
Abstract
To investigate hypoxia-induced factor-1 alpha expression in distinct oral squamous cell carcinoma subtypes and topographies and correlate with clinicopathological data. Hypoxia-induced factor-1 alpha expression was assessed by immunohistochemistry in 93 cases of OSCC. Clinical and histopathological data were reviewed from medical records. Hypoxia-induced factor-1 alpha status was distinct according to tumor location, subtype and topography affect. In superficial oral squamous cell carcinomas, most tumor cells overexpressed hypoxia-induced factor-1 alpha, whereas hypoxia-induced factor-1 alpha was restricted to the intratumoral region in conventional squamous cell carcinomas. All basaloid squamous cell carcinomas exhibited downregulation of hypoxia-induced factor-1 alpha. Interestingly, metastatic lymph nodes (91.7%, p = 0.001) and the intratumoral regions of corresponding primary tumors (58.3%, p = 0.142) showed hypoxia-induced factor-1 alpha-positive tumor cells. Overall survival was poor in patients with metastatic lymph nodes. Hypoxia-induced factor-1 alpha has distinct expression patterns in different oral squamous cell carcinoma subtypes and topographies, suggesting that low oxygen tension promotes the growth pattern of superficial and conventional squamous cell carcinoma, but not basaloid squamous cell carcinoma. Indeed, a hypoxic environment may facilitate regional metastasis, making it a useful diagnostic and prognostic marker in primary tumors.
Keywords
Introduction
Oral squamous cell carcinoma (OSCC) represents more than 90% of all malignancies of the head and neck and mostly affects floor of the mouth and tongue.1,2 Middle-aged males are more frequently affected, and tobacco consumption is the primary cause. 3 According to TNM staging and Broder’s grading system, prognostic factors include tumor size and location, nodal status, and poor histological grade. 2 The pattern of the invasive front may predict tumor spread and prognosis, although the biological changes and molecular mechanisms that affect the tumor microenvironment remain unclear. 4
Low oxygen tension plays a crucial step in the self-renewal, metastatic potential and therapy resistance of cancers. Hypoxia-induced factor-1 alpha (HIF-1 alpha) is expressed in niches of tumor cells, where it mediates invasion and metastasis. 5 Hypoxic conditions may occur due to changes in neoplastic cells and angiogenesis.4,6 HIF-1-induced genes are involved in a wide range of cellular functions associated with tumor development and growth. 7 To adapt to the hypoxic microenvironment, neoplastic cells activate HIF-1 alpha, which dimerizes with the beta subunit (HIF-1 beta) and targets several genes, such as those mediating angiogenesis.6,8 Under hypoxia, HIF-1 alpha is stabilized and is expressed in both the cytoplasm and nucleus. In oxygenated tissue, its degradation is mediated by ubiquitination via the von Hippel–Lindau tumor suppressor.8,9
Several studies have recently shown that HIF-1 alpha expression has role in the malignant progression of oral and head and neck carcinomas, facilitating the adaptation of cells to hypoxia as well as contributing to the invasive properties, cell survival, and angiogenesis in these tumors.1,4,10 Resistance to therapy and poor patient outcomes have also been correlated with tumor hypoxia in several cancers, including lung, breast, prostate, and glioma.5,9,11–13 In OSCC, the relevance of HIF-1 alpha is still controversial. 14 Some studies associate its expression with poor survival, tumor progression, and regional metastasis.15–18 A high density of microvasculature was also correlated with the overexpression of HIF-1 alpha.15,19 However, other authors demonstrated that HIF-1 alpha overexpression is associated with good patient outcome19–21 and the early stages of malignant transformation. 15 The aim of this study was to analyze HIF-1 alpha expression in distinct OSCC subtypes and topographies and to correlate with clinicopathological data.
Materials and methods
Specimens
Paraffin blocks from 93 patients treated surgically for OSCC at the Araujo Jorge Hospital in Goiânia, GO, Brazil, between 2000 and 2006 were selected for this study. In all, 36 lymph node specimens were also included. Only specimens from patients with no prior treatment were eligible and grouped according to microscopic subtypes as follows: superficial OSCC (n = 22), conventional SCC (n = 62), and basaloid squamous cell carcinomas (BSCCs; n = 9). Superficial OSCC was defined as depth of invasion ≤4 mm. 2 Conventional OSCC and BSCC were analyzed in two distinct topographic zones: intratumoral and invasive front. Invasive front was determined as sheets, strands, cords, or single tumor cells in contact with normal tissue on the tumor edge. Patients were followed up for 1–110 months, with a mean of 35.1 months. Clinicopathological data such as gender, age, ethnicity, smoking and alcohol, tumor location, tumor staging (TNM), microscopic type, tumor grade, treatment, and monitoring of patients were analyzed. Histological grading based on Broder’s classification was indicated by the World Health Organization. 2 This study was approved by the Research Ethics Committee of the Federal University of Goiás, Brazil, and informed consent was obtained from all individual participants included in the study.
