
Abstract
PARP-1 (poly(ADP-ribose) polymerase-1) plays an important role in tumorigenesis. Since its effects on different populations are varied, this study investigated the impact of PARP-1 on primary hepatocellular carcinoma in a Southern Chinese Zhuang population. We assessed the global PARP-1 messenger RNA expression in patients with hepatocellular carcinoma using The Cancer Genome Atlas dataset. Increased PARP-1 expression, related to alpha-fetoprotein level, was observed. The area under the receiver operating characteristic curve value was 0.833. Kaplan–Meier survival curves indicated that higher PARP-1 expression was not correlated with poorer overall survival and recurrence-free survival. In a Zhuang population, PARP-1 messenger RNA and protein levels were increased in the hepatocellular carcinoma tissue and its adjacent liver tissues as assessed by quantitative polymerase chain reaction, immunohistochemistry, and western blotting. Higher PARP-1 level was associated with a higher tumor stage (p < 0.05), without correlation with age, gender, smoking, drinking, tumor size, serum alpha-fetoprotein level, hepatitis B virus infection, metastasis, and invasion (p > 0.05). Further analysis suggested that H2AX, a PARP-1 protein interaction partner, was coordinated with PARP-1 in hepatocellular carcinoma tumorigenesis. Overall, some new characteristics of PARP-1 expression were noted in the Zhuang population. PARP-1 is a novel promising diagnostic marker for hepatocellular carcinoma in the Southern Chinese Zhuang population.
Introduction
Poly(ADP-ribose)polymerase-1 (PARP-1), the most abundant isoform of the PARP family, is a 116-kDa nuclear enzyme involved in many key biological processes, such as DNA damage repair, replication, cell proliferation control, and apoptosis.1 –3 PARP-1 is known to be involved in the cellular response to DNA damage repair. 4 When PARP-1 detects DNA damage, it is auto-modified and recruits repair factors to the DNA damage sites.4,5 Defects in DNA repair lead to genomic instability and play a critical role in cancer development. 6 Abnormal PARP-1 expression has been reported in various cancers, including those of the breasts, lungs, and ovaries.7,8 Higher PARP-1 expression was noted in various cell lines showing tumor progression.9,10
Hepatocellular carcinoma (HCC) is a lethal cancer. Its incidence is increasing worldwide with 782,500 new liver cancer cases and 725,500 deaths each year, and 50% of the total deaths are recorded in China.11 –14 Major risk factors associated with HCC include chronic hepatitis B virus (HBV) infection, hepatitis C virus (HCV) infection, alcoholic and non-alcoholic steatohepatitis, food contamination by aflatoxin B1, and some inherited metabolic disorders.12,15,16 Several studies reveled that amplified in liver cancer 1 (ALC1) ATPase activity was dependent upon both PARP-1 and NAD+. 3 Inhibition of PARP-1 decreased HCC growth and enhanced tumor sensitivity to cisplatin in liver cancer cell lines. 17 However, Piskunova et al. 18 reported that HCC developed at a significantly higher frequency in PARP-1−/− mice than PARP-1+/+mice (72% and 49%, respectively, p < 0.05). Some studies have reported that PARP-1 is upregulated in human HCC specimens.19 –21 Our previous studies also indicated that PARP-1 expression was significantly increased in human HCC cell, and it coordinated with H2AX, a sensitive marker for double-strand breaks (DSBs). 22 Co-localization of PARP-1 and γH2AX was observed in the HCC cells. 22
Globally, there are geographic differences in HCC incidence and trends.23,24 HCC remains highly prevalent in China, especially in the southern coastal area, including Guangdong and Guangxi Provinces, where Zhuang population inhabit. 25 According to the sixth nation-wide population census conducted in the year 2010, the population belonging to the Zhuang ethnic group was 16.92 million, and over 90% of the Zhuang population inhabits Guangxi Province (http://www.stats.gov.cn). Polymorphism sites in exons 12, 13, 16, and 17 of the hPARP1 gene were reported in Southern Chinese Han and Miao populations. 26 The expression of PARP-1 in HCCs in Eastern Chinese population was significantly associated with tumor size and stage. 27 However, no study was conducted in the Southern Chinese Zhuang population.
