
Abstract
Glutathione peroxidase 2 has important role of tumor progression in lots of carcinomas, yet little is known about the prognosis of glutathione peroxidase 2 in hepatocellular carcinoma. Glutathione peroxidase 2 expression was assessed by immunohistochemistry in hepatocellular carcinoma tissues. The association between glutathione peroxidase 2 expression with clinicopathological/prognostic value was examined. Glutathione peroxidase 2 overexpression was correlated with alpha-fetoprotein level, larger tumor, BCLC stage, and tumor recurrence. Kaplan–Meier analysis showed that glutathione peroxidase 2 was an independent predictor for overall survival and time to recurrence. glutathione peroxidase 2 overexpression was correlated with poor prognosis in patient subgroups stratified by tumor size, differentiation, tumor–node–metastasis, and BCLC stage. Moreover, stratified analysis showed that tumor–node–metastasis stage-I patients with high glutathione peroxidase 2 expression had poor prognosis than those with low glutathione peroxidase 2 expression. Additionally, combination of glutathione peroxidase 2 and serum alpha-fetoprotein was correlated with prognosis in hepatocellular carcinoma. In conclusion, glutathione peroxidase 2 overexpression contributes to poor prognosis of hepatocellular carcinoma patients and helps to identify the high-risk hepatocellular carcinoma patients.
Introduction
Hepatocellular carcinoma (HCC) is one of the most aggressive tumors associated with high recurrence incidence and poor prognosis and the third most frequent cause of cancer-related death in the world.1,2 Hepatic resection and liver transplantation have remained the most effective treatment with curative potential; however, only 30%–40% of HCC patients are eligible for curative treatments, even in developed countries.3–5 Traditional tumor–node–metastasis (TNM) classification systems provide a basic prognostic model but still have limited capacity to differentiate outcomes when considering the asymptomatic nature and limited detection of early-stage HCC. 6 In addition, survival may vary widely among HCC patients with the same clinicopathological features, which is most likely attributable to the heterogeneity of the biological behavior of tumor cells.7,8 Therefore, identifying new sensitive and reliable biomarkers for the diagnosis, prognosis, and target therapy of HCC is extremely important.
Glutathione peroxidase 2 (GPX2), also known as gastrointestinal GPX, belongs to the antioxidant enzyme GPX family. So far, the antioxidant enzyme family has eight different isoforms of glutathione peroxidase (GPX1–8) in mammals.9,10 Because of their antioxidative activity, several isoforms of GPXs have been investigated in association with inflammation and cancer. 11 GPX2 reduces hydroperoxides and is considered to play a major role in antioxidant defence.11,12 GPX2 is exclusively expressed in gastrointestinal tract, and in human, GPX2 is also expressed in liver. 13 Moreover, GPX2 has been suggested to protect against oxidative damage from food. 14 Recently, GPX2 has been shown to play an important role in the progression of malignant tumors. Overexpression of GPX2 protein is detected in HCC, 15 colorectal cancer,16,17 breast cancer, 18 lung cancer 19 and castration-resistant prostate cancer. 20 And GPX2 could be an important predictor for the prognosis of malignant tumors.20–22 However, the role of GPX2 in prognosis of HCC patients has not been well clarified.
In this study, we therefore analyzed the expression of GPX2 in HCC tissues by immunohistochemistry (IHC). Correlation of GPX2 with clinicopathological parameters and prognosis of HCC patients were analyzed. In addition, it has been known that serum alpha-fetoprotein (AFP) level is an unfavorable prognostic factor for HCC patients. 23 Therefore, we also investigated the prognostic value of GPX2 combined with serum AFP level in HCC patients.
Methods
Patients and specimens
The study was approved by the Institutional Review Board and Human Ethics Committee of Cancer Center, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology. Written consent for using the samples for research purposes was obtained from all patients prior to surgery.
All HCC samples and adjacent non-tumorous liver tissues were collected from 185 patients who had received curative liver resection from May 2009 to November 2010 at the Cancer Center, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology (Wuhan, China). The eligibility criteria of the current study were as follows: (1) all the tumor and adjacent non-tumorous tissues were confirmed histologically, (2) none of the patients had distant metastasis or received anticancer treatment prior to hepatectomy, and (3) no serious complications or other malignant diseases. The cases were selected consecutively on the basis of availability of resection tissues and follow-up data. Detailed clinicopathological features were obtained from patients’ files. Tumor stages were classified according to the 7th edition of the TNM system of the International Union Against Cancer by the 2010 American Joint Committee. Overall survival (OS) was computed from the day of surgery to the day of death or last follow-up. Time to recurrence (TTR) was defined as from the day of surgery to the day of relapse, metastasis, or last follow-up.
