
Abstract
Purpose
Agarose macrobeads containing mouse renal adenocarcinoma cells (RMBs) release factors, suppressing the growth of cancer cells and prolonging survival in spontaneous or induced tumor animals, mediated, in part, by increased levels of myocyte-enhancing factor (MEF2D) via EGFR-and AKT-signaling pathways. The primary objective of this study was to determine the safety of RMBs in advanced, treatment-resistant metastatic cancers, and then its efficacy (survival), which is the secondary objective.
Methods
Thirty-one patients underwent up to four intraperitoneal implantations of RMBs (8 or 16 macrobeads/kg) via laparoscopy in this single-arm trial (FDA BB-IND 10091; NCT 00283075). Serial physical examinations, laboratory testing, and PET-CT imaging were performed before and three months after each implant.
Results
RMBs were well tolerated at both dose levels (mean 660.9 per implant). AEs were (Grade 1/2) with no treatment-related SAEs.
Conclusion
The data support the safety of RMB therapy in advanced-malignancy patients, and the preliminary evidence for their potential efficacy is encouraging. A Phase 2 efficacy trial is ongoing.
Keywords
Introduction
We have shown in our laboratory that mouse renal adenocarcinoma (RENCA) cells embedded in an agarose matrix and surrounded by an outer layer of higher-concentration agarose (forming a roughly spherical bead 6–8 mm in diameter, hereafter called R MB) release factors that inhibit the proliferation of cancer cells of various types outside the macrobead both in vitro and in animal tumor models in the mouse, rat, cat, and dog.1,2 Our gene array studies comparing the freely growing RENCA cells with the freely growing cells exposed to R MB-conditioned media have shown that the embedding of the RENCA cells in the agarose macrobead causes changes in the gene expression patterns that are distinct from those seen in the cells exposed to the conditioned medium or the RMB themselves. The pattern of changes in the freely growing cells exposed to the R MB includes the downregulation of genes regulating DNA replication, angiogenesis, certain oncogenes (Hras), metalloproteinases, and immune defenses along with the upregulation of genes associated with differentiation and strikingly, with 100-fold upregulation of two genes associated with apoptosis, CHOPP, and GADD45.1,2 In other words, the RMB and the factors released by them are associated with the inhibition of neoplastic cell division, while at the same time, increasing programmed cell death. Recent work in our laboratory has shown that the mechanism by which the RMB achieves this effect is associated with, in significant part (estimated to be approximately 40%), increased levels of the transcription factor MEF2 via either or both an EGF receptor-mediated pathway and a P13/AKT pathway (unpublished data). Mass spectroscopic analysis of medium conditioned by exposure to the RMB has identified 10 likely candidate signals. The work to identify the critical signal or signals is ongoing.
This report summarizes the findings from a first-in-human Phase 1 study with intraperitoneal implantation of RMB as a cell-system anti-cancer therapy. The study's primary objective was to assess the feasibility, safety, and toxicity of this approach. Its secondary objective was to determine the preliminary efficacy in patients with advanced solid tumors.
Materials and Methods
Patient population
Eligible patients were males or females, 18 years and older, with histologically confirmed, epithelial-derived tumors and those who had the majority of their disease localized to the peritoneal cavity. All patients had previously failed the existing chemotherapeutic and/or targeted therapies and were being referred to a clinical trial because of the likelihood of their limited survival. Tumor types included renal, ovarian, pancreatic, colon, and gastric adenocarcinomas, hepatocellular carcinoma, and gastrointestinal lymphoma. Tumor size and burden were measured by PET-CT imaging modalities to provide the number and location of primary and metastatic lesions, as well as information on their metabolic activity. Other inclusion criteria included Eastern Cooperative Oncology Group 3 performance status of 0–1; adequate coagulation parameters; liver and renal function (serum creatinine of >1.5 mg/dL or creatinine clearance >60 cc/min).
Patients were excluded if they had surgical treatment or chemotherapy within three weeks of baseline evaluation; radiation therapy within four weeks of baseline evaluation; any condition (cardiovascular or other) resulting in unacceptably high anesthetic or surgical risk; extensive peritoneal carcinomatosis and/or more than minimal ascites; platelet counts of less than 100,000/mm3; pregnancy or the likelihood of becoming pregnant within the subsequent twelve months post implant; breastfeeding; significantly compromised liver function as evidenced by liver enzyme levels: aspartate aminotransferase >4 × the upper limit of normal (ULN), alanine aminotransferase >4 × ULN, albumin <3.0 mg/dL, prothrombin time >1.5 seconds X ULN, or a total bilirubin >1.5 × ULN; or cognitive impairment sufficient to render the patient incapable of giving informed consent.
Any known allergy to murine antigens or body tissues, or a history of any type of hypersensitivity reactions, hepatic blood flow abnormalities, and HIV-positive status was also considered exclusion criteria.
All patients completed a written informed consent for the study, which was approved by the Weill Cornell IRB and was conducted in accordance with the IRB policies, the principles of the Declaration of Helsinki and GCP guidelines.
Study design
The Phase 1, open-label, noncomparative study was designed to evaluate the safety and, preliminarily, the efficacy of RMB implantation in patients with advanced, treatment-resistant, epithelial-derived cancers. The study was open to all such cancers, primarily to those arising within intraperitoneal organs, but also included breast, prostate, and lung malignancies.
