFR2 expression is correlated to unfavorable outcome in various human solid tumors, indicating that FGFR2 may be a novel therapeutic target. Second, a subgroup of tumors with high FGFR2 expression in tumor tissues were shown to have worse OS, including gastric cancer, hepatocellular carcinoma, and esophageal cancer. Finally, this study highlights the potential clinical application of FGFR2 as a valuable prognostic biomarker.
However, this meta-analysis also had some limitations. First, small sample studies with negative results may not have been published, resulting in publication bias. Second, different analysis methods and cut-off values for evaluating FGFR2 overexpression were inconsistent among the included reports. Third, English language, as one of the constraints for this meta-analysis, rule out other language studies lead to analysis is incomplete date. Finally, the substantial heterogeneity observed among studies could not be completely interpreted although appropriate analytical methods with random effects models were used.
In summary, this meta-analysis indicates that FGFR2 overexpression is associated with poor OS in most human solid tumors, suggesting that FGFR2 is a valuable prognostic indicator and a novel therapeutic target for human solid tumors.
Footnotes
Acknowledgements
G.L. and D.X. contributed equally to this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the Science and Technology Project of Natural Science Foundation of Fujian Province (no. 2016J01639), the Medical Innovations Topic in Fujian Province (no. 2016-CXB-8, 2012-CXB-29) and Project of Xiamen Scientific and Technological Plan (no. 3502Z20134011).