IHC staining
The HCC tissues and their adjacent non-tumorous samples were used in the IHC analysis. After being baked at 60°C for 2 h, the samples were deparaffinized and hydrated and incubated with 3% hydrogen peroxide. The sections were microwaved for antigen retrieval in 0.01 M sodium citrate buffer (pH 6.0) for 30 min and then preincubated in 10% normal goat serum for 30 min to prevent nonspecific staining. The sections were incubated with the GPX2 rabbit polyclonal antibody (working dilution 1:200, #ab64322; Abcam, Cambridge, UK) overnight at 4°C. Subsequently, the sections were incubated with a biotinylated goat anti-rabbit secondary antibody (Dako, Glostrup, Denmark) for 30 min at room temperature. Assessments of the staining were scored by two experienced pathologists blinded to the patients’ identity and clinical status. In discrepant cases, a pathologist reviewed the cases and reached the consensus.
Both the extent and intensity of immunostaining were taken into consideration when analyzing the data. The intensity of staining was scored from 0 to 3, and the extent of staining was scored from 0% to 100%. The final quantitation of each staining was obtained by multiplying the two scores. GPX2 expression was classified as high expression if the score was higher than the median score of 1.1, and if the score was 1.1 or less, the case was classified as low expression.
Follow-up
The study was censored on 31 May 2016. The median follow-up time was 48.0 months (range = 3.0–73.0 months). All patients were followed up every 1–3 months in the first year and every 3–6 months thereafter. The follow-up protocol included physical examination, serum AFP level, chest X-ray, and abdominal ultrasonography. Computed tomography and/or magnetic resonance imaging and/or positron emission tomography were performed when intrahepatic relapse or distant metastasis was suspected. The main causes of death were HCC recurrence or complicated cirrhosis of the liver. During the course of follow-up, the rate of recurrence was 53.5% (99/185), while there were 84 patients (45.4%) died of cancer-related causes.
Statistical analysis
All statistical analyses were carried out using the SPSS software package (version 16.0; Chicago, IL, USA). The chi-squared test or Fisher’s exact test was used to analyze the correlation of GPX2 status with clinicopathological features. The Student’s t-test was used for comparisons. OS and TTR curves were generated using the Kaplan–Meier method, and differences between curves were estimated by the log-rank test. The Cox multivariate proportional hazards regression model was used to determine the independent factors that influence survival and recurrence based on the investigated variables. All p values were two-sided, and p value less than 0.05 was considered to be statistically significant.
Results
GPX2 expression in HCC and adjacent non-tumorous liver tissues
To illuminate the biological significance of GPX2 in HCC, we examined the immunohistochemical expression of GPX2 in 185 HCC specimens (tumor and matched adjacent non-tumorous tissues). Our results found that GPX2 was primarily localized in the cytoplasm of tumor cells (Figure 1(a)). The positive rate of GPX2 expression was 54.6% (101/185) in primary HCC specimens, while there was only 15.7% (29/185) in adjacent non-tumorous tissues (p < 0.001; Figure 1(b)). These data indicate that GPX2 expression is significantly higher in HCC tissues than that in adjacent non-tumorous tissues.