In this study, we used the RNA-seq data from The Cancer Genome Atlas (TCGA) database to analyze the PARP-1 expression. Then, we assessed PARP-1 expression in paired samples of tissues from the patients in Zhuang population and discussed its clinical correlation. Simultaneously, we also analyzed H2AX (a PARP-1 interacteror) expression in the HCC tissues and discussed its clinical roles.
Materials and methods
Data collection and analysis from TCGA Liver Hepatocellular Carcinoma dataset
RNA sequencing (RNA-seq) data and patients’ clinical and demographic information of HCC patients from TCGA Liver Hepatocellular Carcinoma (LIHC) dataset were downloaded from the Xena Public Data Hubs (https://xenabrowser.net/). As described in UCSC Xena website, the gene expression profile was measured experimentally using the Illumina HiSeq 2000 RNA Sequencing platform by the University of North Carolina TCGA genome characterization center. Level 3 data were downloaded from TCGA data coordination center. RNA-seq data were quantified using RSEM (RNA-Seq by Expectation-Maximization) as described previously. 28 Association between the expression of selected genes and clinicopathological features and survival of HCC patients were analyzed.
HCC patients of Zhuang population and tissue samples
A total of 96 HCC patients of Zhuang population enrolled in this study. HCC tumor tissues and its paired adjacent normal tissues were obtained by hepatectomy from the First Affiliated Hospital of Guangxi Medical University; written informed consent and approval from the Ethics Committee were obtained. The diagnosis of HCC was made by pathological examinations of the resected tissues after operation. No patients received preoperative treatments prior to the surgery. All tumors were classified according to the International Union Against Cancer tumor–node–metastasis classification system and World Health Organization criteria. The clinicopathological characteristics of enrolled HCC patients (age, gender, smoking, drinking, tumor size, the alpha fetoprotein (AFP) in serum, and HBV infection, metastasis, and invasion) were shown in Table 1.
Correlation between the factors and clinicopathological characteristics in HCC in TCGA dataset (n = 363).

HCC: hepatocellular carcinoma; TCGA: The Cancer Genome Atlas; LIHC: Liver Hepatocellular Carcinoma; RSEM: RNA-Seq by Expectation-Maximization; PARP-1: poly(ADP-ribose) polymerase-1; AFP: alpha fetoprotein; SD: standard deviation.
p < 0.05.
Reverse transcription polymerase chain reaction
Total RNA was extracted using the TRIzol Reagent (Invitrogen). Up to 1 µg of RNA was reversed transcribed using the PrimeScript RT reagent Kit with gDNA Eraser (Takara). Complementary DNA (cDNA) was amplified in SYBR green master mix (Roche) with the Realplex (Eppendorf). Conditions used for polymerase chain reaction (PCR) were as follows: an initial 10-min 95°C period followed by 40 cycles of 95°C for 15 s and 60°C for 1 min through the reverse transcription PCR (RT-PCR) System Thermal Cycling Block (Applied Biosystems StepOnePlus). Relative messenger RNA (mRNA) levels were determined using the 2−ΔΔCt interpretation and normalized by β-actin. The primers used for PCR amplification were 5′-GCAACCACACACAATGCGTA-3′ (forward) and 5′-GTTGGCACTCTTGGAGACCA-3′ (reverse) for PARP-1; 5′-CTCCATCCTGGCCTCGCTGT-3′ (forward) and 5′-GCTGTCACCTTCACCGTTCC-3′ (reverse) for β-actin.
Western blot analysis
Tissues were lysed with radioimmunoprecipitation assay (RIPA) buffer. Protein concentrations were determined using the DCTM Protein Assay (Bio-Rad). Following sodium dodecyl sulfate polyacrylamide gel electrophoresis (SDS-PAGE), western Blot analysis was performed using the following primary antibodies: γH2AX (Abcam), β-actin (Abcam), and PARP-1 (Santa Cruz Biotechnology). A horseradish peroxidase–conjugated antibody (Abcam) was used as a secondary antibody. Pierce ECL Western Detection Kit (Thermo Fisher Scientific) was used for protein visualization.