The RENCA macrobead (RMB)
RMB (6–8 mm in diameter) are composed of two concentric, nearly spherical agarose layers: the 4–6 mm inner core composed of 0.8%–1.0% agarose, and a 1–2 mm outer coating composed of 4.5%–5.0% agarose. The 150,000 ± 10% RENCA cells are embedded in the inner layer. Prior to implantation, the RMB are cultured in vitro (RPMI medium with 10% newborn calf serum) for 6–16 weeks, during which period ~99% of the original RENCA cells undergo apoptotic death, with the remaining 1% resulting in the selection of a stem cell–like subpopulation that, together with at least one other cell subpopulation of daughter cells and/or tumor-initiating cells, drive long-lasting colony formation. It is when the colonies have formed that the inhibitory effect of the cancer macrobead becomes measurable.
The surviving encapsulated cells are unable to escape from the inner agarose core and, over a period of several months, form individual tumor colonies that reach a maximal size and number within the growth-restricted macrobead core. Host peritoneal cells, such as phagocytes and macrophages, cannot penetrate because of the outer agarose layer, although molecules <100 kDa are able to migrate into and out of the macrobead. Following implantation, the macrobeads remain largely free-floating in the peritoneal cavity, where they produce and release numerous potentially tumor-inhibitory molecules that suppress freely growing animal and human cancer cells in vitro and in vivo without species or tumor-type (within a broad range of epithelial-derived tumors) specificity.
Treatment
The implantation of 22–44 RMB/kg body weight was found to be both safe and effective in dogs and cats. For humans, taking into consideration the differing metabolic rates of cats and dogs with those of humans, a dosage of 8 or 16 macrobeads/kg (approximately 600–1200 macrobeads/patient) was considered to be appropriate and consistent with the peritoneal cavity space available.
As this study was a first-of-a-kind approach in humans, the initial five patients were enrolled sequentially, and each was observed for at least three months for potentially unacceptable treatment-related toxicity before treatment of the next patient. The first five patients received implants of 8 RMB/kg, and the second five patients received 16 RMB/kg. Without any obvious difference in the responses induced, and with the concept that up to four such implants might be needed based on the experience in veterinary patients, patients 11–31 received the 8 RMB/kg dosage.
The RMB were prepared at the Rogosin Institute/Xenia Division, Xenia, OH. The implantation was conducted at the Rogosin Institute/New York-Presbyterian Hospital, New York, NY. The insertion of RMB into the peritoneal cavity was performed laparoscopically through two ports under general anesthesia–-a 5 mm port for the camera and a 12 mm port to deliver the macrobeads. The video camera enabled the surgeon to be certain that the RMBs were distributed evenly throughout the available space in the abdominal cavity, ensuring maximal surface area exposure to macrobead-secreted factors, while also reducing nutritional competition and thus promoting longer survival for the cells in the RMBs. The initially enrolled patients were observed in the hospital for 24–48 hours after surgery to ensure that there were no unexpected adverse events. Patients subsequently added to the series underwent the procedure entirely on an outpatient basis.
Assessment of safety and follow-up
Because of the novelty of the RMB therapy, multiple clinical, laboratory, and imaging parameters were assessed, both at baseline and at the post-implant protocol-specified visits on Days 3, 7, 14, 21, 28, 42, 53, 68, 83, 113, 143, and 173.
Physical examinations were done at each visit. Laboratory testing included metabolic, hematologic, inflammation, coagulation, hepatic (plus alkaline phosphatase, gamma-glutamyl transferase), cellular and humoral immune function, tumor markers (CEA and CA19-9) as well as circulating tumor cells, and positron emission tomography with non-contrast CT imaging (PET-CT) to evaluate tumor size, number, and metabolic activity ( 18 F-flourodeoxyglucose uptake (FDG)). Preoperative evaluations at baseline and on Day 90 after each implantation included the above tests plus a chest X-ray, electrocardiogram, and Doppler abdominal ultrasound where there was a suspicion of altered portal vein outflow.
Because a post-implant inflammatory response was expected, C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and CA125 levels were measured as markers of inflammation. In particular, CA 125 was used to monitor any potential inflammatory/irritative peritoneal or serosal surface reactions to the intraperitoneal placement of the RMB. Serum CA19-9 and CEA measurements were performed on all patients to further assess tumor response to RMB implantation. Tumor marker response was defined as at least a 20% decrease from baseline in CA 19-9 or CEA levels within the first 30 days after implant. It was also assessed at the following time points after each implantation, as applicable: Days 3, 7, 14, 21, 28, 42, 53, 68, 83, 113, 143, and 173.
Sample size determination
Since this was the first clinical study (open-label, noncomparative) performed using RMB, there was no prior clinical experience on which to base a sample-size calculation. Adverse Events percentages were calculated for the safety assessment, and overall survival (OS), for efficacy assessment.
Results
Patient characteristics
A total of 56 patients provided informed consent to participate in the study. Of these, 31 patients (16 females and 15 males) underwent RMB implantation. Patients were not considered evaluable unless they underwent an implantation procedure. The first patient was implanted on 6 April 2005, and the last patient was implanted on 11 January 2011. Twenty-seven patients had histologically proven, epithelial-derived tumors with the majority of their disease localized to either the peritoneal or thoracic cavity. Four patients had non-small-cell lung carcinoma. The baseline and demographic patient data are provided in Table 1.