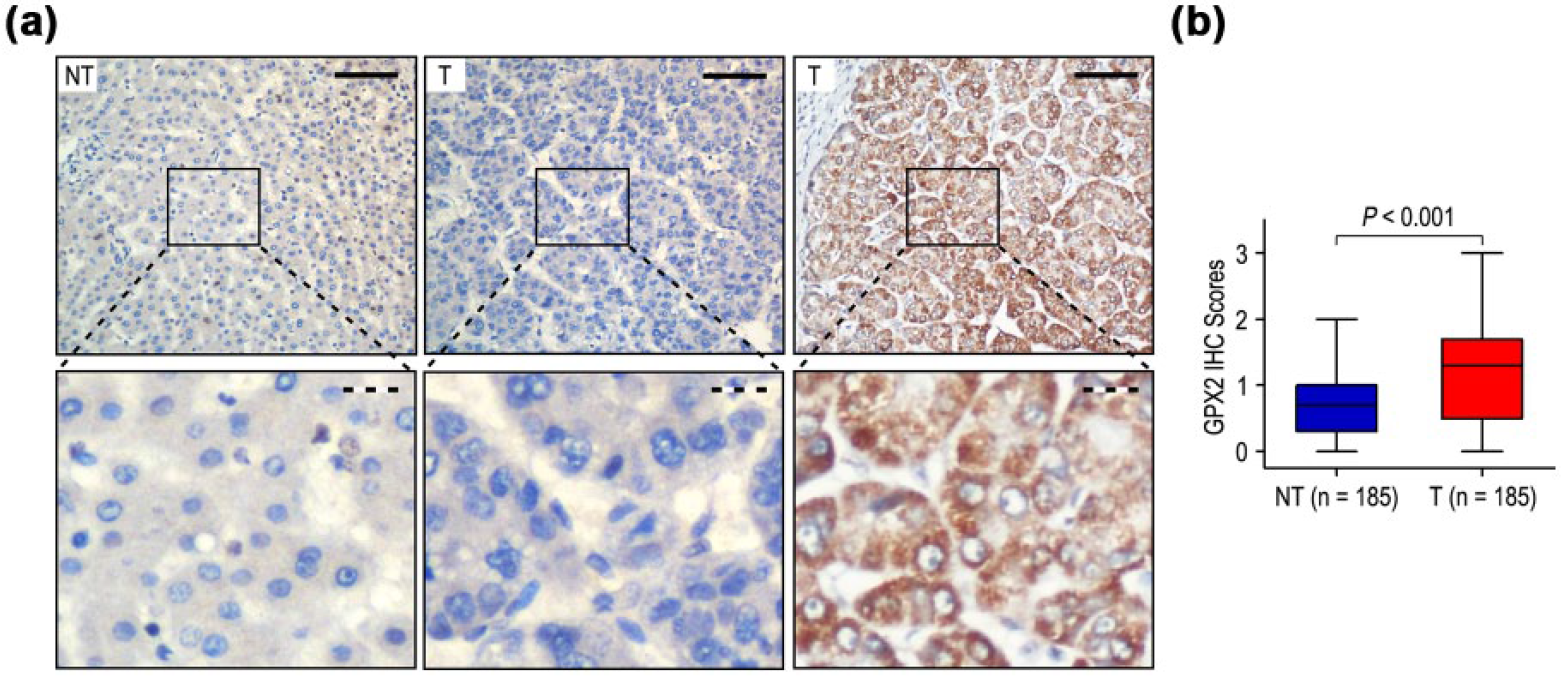
GPX2 was upregulated in HCC tissues. (a) Immunohistochemistry (IHC) assays of GPX2 expression in 185 paired HCC and adjacent non-tumorous tissues. The upper left panel represents low GPX2 expression in adjacent non-tumorous tissues. The upper middle and right panels represent low and high GPX2 expression in HCC. Lower panels represent magnified pictures of boxed area in the corresponding upper panels. The full line and dotted line scale bars represent 50 and 10 µm, respectively. (b) GPX2 expression levels were compared with HCC and adjacent non-tumorous specimens. Statistical analysis was performed by paired-samples t-test.
The association of GPX2 with clinicopathological variables
According to the results of IHC, we correlated GPX2 status with widely recognized clinicopathological features in 185 HCC samples. The high GPX2 expression in HCC was positively correlated with high AFP level (p = 0.008), larger tumor (p < 0.001), BCLC stage (p = 0.001), and tumor recurrence (p < 0.001; Table 1). In contrast, no significant association was observed between gender, age, HBsAg, gamma-glutamyltransferase (GGT), liver cirrhosis, tumor number, satellite nodule, tumor capsule, tumor differentiation, vascular invasion, and TNM stage with GPX2 expression (all p > 0.05). In addition, the expression levels of GPX2 in tumors increased in TNM and BCLC stage-dependent manner, and they were significantly higher in TNM stage-III and BCLC stage-C tumors than those in TNM stage-I and BCLC stage-0 tumors (Figure 2). It has been known that HCC recurrence can be divided into early recurrence and late recurrence, using 36 months post-resection as cut-off time. 24 The expression of GPX2 was both higher in the early and late recurrence groups, compared with that in the no recurrence groups (p = 0.001 and p = 0.014, respectively; Figure 3).
Correlation of GPX2 protein expression with clinicopathological parameters.

AFP: alpha-fetoprotein; GGT: gamma-glutamyltransferase; TNM: tumor–node–metastasis; GPX2: glutathione peroxidase 2.
Tumor number indicates number of primary tumor mass detected at the time of surgical operation.

Comparison of GPX2 expression by TNM stage and BCLC stage. GPX2 expression is gradually increased as tumors progress in (a) TNM stage and (b) BCLC stage. Statistical analysis was performed by Student’s t-test.

Comparison of GPX2 expression in HCC patients with or without recurrence. GPX2 is overexpressed in (a) early recurrence and (b) late recurrence patients. Statistical analysis was performed by Student’s t-test.