Immunohistochemistry
HCC tissue specimens were paraffin-embedded and sectioned. After sections were deparaffinized in water, heat-induced antigen retrieval in 10 mM citric acid buffer for 15 min was performed. The endogenous peroxidase activity was blocked in hydrogen peroxide (0.3%). The sections were incubated at 4°C with anti-PARP-1 antibody (1:1000) and anti-γH2AX antibody (1:500) overnight, followed by incubation with biotinylated secondary antibodies at room temperature after rinsing in phosphate-buffered saline (PBS; pH 7.2). Negative control slides were incubated in parallel in PBS only. Finally, the slides were counterstained with hematoxylin, dehydrated, and mounted in resin blocks. The degree of immunohistochemistry (IHC) staining was evaluated by two independent pathologists. Five high-power fields were randomly chosen in each section for assessment of PARP-1 and γH2AX, and at least 300 cells were counted per field.
Statistical analysis
Statistical analyses were performed using the SPSS 19.0 software package. Data were expressed as mean ± standard deviation (SD). Two-sided Student’s t-tests/paired Student’s t-tests were used to compare quantitative sample data. Analysis of variance (ANOVA) analyses and Pearson’s chi-squared were used for correlation analyses. The area under the receiver operating characteristic (ROC) curve (AUC) was used to evaluate the diagnostic performance. The overall survival (OS) and recurrence-free survival (RFS) curves were generated by the Kaplan–Meier survival curves and analyzed using the log-rank test. Patients were divided into two groups (high and low) according to median expression level of RSEM of PARP-1 for survival analysis. 29 A p value of less than 0.05 was considered significant in all cases.
Results
PARP-1 and H2AX analyses in TCGA dataset