Baseline demographic and clinical characteristics (N = 31).
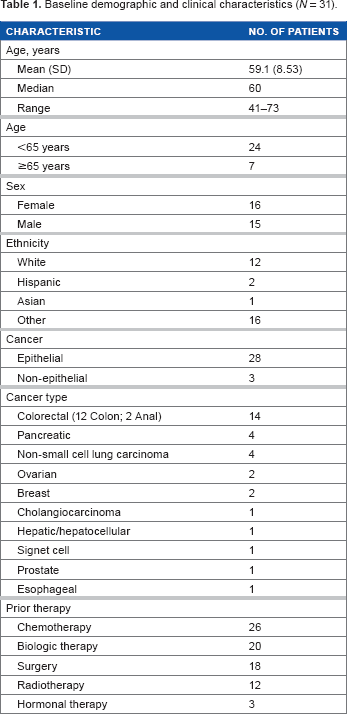
Fourteen of the 31 patients were diagnosed with colorectal adenocarcinoma and four patients with pancreatic adenocarcinoma. Other diagnoses included anal (squamous) carcinoma (2); carcinoma of the biliary tract (1); hepatocellular carcinoma (1); non-small cell lung carcinoma (4); gastric carcinoma (1); prostate carcinoma (1); ovarian carcinoma (2); breast carcinoma (2); and esophageal carcinoma (1). The mean (SD) number of RMB implanted was 661 (±297). Twenty-two (71%) patients had only one implantation; eight (26%) patients received two implants; and one (3%) patient received four implants.
Safety
Because this was a first-in-human study of a complex biological product involving cells from a non-human species, each patient's medical condition was carefully monitored by multiple means, as indicated in the Materials and methods section above. In total, 27 (87.1%) patients reported an adverse event during the study (Table 2). Adverse events occurring in more than 5% of all patients were fatigue (48.4%), pyrexia (35.5%), abdominal pain (25.8%), nausea, constipation, and night sweats (19.4% each), abdominal distention, vomiting, and pain (16.1% each), and inflammation, variable hyperhidrosis, and evanescent post-implant rash (12.9% each). Decreased appetite, consistent with the above symptoms, was common, but also transient. It did, however, result in weight loss, which ranged from 1 to 4 kg over the first 30 days, followed by weight stabilization and/or recovery in most cases. Taken together, these symptoms were consistent with the induction of a systemic inflammatory reaction (SIRS) by the surgical procedure itself, along with the introduction of the RMB (evident from rises in CRP, ESR, and CA 125, where it was not a tumor marker). It is important to emphasize that these were expected consequences of the procedure of implantation and not adverse events in the usual sense of unexpected, untoward events. They were mild and transitory in all cases, with many of the patients reporting that they had not felt better since their initial diagnosis and/or chemotherapy than they did after the SIRS resolved (generally in 7–14 days).
Treatment-related AEs occurring in >5% of all patients.
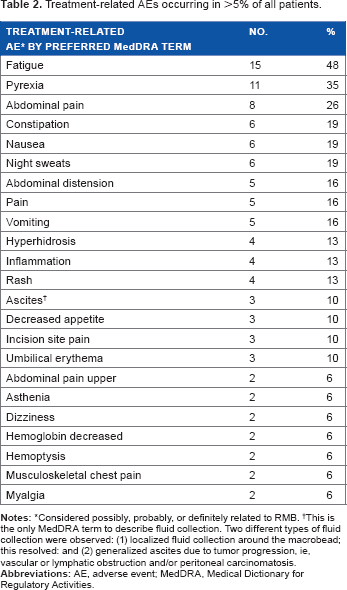
Considered possibly, probably, or definitely related to RMB.
This is the only MedDRA term to describe fluid collection. Two different types of fluid collection were observed: (1) localized fluid collection around the macrobead; this resolved: and (2) generalized ascites due to tumor progression, ie, vascular or lymphatic obstruction and/or peritoneal carcinomatosis.
Accumulation of ascites in patients, such as those with pancreatic or ovarian cancer, produced a gain in weight that signaled progressive disease. The majority of the adverse events occurred in the days immediately after implant through Day 14. All patients ultimately died from disease progression (n = 28) or due to adverse events associated with the malignancy itself or due to other comorbidities unrelated to the RMB treatment (n = 3). No deaths were judged to have occurred as a complication of macrobead therapy.
Overall, there were no persistent, clinically significant changes in the laboratory findings attributable to the RMB or the implantation procedure itself. Clinical laboratory changes directly attributable to the macrobeads included an initial postoperative SIRS to their intraperitoneal placement and, of course, the laparoscopic surgical procedure itself. These findings included elevations in CRP, ESR, and CA-125; a decrease in serum albumin levels; a small increase in INR (to 1.2); and an increase in IL-6 (see paragraph below). In the two-dose cohorts (8 or 16 RMB/kg) implanted, no dose limiting toxicities were observed, indicating that the maximum tolerated dose was not reached.