Overexpression of GPX2 significantly associated with poor prognosis in HCC patients
To further confirm the effect of GPX2 expression on OS and TTR in HCC patients, we evaluated univariate analysis of traditional clinicopathological parameters for prognosis. Kaplan–Meier analysis revealed that high expression of GPX2, high AFP level, high GGT level, liver cirrhosis, larger tumor size, and vascular invasion were poor predictors for OS and TTR of HCC patients (all p < 0.05; Table 2). Significant OS and TTR advantages were observed for HCC patients with low GPX2 expression (both p < 0.001; Figure 4(a)). In addition, the median times of OS and TTR in GPX2 high-level group were 34.0 and 17.0 months, which were significantly lower than that of the GPX2 low-level group (58.0 and 57.0 months). Furthermore, the 5-year OS rate in GPX2 high-level group and GPX2 low-level HCC patient subgroups was 36.5% and 71.5%, while the 5-year TTR rate was 23.7% and 68.4% (Figure 4(a)).
Univariate and multivariate analyses of GPX2 associated with survival and recurrence in HCC patients.

GGT: gamma-glutamyltransferase; AFP: α-fetoprotein; OS: overall survival; TTR: time to recurrence; NS: not significant; HR: hazard ratio; CI: confidence interval; GPX2: glutathione peroxidase 2.
TNM stage and BCLC stage were combined with several clinical indexes such as tumor size, number, and tumor thrombus; we did not enter the TNM stage and BCLC stage into multiple analysis with these indexes to avoid any bias in analysis.
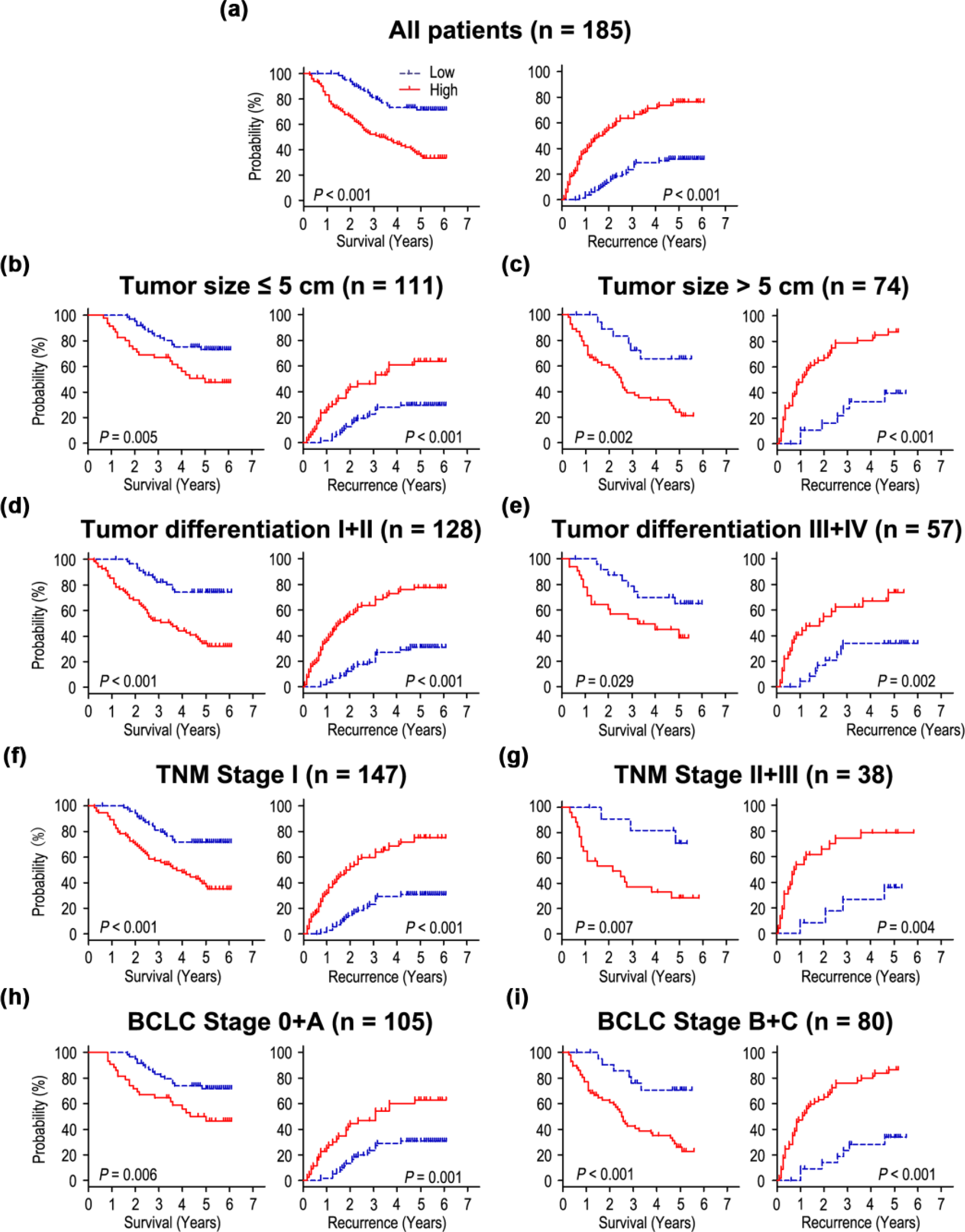
Overall survival and time to recurrence are shown for patients with HCC. All patients were stratified according to tumor size, tumor differentiation, TNM classification, and BCLC stage. Kaplan–Meier survival estimates and log-rank tests were used to analyze the prognostic significance of GPX2 expression in (a) all patients and (b–i) each subgroup.