Data on PARP-1 expression at the mRNA level were obtained from 419 tissues (363 tumor tissues and 50 adjacent tumor tissues) in TCGA. The expression of H2AX and PARP-1 was significantly upregulated in tumor tisssues as compared to the adjacent non-tumor tissue (Figure 1(a)). To further evaluate the diagnostic significance of PARP-1 and H2AX, an ROC curve was constructed by plotting sensitivity versus specificity (Figure 1(b)). The value for AUC of PARP-1 was 0.833 (p < 0.01). Based on the maximum Youden index discriminating patients with HCC from controls, an optimal cut-off value of 11.55 was obtained, and its sensitivity and specificity for predicting HCC were calculated to be 67.5% and 93.9%, respectively.
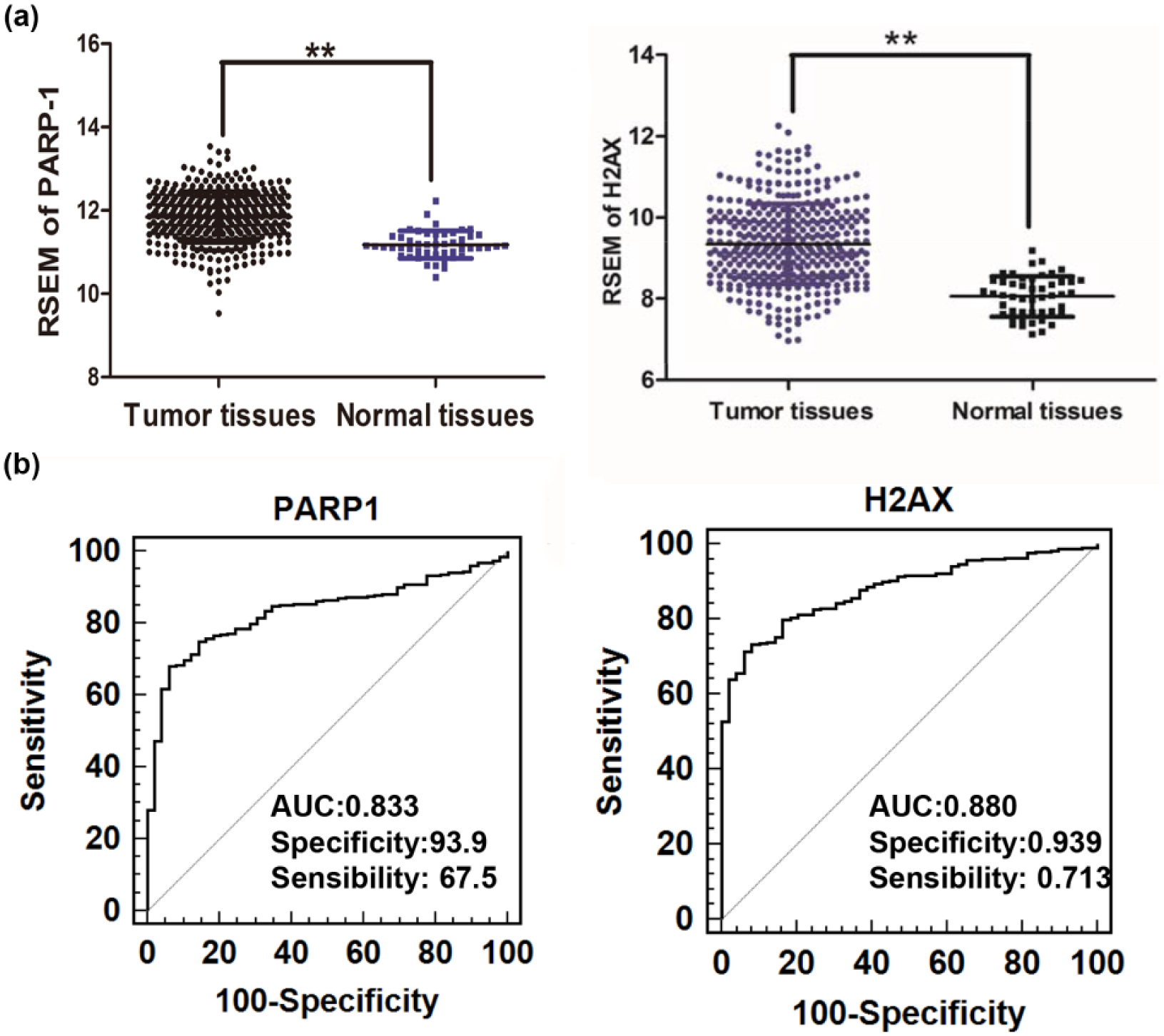
Data mining of PARP-1 in TCGA dataset. (a) RSEM of PARP-1 and H2AX. Significant differences were observed between tumor tissues and normal tissues. (b) ROC curve of PARP-1 and H2AX (**p < 0.01).
Clinical data from 363 tumor tissues were further studied. Results showed that AFP levels in serum were significantly correlated with PARP-1 expression. However, there was no correlation between PARP-1 expression and gender, age, smoking, drinking history, HBV infection, clinical stage, Child–Pugh score, and metastasis (Table 1).
Increased PARP-1 and γH2AX expression in patients with HCC in Zhuang population
Compared to the adjacent tissues, HCC tissues showed decreased PARP-1 expression at both mRNA and protein levels (Figure 2). The results of western bolting and IHC revealed that the expression of PARP-1 and γH2AX in the HCC tissues was higher than that in the adjacent tissues in 96 patients from Zhuang Province (Figure 2(b) and (c)). Both the proteins were mainly expressed in the nucleus, and PARP-1-positive cells were detected in all the HCC tissues (96/96) with an average rate of 68.39% ± 27.31%. In the adjacent tissues, only 26.04% (25/96) cells were positive for PARP-1 and 20.83% (20/96) were positive for γH2AX.