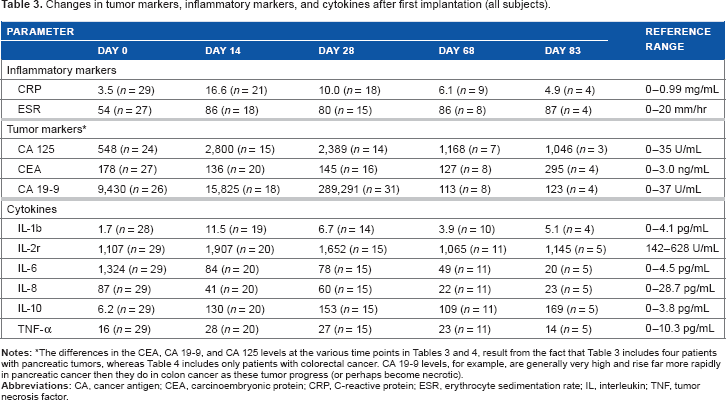
With regard to the post-implant inflammatory response, as noted in Table 3, the median increases from baseline in CRP serum levels were seen beginning Day 14, with a gradual return to near-baseline values by Day 60 following the first implantation. Median increases from baseline in ESR were also seen beginning Day 14 and the ESR remained elevated through Day 60 after the first implantation. The median CA-125 value at baseline was elevated (41.80 U/mL). Median increases from baseline were observed through Day 83 following implantation.
Changes in tumor markers, inflammatory markers, and cytokines after first implantation (all subjects).
Platelet counts were also followed as an indicator of SIRS. The counts uniformly increased in all patients, although the magnitude of the increase varied from a factor of 1.2–3 times baseline. All such increases were transient, and they were not associated with any clinical findings. No patient experienced a decrease in platelet count from that at baseline.
Finally, with respect to the inflammatory process, serum levels of albumin decreased transiently following RMB implantation. Median decreases by Day 14 were of the order of 0.5 g/dL. Recovery of the serum albumin level at or near baseline levels occurred by Day 30. Consistent with the decrease in serum albumin levels were decreases in the serum calcium levels, which maintained normal free serum calcium levels.
Cytokines patterns, including those for interleukins IL-1B, IL-2R, IL-6, IL-8, IL-10, tumor necrosis factor-alpha (TNF-α), and lipid binding protein, were analyzed for all patients irrespective of tumor type, and separately for the 12 patients with colorectal cancer. For the colorectal cancer patients, the median value for IL6 increased rapidly after implantation and then declined, although it remained elevated above baseline through Day 90 (baseline, 8.1 pg/mL; Day 14, 29.8; Day 28, 66.2; Day 60, 17.8; Day 90, 18.3). The median IL-10 level increased markedly, although more slowly than IL-6, from a baseline value and then declined significantly. Its level also remained above the baseline value at Day 90 (baseline, 1.2 pg/mL; Day 14, 9.7; Day 28, 33.4; Day 60, 53.3; Day 90, 12.2; see also Table 4).
Changes in tumor markers, inflammatory markers, and cytokines after first implantation (colorectal cancer subject n = 14).
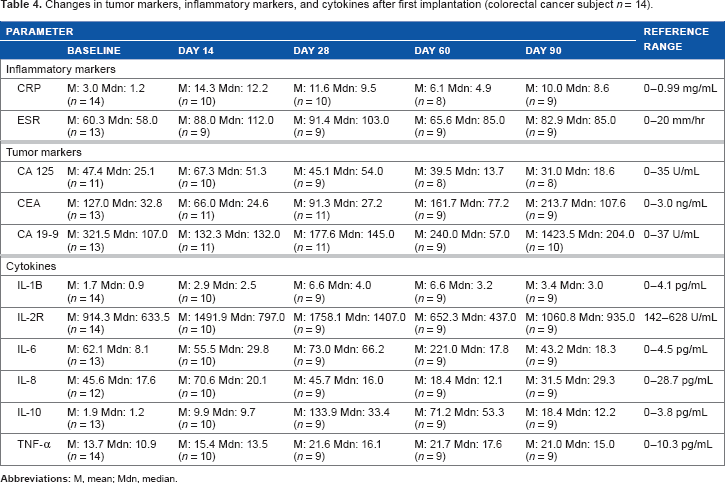
Regarding other cytokines (Table 4), a similar pattern of increases occurred after implantation, although the rise and fall in levels were less dramatic for both TNF-α and IL-2R. The median value for IL-1B increased from baseline to Day 14 followed by a gradual decrease at Day 90 with all median values remaining within the normal range. The median value for IL-2R more than doubled from baseline to Day 28; median values then decreased, but the value was actually higher than baseline at Day 90 (baseline, 633.5 pg/mL; Day 90, 935.0).
The median value for IL-8 showed small changes from baseline (17.6 pg/mL), with the lowest median value (12.1 pg/mL) reported on Day 60 and the highest median values observed on Day 14 and Day 68 (20.1 and 16.0 pg/mL, respectively), and Day 90 (29.3 pg/mL). The median value for TNF-α showed an increase from baseline to Day 60; median values at subsequent time points gradually decreased but remained elevated above baseline and/or the normal range.