Furthermore, we analyzed whether GPX2 could be an independent predictor for OS and TTR in HCC patients. A multivariate Cox model adjusted for AFP, GGT, liver cirrhosis, tumor size, vascular invasion, and GPX2 expression was performed. Our results showed that overexpression of GPX2 was an unfavorable predictor for OS in HCC patients (hazard ratio (HR) = 2.506, 95% confidence interval (CI) = 1.510–4.158, p < 0.001). In addition, the patients with high GPX2 expression was almost 3.3 times more likely to suffer from relapse than those with low GPX2 expression (HR = 3.365, 95% CI = 2.099–5.392, p < 0.001; Table 2).
To further investigate the prognostic value of GPX2 in different subgroups, patients were stratified according to tumor size (Figure 4(b) and (c)), tumor differentiation (Figure 4(d) and (e)), TNM stage (Figure 4(f) and (g)), and BCLC stage (Figure 4(h) and (i)). The high expression of GPX2 maintained its prognostic value in predicting shorter OS and TTR in all of these subgroups. Therefore, it has been suggested that GPX2 may serve as a potential prognostic biomarker for HCC patients in different risk groups.
Prognostic significance of GPX2 in early HCC patients
We further investigated the clinical significance of GPX2 on prognosis in early HCC patients. For the 147 TNM stage-I patients, significant correlation was found between GPX2 expression and OS (p < 0.001) and recurrence-free survival (RFS; p < 0.001; Figure 5). The association of OS and RFS with clinicopathological features and GPX2 expression in TNM stage-I HCC patients was shown in Table 3. In the Cox model adjusting for other prognostic variables, GPX2 was an independent negative prognostic factor for survival in TNM stage-I patients (Table 3). Patients with GPX2 overexpression had poorer OS (HR = 2.430, 95% CI: 1.405–4.204; p = 0.001) and TTR (HR = 3.427, 95% CI: 2.041–5.755; p < 0.001) than those with low GPX2 expression in TNM stage-I patients.

GPX2 overexpression indicates poor prognosis in TNM stage-I HCC patients. (a) Overall survival and (b) time to recurrence curves were generated based on the GPX2 protein expression statuses in 147 TNM stage-I patients.
Univariate and multivariate analyses of GPX2 associated with survival and recurrence in TNM stage-I HCC patients..

GGT: gamma-glutamyltransferase; AFP: α-fetoprotein; OS: overall survival; TTR: time to recurrence; NS: not significant; HR: hazard ratio; CI: confidence interval; GPX2: glutathione peroxidase 2.
Combined influence of GPX2 and serum AFP on risk of HCC death and recurrence
It has been known that serum AFP level is a poor prognostic factor for HCC patients. 23 Our results revealed that preoperative serum AFP level above 400 ng/mL was significantly associated with shorter OS (p < 0.001) and TTR (p = 0.001; Table 2). Therefore, we evaluated the prognostic value of GPX2 expression with serum AFP level for recurrence and survival of HCC patients. According to GPX2 expression and serum AFP level, HCC patients were divided into four subgroups with different survival and recurrent risks: group I with GPX2 (−) and AFP ≤ 400 ng/mL, good prognosis, and low risk of recurrence; group II with GPX2 (−) and AFP > 400 ng/mL; group III with GPX2 (+) and AFP ≤ 400 ng/mL, intermediate prognosis, and intermediate risk of recurrence; and group IV with GPX2 (+) and AFP > 400 ng/mL, poor prognosis, and high risk of recurrence (Figure 6). Multivariate analysis further demonstrated that the combination of GPX2/AFP was an independent prognostic factor for OS (HR = 1.648, 95% CI = 1.334–2.037, p < 0.001) and TTR (HR = 1.759, 95% CI = 1.453–2.130, p < 0.001; Table 4).