Expression of PARP-1 and γ-H2AX in human HCC cells. (a) Relative mRNA expression of PARP-1. Test sites are listed on the X-axis, and the relative expression level is shown in the Y-axis. (b) Western blotting of PARP-1 and γ-H2AX. Lanes 1, 3, 5, and 7: cancer tissues; lanes 2, 4, 6, and 8: adjacent tissues. (c) Representative images showing immunohistochemical staining of PARP-1 and γ-H2AX in tumor tissues and adjacent tissues.
Association between PARP-1 expression and clinicopathological features of patients with HCC in Zhuang population
Higher PARP-1 expression could be correlated with a higher stage of HCC (p< 0.01). The rate of PARP-1-positive cells in stages III and IV was higher than that in stages I and II. No association was observed between PARP-1 expression and age, gender, smoking, drinking, tumor size, serum AFP level, HBV infection, metastasis, and invasion (p > 0.05). All results are shown in Table 2.
Correlation between the factors and clinicopathological characteristics in the Southern Chinese Zhuang population (n = 96).

HCC: hepatocellular carcinoma; TCGA: The Cancer Genome Atlas; LIHC: Liver Hepatocellular Carcinoma; RSEM: RNA-Seq by Expectation-Maximization; PARP-1: poly(ADP-ribose) polymerase-1; AFP: alpha fetoprotein; SD: standard deviation.
p < 0.05.
The influence of PARP-1 expression level on OS in HCC patients
Kaplan–Meier analysis revealed that patients with a high PARP-1 expression did not have a significantly poorer prognosis compared with those with a low PARP-1 expression (p > 0.05). The number of patients with high or low PARP-1 expression, the number of dead or alive patients, and values of Log-rank test and Gehan–Breslow–Wilcoxon from the Kaplan–Meier analysis were shown in Table 3. Figure 3(a) and (b) shows the association between PARP-1 expression and OS and RFS, respectively.
The number of patients with high or low PARP-1 expression, the number of dead or alive patients, and values of Log-rank test and Gehan–Breslow–Wilcoxon from the Kaplan–Meier analysis in TCGA dataset.
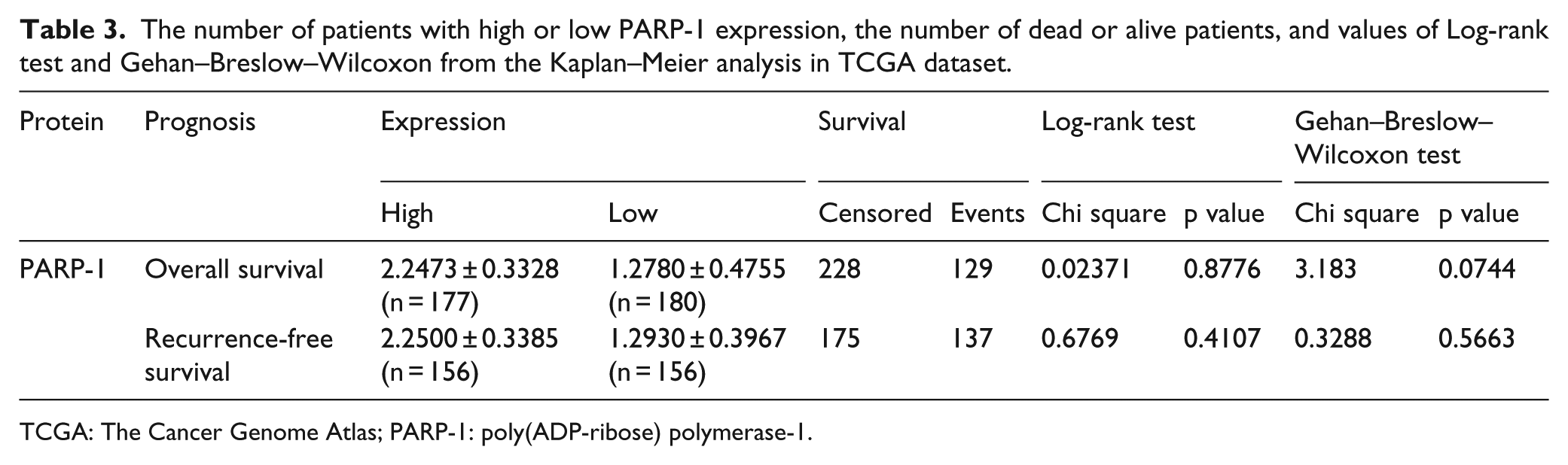
TCGA: The Cancer Genome Atlas; PARP-1: poly(ADP-ribose) polymerase-1.