Both cellular and humoral immune parameters were assessed at baseline and at monthly intervals thereafter. There were no consistent changes in the baseline values of either NK cell activity or immunoglobulin patterns at any time point following macrobead implantation. The mean immunoglobulin values over the measurement period were as follows: IgG–-1,100 mg/dL [ref. range 620-1,400 mg/dL]; IgA–-280 mg/dL [ref. range 80-360 mg/dL]; IgM–-100 mg/dL [ref. range 50-300 mg/dL]; and IgE–-1,400 mg/dL [ref. range 694-1618 mg/dL]. These values showed only minor variability over the course of the 413-day period during which the patients in the Phase 1 study were followed. In some patients, there were transient elevations in IgE, but there was no change in hypersensitivity reactions as measured by a standardized mouse antigen skin test, and so no.
With regard to NK cell activity, the patterns again indicated no suppression of activity after one or more implants and over the total follow-up period (maximum for one patient) of 413 days. There were transient increases of variable magnitude after the implants, but there was never an indication of decreased activity (transient or otherwise). The mean activity over the follow-up period was 20 LU30 (lytic units) with the normal range being 7-125 LU.
There were no clinically significant or consistent changes attributable to the RMB implantation in metabolic parameters, including electrolytes, renal function (creatinine, BUN), or liver function (aspartate aminotransaminase, alanine aminotransaminase) with the exception of the albumin level mentioned above.
Patients were monitored for an allergic reaction to the implanted agarose or the antigen present in the mouse RENCA cells in the macrobead. All patients were required to show no reaction to mouse epidermal antigens, applied as a skin-scratch test, at baseline and prior to any subsequent implantation. No reactions were observed in any individual at any time. However, four patients exhibited transient (maximum duration of 24 hours) urticarial rashes and/or erythema in the area around the abdominal incisions immediately following the implantation. Eosinophilia, again transient, was documented in two patients after RMB placement.
Because of the presence of an ecotropic variant of the murine leukemia virus (eMuLV) in the mouse RENCA cells, a serum specimen for each patient was collected at baseline and at each subsequent protocol visit to check for the transmission of and/or infection with this virus (SGS Vitrology, Glasgow, UK).
There was no real-time polymerase chain reaction or clinical evidence for transmission during or infection by ecotropic variant of the murine leukemia virus (eMuLV) in any patient at any time during a follow-up period, which for one of our patients was 3.6 years following implantation with RMB.
A different but important approach to the assessment of patient safety relevant to the macrobead incorporated the EORTC Quality of Life Scale, 4 the Karnofsky Performance Status, 5 and self-reporting by each patient at home during intervals between protocol visits. At baseline, the median Karnofsky score was 90.0 points for all patients: Three of the 21 patients (14%) showed improvement from baseline at ≥1 time point during the study, and eight of 21 patients (38%) had a best status of no change from baseline.
What is not reflected in the formal scale data is that patients in the Phase 1 trial frequently reported a return to physical activity levels not achievable during chemotherapy, and some even returned to full-time work. For example, Patient 1 took up a busy schedule of long automobile travel to visit his children who lived throughout the northeastern United States. Patient 26, who ultimately underwent four RMB implants, resumed work as a legal assistant within a week after her first implant and continued to work for the next 18 months, missing only one or two work days after each implant. Patient 38 went back to full-time work, managing an international literary agency.
Finally, with regard to the assessment of the safety of the RMB, five patients provided voluntary informed consent to a postmortem examination as a component of their participation in the Phase 1 macrobead protocol. Tumor types represented were hepatocellular carcinoma (1) and metastatic colorectal cancer (4). Tumor necrosis was a prominent finding described in all five patients. Additional findings reported by the independent team of pathologists performing these examinations included (1) frequent opacification with absence of visible colonies in most (largely intact) macrobeads at three months or longer periods of implantation; (2) entrapment of some RMB by the omentum; and (3) variable degrees of mild adhesion formation without evidence of interference with intra-abdominal organ function except that produced by the metastatic cancer itself. Overall, there were no findings of clinically significant adverse effects of the RMB.
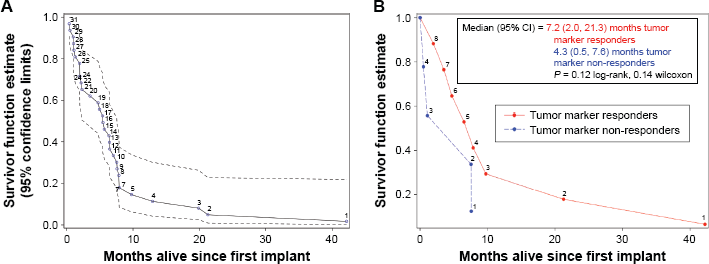
Overall survival. The median OS for the thirty-one patients who received at least one implant, regardless of tumor type, was 5.4 months (95% confidence interval [CI]: 2.2–7.0 months; Fig. 1A)]. Median OS was 7.0 months (95% CI: 1.1–9.7 months) for patients with colorectal cancer (Fig. 1B), 1.1 months (95% CI: 1.0–2.2 months) for pancreatic cancer, and 5.7 months (95% CI: 2.0–7.0 months) for the other primary cancer types.
(
Tumor markers
Serum CA19-9 (normal range, 0 to 37 U/mL) and CEA (normal range, 0–3.0 ng/L) measurements were performed on all subjects to determine tumor response to RENCA macrobead implantation (Tables 3 and 4).