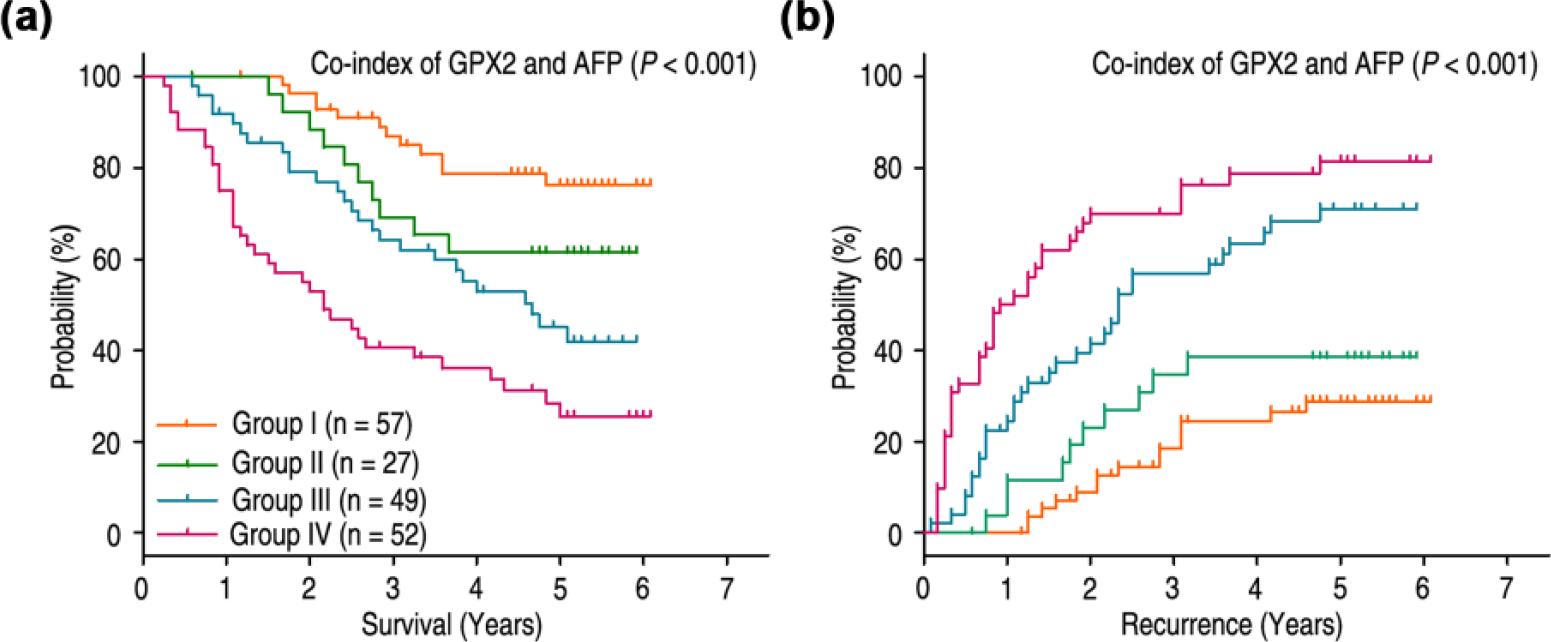
Combined influence of GPX2 and serum AFP on risk of HCC death and recurrence. (a) The associations of GPX2/AFP co-expression with overall survival (log-rank p < 0.001) and (b) time to recurrence (log-rank p < 0.001) in 185 HCC patients.
Univariate and multivariate analyses of co-index of GPX2/AFP associated with survival and recurrence in HCC patients.