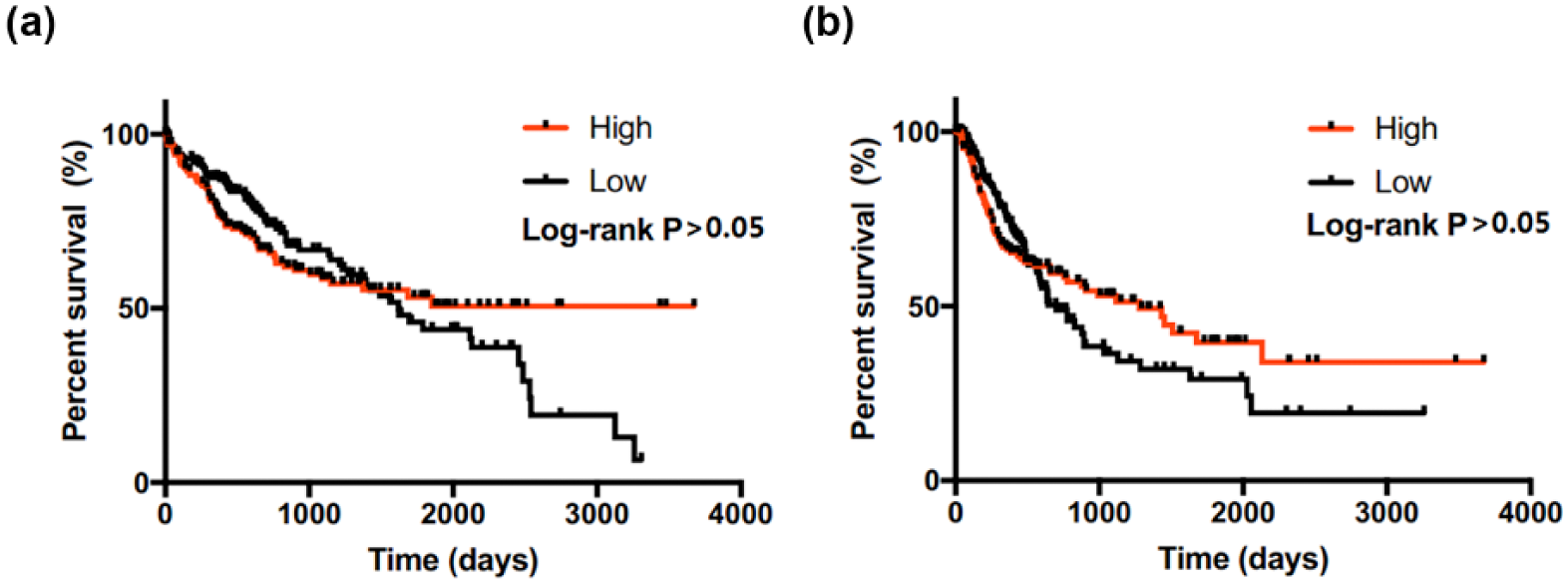
Kaplan–Meier curves of OS and RFS of PARP-1 expression in hepatocellular carcinoma samples. Kaplan–Meier analysis revealed that patients with a high PARP-1 expression did not have significantly poorer prognosis compared with those with a low PARP-1 expression (p > 0.05): (a) overall survival and (b) recurrence-free survival.