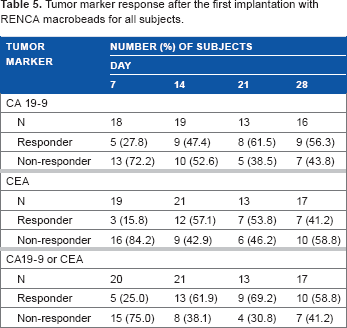
The proportion of subjects who had a tumor marker response with regard to either CA19-9 or CEA was greater than 50% at Days 14, 21, and 28 after the first implantation with RMB. The response rate was nominally higher for CA 19-9 compared with CEA at most time points (Table 5).
Tumor marker response after the first implantation with RENCA macrobeads for all subjects.
Of the eight subjects who had two implantations, tumor response with regard to CA 19-9 was noted for two of them at Days 14, 21, and 28 after the second implantation. With regard to CEA, tumor response was noted for one of them at Days 14 and 21 after the second implantation.
One subject had a third implantation and had a tumor response at Day 14 (CA 19-9). The median CA 19-9 value at baseline was elevated (48.0 U/mL), and small median decreases were generally observed through Day 42 after the first implantation. The median CEA value at baseline was elevated (27 ng/mL) and appeared to be relatively stable from Day 14 to Day 68.
One interesting and potentially important feature of the tumor marker data is that occasional transient rapid rises in either CA19-9 or CEA were observed. These usually occurred in parallel with increases and decreases in lactate dehydrogenase levels, suggesting tumor cell damage and release of otherwise intracellular tumor markers.
It is interesting to note that the mean and median values of CA 125 in the colorectal patients were relatively low at baseline, increased modestly and transiently after RMB implantation, and actually decreased by Day 90. This finding was consistent with the low prevalence on peritoneal spread in these patients.
Attempts to evaluate circulating tumor cells using CellSearch® were also made in all the Phase 1 trial patients both before and after RMB implantation. Frequent clumping of the cells limited the reliability and utility of this assay. Beyond that, results, such as a very high level of such cells (>100), suggesting either advancing disease or a test-system artifact, often could not be interpreted. 6
Imaging data: PET-CT
PET-CT scanning (at baseline and at Day 90, as evaluation preparatory to the possibility of the next implant) was utilized to evaluate the number, location, size/volume, and metabolic activity of both primary and metastatic tumors in all subjects. Use of the PET-CT scan without contrast for the CT scan was intended to reduce the risk of renal injury in these individuals, most of whom had a history of heavy pretreatment with nephrotoxic agents. Of course, this meant that the contrast-assisted measurement of tumor necrosis was not possible. We believe that the ability to define tumor metabolic activity data with the use of FDG compensated for this. Use of FDG, at least for lesions above 1 cm in diameter, ie, at or above the resolution level of the PET imaging, added another important measure of efficacy, enabling the evaluation of questionable metastases present on the CT portion of the PET-CT.
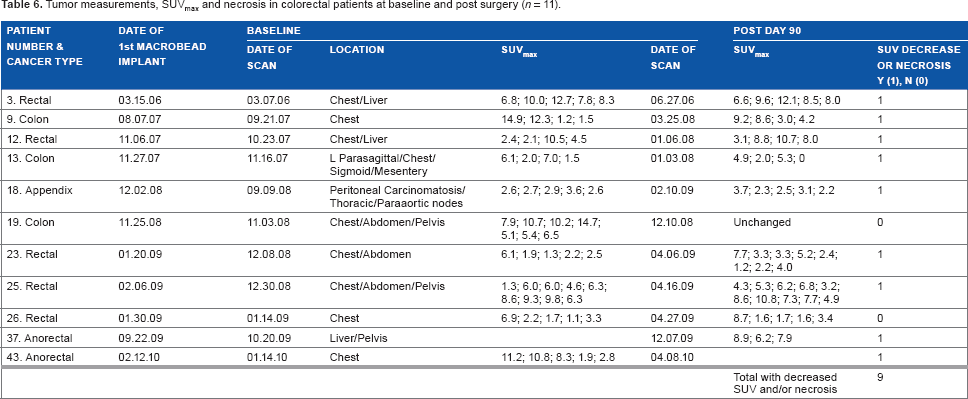
Several patterns became evident. First, some tumors seemed to increase in volume following RMB implantation. This phenomenon was difficult to interpret because of the enlargement of tumors induced by infiltrating lymphocytes and associated tissue damage. As this increase in volume did not necessarily persist, it seemed to reflect intra-tumor swelling. Second, there was a clear trend toward increased tumor necrosis that was not only central (as could be expected on the basis of tumor size alone) but often peripheral. Such peripheral necrosis represents a pattern unlikely to be the result of poor tumor vascularization but more likely an RMB anti-tumor effect. Such necrosis may also be accompanied by intra-tumor swelling. Third, decreases in 18 F-fluorodeoxyglucose uptake by the tumors were indicative of metabolic suppression of the tumor, again an effect very likely reflecting RMB-induced tumor damage. This effect was often seen even with stable tumor volume. In addition, necrosis and/or Standard Uptake Values (SUVs) occurred in 9 of the 11 evaluable subjects with colorectal cancer, who had a post-Day 90 scan (Table 6).
Tumor measurements, SUVmax and necrosis in colorectal patients at baseline and post surgery (n = 11).