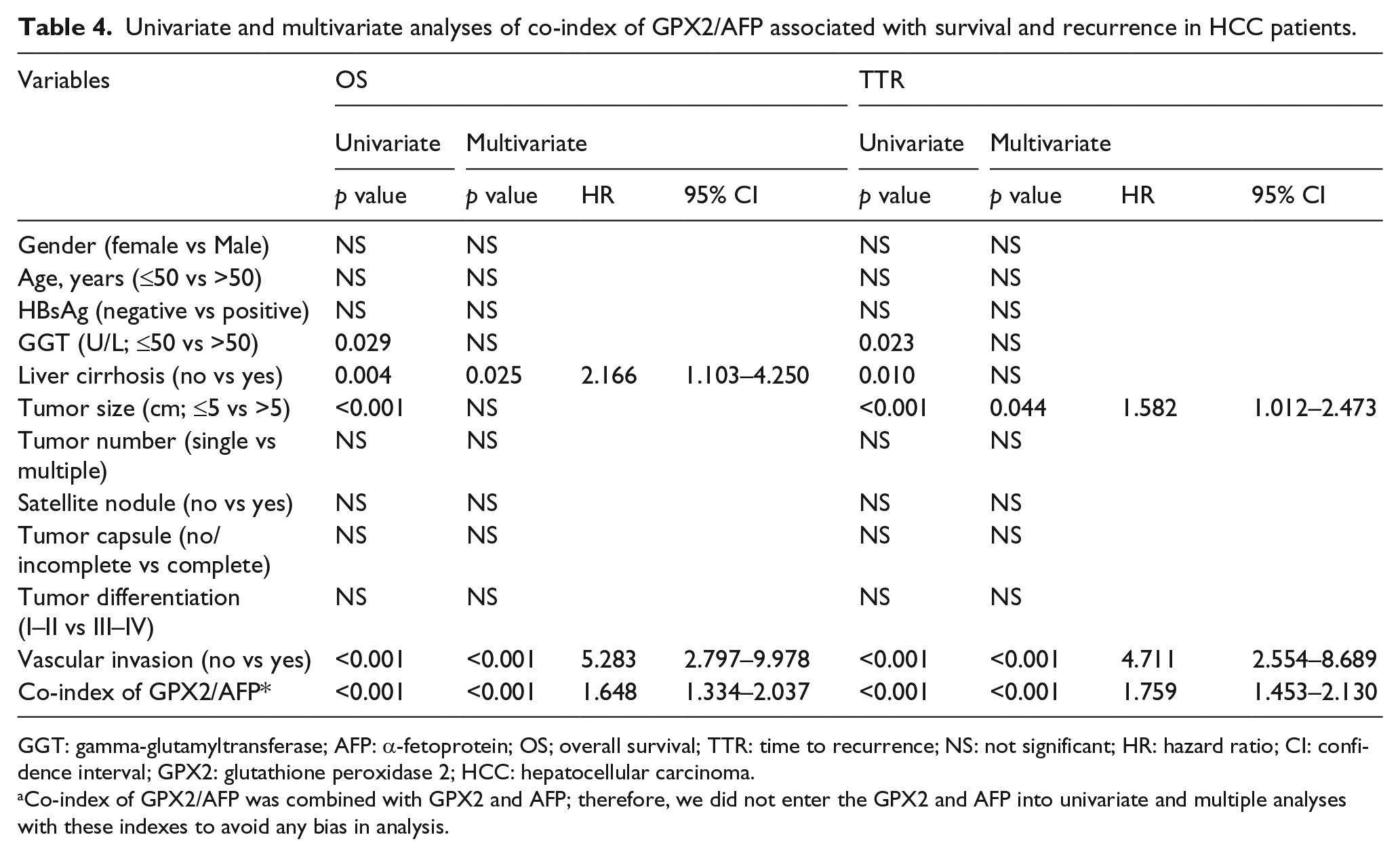
GGT: gamma-glutamyltransferase; AFP: α-fetoprotein; OS; overall survival; TTR: time to recurrence; NS: not significant; HR: hazard ratio; CI: confidence interval; GPX2: glutathione peroxidase 2; HCC: hepatocellular carcinoma.
Co-index of GPX2/AFP was combined with GPX2 and AFP; therefore, we did not enter the GPX2 and AFP into univariate and multiple analyses with these indexes to avoid any bias in analysis.