Discussion
Human PARP-1 was reported as a novel promising diagnostic/prognostic marker for HCC in an Eastern Chinese population. 27 However, the role of PARP-1 in population from different regions is not known. Ours is the first study investigating the effect of PARP-1 on HCC in Southern Chinese Zhuang population. TCGA dataset analysis without stratification of population also revealed an increased PARP-1 mRNA expression in HCC. A similar result was obtained with HCC tissue samples from a Zhuang population. Furthermore, PARP-1 protein expression in HCC tissues was significantly higher than that in the adjacent normal tissues, as confirmed by western blotting and IHC of a large number of clinical specimens. The results were consistent with those of mRNA expression. PAPR-1 expression increased the replication efficiency of HBV, inhibited the DNA repair capacity, and potentially contributed to the development of HCC. 30
It is intriguing that the associations between PARP-1 high/low status and clinical characteristics are different among different populations. The results of TCGA dataset, without stratification of population, showed that the PARP-1 mRNA expression was only associated with AFP, without a correlation with gender, age, smoking, drinking history, HBV infection, clinical stage, Child–Pugh score, and lymph node metastasis. A previous study revealed that high PARP-1 protein expression was significantly associated with larger tumor size and higher stage in Eastern Chinese population. 27 In the Zhuang population, we only found a significant correlation between higher PARP-1 and higher tumor stage of HCC. The difference indicated that genetic factors affected the role of PARP-1. It was reported that peri- and postmenopausal women carrying the C-allele of the PARP-1 Val762Ala polymorphism (rs1136410) present a statistically significant lower OS and disease-free survival (DFS) among those with early-stage cervical cancer. 31 In the previous meta-analysis, PARP-1 polymorphism (rs1136410: T > C) was also noted to be a risk factor for gastrointestinal cancers in an Asian population, but not in a Caucasian population. 32 PARP-1 would be an advantageous indicator of the disease for population studies.
Furthermore, after analyzing TCGA database with clinical information, we did not find that the average OS of the HCC group with a relatively higher PARP-1 expression was shorter than that of the group with lower PARP-1 expression. As reported previously, higher PARP-1 was related to poor survival in HCC.27,33,34 These results suggested that PARP-1 did not affect Zhuang population similar to the other population, such as Spanish and Eastern and Northeastern Chinese population.
Since our previous study showed that H2AX protein interacts with PARP-1, 22 we detected H2AX in TCGA dataset and the active H2AX (γH2AX) in the Zhuang population. Higher H2AX expression was observed in HCC tissues in TCGA dataset. The AUC was 0.88, close to that of PARP-1. Sharma et al. 35 reported that the expression of γH2AX was associated with race. In the Zhuang population, the protein expression of γH2AX was increased in the HCC tissues than in the adjacent normal tissues, consistent with the expression of PARP-1. However, the result of IHC showed that the rate of γH2AX-positive cells was less compared to that of PARP-1-positive cells in the HCC tissues. H2AX senses DSBs in the DNA and recruits characteristic sets of proteins at its phosphorylated (γH2AX) foci for concurrent DNA repair.36,37 PARP-1 belongs to the HCC-specific H2AX interactome dataset. 22 Our results indicated that PARP-1 was involved in the HCC tumorigenesis via γH2AX in the Zhuang population. However, the in-depth details need to be studied further.
In conclusion, PARP-1 expression is higher in HCC tissues, and higher PARP-1 was correlated with a higher tumor stage in a Zhuang population. PARP-1 expression is not associated with OS and RFS. PARP-1 may play an important role in the development of HCC and may be a biomarker for diagnosing HCC and a potential molecular target of HCC therapy. The diagnostic and prognostic values of PARP-1 and its possible therapeutic applications are worth further investigation.
Footnotes
Acknowledgements
J.L., D.D., P.L., and W.L. have contributed equally to this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors gratefully acknowledge the National Natural Science Foundation of China (grant no. 81660497), the Guangxi Natural Science Foundation (grant no. 2016GXNSFDA380010), and the High Incidence of Guangxi Local Disease Prevention and Control Foundation (grant no. 0842009-Z6 (Guikeneng)).