Discussion
The results of this first-in-human Phase 1 evaluation of RENCA macrobead therapy conducted in 31 subjects with a total of 42 implantations over a six-year period (with individual exposure to RMB of up to four implants for up to three years) strongly support the feasibility and safety of its use for advanced, treatment-resistant, epithelial-derived cancers. RMBs are well tolerated after implantation and permit normal activity, including the ability to return to normal work responsibilities. No treatment-related serious adverse events or deaths occurred after implantation procedures. The most frequent treatment-related adverse events occurring in patients with various tumor types were transient and associated with the SIRS induced by the laparoscopic macrobead implantation. Other adverse events could be attributed to the advanced disease.
With respect to the efficacy of the RMB, the data from this study can only be regarded as preliminary, but it is encouraging. The response of the tumor markers in approximately 70% of these late-stage, treatment-resistant patients (as defined as a 20% or more decrease in either or both CEA and/or CA 19-9 within the first thirty days after macrobead implantation) suggests a positive response. With regard to CA 125, Table 3 has higher values than those shown in Table 4 because of the inclusion of a case of ovarian cancer (where it is at the inclusion of cases of pancreatic cancer), where CA 125 is a marker of peritoneal irritation and inflammation, rather than tumor progression. CA 125 was shown to rise initially and transiently in all patients in this Phase 1 trial as a result of the surgical implantation of the RMB and thus, the induction of mild peritoneal inflammation. This rise of CA 125 was transient, with the exception of the one case with ovarian cancer, where it was a marker of tumor progression and such progression did occur, and in cases (especially those of pancreatic cancer) where peritoneal carcinomatosis was seen and its progression documented.
Imaging data derived from the serial PET-CT studies are also encouraging, at least with regard to metastatic colorectal cancer in indicating suppression of metabolic activity and induction of necrosis. Evidence of a rapid tumor lysis syndrome, as has been described in the literature,7,8 was not observed. Although one cannot rule out spontaneous necrosis due to poor vascular supply, the suggestion, especially given the peripheral necrosis that was routinely observed, is that the necrosis is an effect of the RMB therapy and deserves further exploration.
The median OS after implantation of RMB, regardless of tumor type, was 5.4 months. It was 7.0 months for colorectal cancer and 5.7 months for other types of cancer, except for pancreatic cancer (1.1 months), indicating that the survival was not shortened by the macrobead therapy. The good, and even enhanced, quality of life experienced by most of the implanted patients cannot, per se, be attributed to the efficacy of the RMBs, but it does confirm their safety.
Definition of the mechanism(s) of action by which the RMB produce their anti-cancer effect must be a critical piece of the story. As described briefly in the Introduction, our studies of the genomics of the RMB and of the freely growing neoplastic cells exposed to the RMB directly or to the medium conditioned by the RMB have shown that the factor or factors released by the RMB induce the following range of gene expression changes in freely growing cancer cells: downregulation of DNA proliferation, angiogenesis, metalloproteinase production, oncogene activity, immune defenses, and the upregulation of differentiation and apoptosis-associated gene.1,2 The mechanism by which these changes in gene expression are achieved remains to be fully worked out, but we do now know that the transcription factor MEF2 is involved in producing approximately 40% of the overall tumor inhibitory effect. The clear upregulation of this transcription factor is achieved by either or both an EGFR-mediated pathway and the P13K/Akt pathway (unpublished data). Work to further identify the signal(s) responsible for this inhibitory effect and for the other regulatory effects yet to be identified is ongoing, with a major collaborative project with the mass spectroscopy laboratory at Lund University in Sweden now underway. The possibility that part of the effect of the RMB is achieved by other than protein or peptide signals, ie, mRNA, is also being explored in our laboratory, for example, the study carried out by Tiram et al. 9
The multiple gene expression changes that are induced by the signal(s) from the RMB provide a multipronged attack on the neoplastic cell that is consistent with the growing recognition of the complexity, heterogeneity, and dynamism/evolutionary capacity of tumor cells over time and in response to both natural and therapy-induced stresses. In fact, the situation is even more complex than that. The complex and dynamic nature of cancer as a biological system dynamic arises not only from the nature of the neoplastic cell itself and the interactions among tumor cells but also from their interactions with the cells and matrix of the tumor microenvironment,10–12 normal neighboring cells,13,14 endothelial and other vascular cells,15,16 the immune system, 17 and the endocrine system, 18 to name just a few parts of the system. These interactions may be autocrine, paracrine, exocrine (as with exosomes),10,19 circulating tumor cells 20 and circulating DNA, DNA fragments, chromatin, and mRNA21,22 (exosomal or not),10,19 and hormonal. 18 They alter cell behavior at the molecular, genomic, and epigenetic levels. 23 The data of Gerlinger et al 24 and, even more perhaps, data of Ling et al 25 demonstrating striking genetic diversity even in a single tumor (286 genotyped samples revealed more than 100 million coding region mutations) provide further support for dynamic complexity of solid tumors, 23 both as primary and metastatic lesions. The large number of coding region mutations supports the hypothesis, as Ling et al argue, that tumors are capable of non-Darwinian evolution and have an ability to evolve rapidly over time. Because of this, they present a moving therapeutic target, a phenomenon that is well known to oncologists. 26