Discussion
GPXs are a family of antioxidant enzymes. The function of GPXs is to reduce H2O2 or organic hydroperoxides to water or their corresponding alcohols, respectively. 25 GPX2, as a member of GPX family, is specifically expressed within the gastrointestinal tract in human. 13 Importantly, GPX2 has an anti-inflammatory and anti-tumour effect in the course of the tumorigenesis. 26 It has been reported that GPX2 is related to the genesis of several types of cancer.11,17–19,27 However, the prognostic significance of GPX2 expression in HCC is still unclear. Our results revealed that GPX2 was upregulated in HCC tissues compared with that in adjacent non-tumorous tissues. In addition, GPX2 overexpression was correlated with high AFP level, larger tumor, BCLC stage, and tumor recurrence. Moreover, the levels of GPX2 expression were both higher in the early and late recurrence groups, compared with those in no recurrence groups. In addition, the Kaplan–Meier survival analysis found that GPX2 overexpression was an independent predictor for poor OS and TTR in HCC patients. Furthermore, we also estimated the prognostic value of GPX2 in different subgroups according to tumor size, tumor differentiation, TNM stage, and BCLC stage, which suggested that GPX2 may work as a powerful prognostic factor for patients with HCC in different risk groups. The results indicate that GPX2 could serve as a feasible prognostic biomarker of HCC. In several investigations, it has been shown that the abnormal expression of GPX2 in cancer cells is associated with tumor progression. Suzuki et al. 15 reported that the GPX2 was overexpressed in the most metastatic features of HCC cell lines. GPX2 small interfering RNA (siRNA) could inhibit HCC cell proliferation, suppress cell migration and invasion, and reduce the secretion of matrix metalloproteinase 9. Naiki et al. 20 investigated the role of GPX2 in castration-resistant prostate cancer and found that GPX2 promoted cell proliferation by the way of cyclin B1-dependent G2/M arrest. Moreover, patients with GPX2 overexpression in biopsy specimen had poorer prognosis than those with low GPX2 expression. However, Chang et al. 22 revealed that GPX2 protein underexpression was associated with advanced pT status, nodal metastasis, high histological grade, vascular invasion, and frequent mitoses in urothelial carcinoma. Decreased GPX2 could be an unfavorable predictor for urothelial carcinoma. Our findings and previous observations strongly implicate that GPX2 expression is involved in the tumor progression and may serve as a prognostic factor for HCC patients.
The International Union Against Cancer’s TNM staging is one of the most important factor to estimate the prognosis of HCC patients. The TNM system has successfully graded patients on their prognosis according to the clinicopathological features. However, it has reached its limit in providing critical information that may influence treatment strategy. It is difficult for surgeons to predict who will suffer relapse in early-stage patients who received curative treatment. To overcome the limitations of these traditional systems, many molecular markers have been reported and shown to have potential predictive significance. However, so far, molecular markers that could stratify TNM stage-I HCC patients are still substantially limited. In our results, we found that GPX2 was an independent negative prognostic factor for survival in TNM stage-I patients. These results suggest that GPX2 could serve as a predictive tool to identify patients with TNM stage I at high risk of recurrence.
Previous study reported that AFP, as a tumor-associated antigen, could be used for diagnosis and predicted prognosis of HCC and monitor tumor recurrence in HCC patients with high AFP level after hepatectomy.28,29 However, it is difficult to predict the prognosis and recurrence in normal AFP HCC patients after hepatectomy. To estimate whether the prognostic value of GPX2 combined with serum AFP level was superior to AFP alone, we divided the HCC patients into four groups according to GPX2 expression and serum AFP level and found that combination of GPX2 and serum AFP level could be used for predicting the risk of tumor recurrence and survival of patients. HCC patients can be classified into different subgroups with different risks of tumor recurrence and prognosis based on GPX2 expression in HCC tissue and preoperative AFP level. Therefore, the simultaneous analysis of GPX2 expression and serum AFP level may help determine whether adjuvant therapy is required after resection.
In summary, we proved that GPX2 may work as a feasible biomarker for prognostic prediction in HCC patients. Moreover, GPX2 could be a predictive tool to identify patients with TNM stage I at high risk of recurrence. The combination of GPX2 with serum AFP level may help to identify the high-risk HCC patients after hepatectomy. The findings of this study may help to determine optimal treatment strategies. However, it also requires further studies to clarify the underlying biology of GPX2 in the development of HCC.
Footnotes
Acknowledgements
The authors gratefully acknowledge the clinical data provided by the Pathology Department (Cancer Center, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology). T.L. and X.-f.K. have equally contributed to this project. J.Y. and P.-d.L. have jointly supervised this work. We would like to thank Mrs. Lorraine Medoro for proofreading and insightful views (Radiation Department, Fox Chase Cancer Center).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was primarily supported by National Natural Science Foundation of China (no. 81502697 to P.D.L.; no. 81601578 to X.F.K.; no. 81202460 to J.Y.), the Natural Science Foundation of Hubei Province (no. 2016CFB374 to P.D.L.; no. 2015BCA270 to J.Y.; no. 2014CFB404 to J.Y.). Also, this work was partially supported by the Independent Innovation Research Foundation of Huazhong University of Science and Technology (no. 01-08-530059 to P.D.L.) and the Union Hospital Key Laboratory Foundation of Biological Target Therapy (no. 02.03.2013-80 to P.D.L.).