From this conceptual point of view, understanding the molecular and cellular biology as well as the interacting network of signaling pathways of any given tumor over time and defining appropriate therapies require the application of systems biology approaches.26––29 Specific examples of the complex and dynamic regulatory processes operative in neoplastic cell populations exist. These include the phenomenon of contact inhibition; the slowing of tumor growth in vivo with increasing tumor mass;30––44 and the high genetic diversity in individual tumors indicative of non-Darwinian evolution 45 already mentioned above. Modeling such complex multibody dynamical systems to better understand them and develop therapeutic targets remains a major challenge. 45
Given these observations, it is not unreasonable to hypothesize that an anti-cancer treatment could consist of the provision of an implantable biological system capable of controlling multiple aspects of the neoplastic cell's growth regulatory mechanisms. Such a system requires both a delivery mechanism, a sensor mechanism (responsive to changes in tumor biomarkers), and the ability to protect the implanted cell system from the host immune system. In another complex, but nonmalignant disease, we have achieved such a system with our islet macrobeads.46––51
Yet another example of the power of an implanted cell system is that of synthetic biology-based gene circuits in the form of encapsulated cells to treat psoriasis, a chronic inflammatory skin disease characterized by a relapsing-remitting disease course and correlated with increased expression of pro-inflammatory cytokines, such as TNF and interleukin 22 (IL22). 52 Psoriasis presents therapeutic challenges because of its unpredictable and symptomless flare-ups, so that treatment is limited to symptomatic changes. Schukur et al 52 point out that cell systems with characteristics such as the one they have designed for psoriasis are “uniquely suited for the treatment of diseases with complex dynamics because they can autonomously couple the detection of disease biomarkers with the production of therapeutic proteins.” In their case, they have a mammalian cell synthetic cytokine converter that [selectively] quantifies psoriasis-associated TNF and IL22 levels using serially linked, receptor-based synthetic signaling cascades, processes the levels of these proinflammatory cytokines with AND-gate logic, and triggers the corresponding expression of therapeutic levels of the anti-inflammatory/psoriatic cytokines IL4 and IL10.
Their goal was to take what they have demonstrated in their mouse model to patients. Their point is that the implanted cells they have designed to release anti-inflammatory cytokines will “dynamically interface with the patient's metabolism by detecting specific disease metabolites or biomarkers, processing their blood levels with synthetic circuits in real time, and coordinating immediate production and systemic delivery of the relevant protein therapeutics.”
What the RMB represent is an attempt to do just what the islet macrobeads and the cytokine-detection cells of Schukur et al 52 are intended to do, with the important difference being that the RMBs are being used in a neoplastic disorder. They constitute a biological (neoplastic) system that, by virtue of the entrapment of its cells in an agarose matrix, is induced to change the expression of its genome to produce factors that inhibit, rather than foster, the growth and survival of neoplastic cells outside the macrobead. It is a complex, responsive biological system that is designed to control a freely growing equally or more complex and dynamic neoplastic cell system, with control, in this sense, meaning cytostatic, cytotoxic, and/or dormancy-promoting capability. 9 The safety and very preliminary efficacy data of this Phase 1 trial are consistent with the hypothesis that the RMB is such a system.
The limitations of any open Phase 1 study in advanced, treatment-resistant, epithelial-derived cancer are many. A particular limitation of this study is the inclusion of different types of tumors so that experience with any one tumor type is necessarily limited. Genotyping, which was not done in this study, will need to be done in any subsequent trial, moving beyond KRAS to the wide range of genes and gene mutations now associated with colorectal cancer. Even with the 12 metastatic colorectal cancer patients included in this Phase 1 study, the fact that none of these tumors is genomically identical, along with the varied comorbidities of the individual patients and the rapid genomic and epigenetic evolution of the tumors themselves, introduces even more complexity. This dynamism presents problems for a randomized trial, let alone a Phase 1 study in a late-stage cancer patient population. Innovative trial designs are needed if complex, systems biology-based therapeutic approaches and agents are to be meaningfully evaluated. The possibility of combining the RMB therapy with other gene and immunomodulatory therapeutic modalities should be explored as well because of the potential synergies that seem likely.
Implantations of RMB in a variety of end-stage, treatment-resistant, epithelial-derived solid tumor patients were indeed safe. It is very difficult to comment on the efficacy of the RMB in virtually all of the tumor types included in this study, with the possible exception of colorectal cancer, where there were 14 out of the total 31 patients.
In summary, the survival data from the patients with colorectal cancer in the Phase 1 study were encouraging enough to suggest that any Phase 2 trial should focus on these patients. Phase 2 trials to evaluate the efficacy of the RMB in mCRC and pancreatic cancer are ongoing.
Footnotes
Acknowledgments
Appreciation is extended to Vital Systems Inc. for their data collection and statistical analysis. We are also grateful for the continuing financial support of this project received from Metromedia Bio-Science LLC.
Author Contributions
Conceived and designed the experiment: BHS, DML, TSP, LSG, TJF and AJO. Analyzed data: BHS, DML, TSP, AA, EA and AN. Wrote first draft of manuscript: BHS, TP, ZPA and AN. Contributed to the writing of the manuscript: All authors. Agree with manuscript results and conclusion: All authors. Jointly developed the structure and argument for the paper: BHS, AN, TP, ZPA, DJW, DML, TSP, and NB. Made critical revisions and approved final version: BHS, AN, TJF, TSP and LSG. Administrative support: BHS, AN, TP, ZPA, JT, AA, DML, TSP and MW. All authors reviewed and approved the final manuscript.