Immunohistochemical analysis
Paraffin blocks of 93 patients with OSCC were sectioned at 3 µm and immunohistochemically stained using the avidin–biotin–peroxidase complex technique (Starr Trek Universal HRP Detection System; Biocare Medical, LCC, Concord, CA, USA). Initially, the sections were deparaffinized and heated in Tris-EDTA buffer solution in a steamer for 30 min to retrieve the antigenicity and then incubated with 10 mg/mL (1:100) rabbit monoclonal HIF-1 alpha antibody (Cell Signaling Technology, Danvers, MA, USA) for 1 h, according to the manufacturer’s recommendations. Subsequently, the sections were treated with 3% H2O2 in order to inhibit the endogenous peroxidase, incubated with secondary antibodies, and finally visualized by a diaminobenzidine substrate kit for 5 min. Slides were assembled, counterstained with hematoxylin, and examined by light microscopy. Kidney samples were used as positive controls, and negative controls were achieved by omitting the primary antibody. Immunostains were analyzed by two independent observers, blinded to the clinical data. At least 1000 tumor cells were counted in 10 randomly selected high-power fields of 400×. 15 HIF-1 alpha expression was analyzed quantitatively and semi-quantitatively. The percentage of positive tumor cells was categorized as follows: 0 (absence), 1 (≤25%), 2 (>25% to ≤50%), 3 (>50% to ≤75%), and 4 (≥75%). 11 The relative staining intensity was scored as 0 (no stain), 1 (weak), 2 (moderate), or 3 (high). The product of the intensity and percentage was calculated as a final score as follows: (0) absent, (1–4) low, and (6–12) high.
Statistical analysis
One-way analysis of variance (ANOVA), chi-square tests, and linear regression analyses were used to compare the differences between groups (p ≤ 0.05). Multivariate logistic Cox regression was used for multivariate tests (odds ratio (OR)) and confidence interval (CI ≥ 95%). Survival curves were plotted using the Kaplan–Meier method and p values were calculated using log-rank tests. Statistical calculations were performed using the Statistical Package for the Social Science (SPSS, Chicago, IL, USA), version 15.
Results
Clinicopathological data
Clinicopathological data of 93 OSCC patients are summarized in Supplementary Table S1. Males were predominant (76.3%), with ages range from 31 to 80 years (mean 56.3 years). Tobacco use was registered in 73.1% of patients and concomitant use of alcohol was recorded in 45 cases (48.4%). The tongue and floor of the mouth were the most affected locations (61.3%). Based on TNM classification, the majority of the tumors presented as T3–T4 (54.8%). These tumors spread to the cervical lymph nodes in 35.5% cases and systemic metastasis was detected in 9.7% cases. Microscopically, three tumor subtypes were analyzed as follows: conventional SCC (66.7%), BSCC (9.7%), and superficial OSCC (23.6%). Conventional SCC was graded as well (30.6%), moderately (54.8%), or poorly differentiated (14.5%). Surgery was the most common therapy (40.9%), followed by radiotherapy (33.3%) and radiotherapy/chemotherapy (20.4%). Recurrence was observed in 38.7% of cases.
HIF-1 alpha expression varies according to tumor subtype and topography
Typical microscopic features of superficial OSCC, conventional SCC, and BSCC are highlighted in Figures 1 and 2. HIF-1 alpha immunostaining was observed in the cytoplasm and nuclei of tumor cells and its expression varied among tumor subtypes. No expression was registered in normal mucosa (Figure 1(a) and (b)). In superficial OSCC, most neoplastic cells showed high HIF-1 alpha expression (Figure 1(c) and (d) and Table 1). High expression of HIF-1 alpha was observed in the intratumoral region in 56.5% of conventional SCC (Figure 2(b) and Table 2). In contrast, only 22.2% of BSCC cases showed HIF-1 alpha expression (Figure 2(d) and Table 2), suggesting a distinct biology among tumor subtypes.

HIF-1 alpha expression in early OSCC. (a) Normal oral mucosa (hematoxylin and eosin). (b) Absence of HIF-1 alpha expression in normal oral mucosa. (c) Superficial OSCC measuring less than 4 mm. (d) HIF-1 alpha positivity in most tumor cells in superficial OSCC.
HIF-1 alpha expression in superficial OSCC.
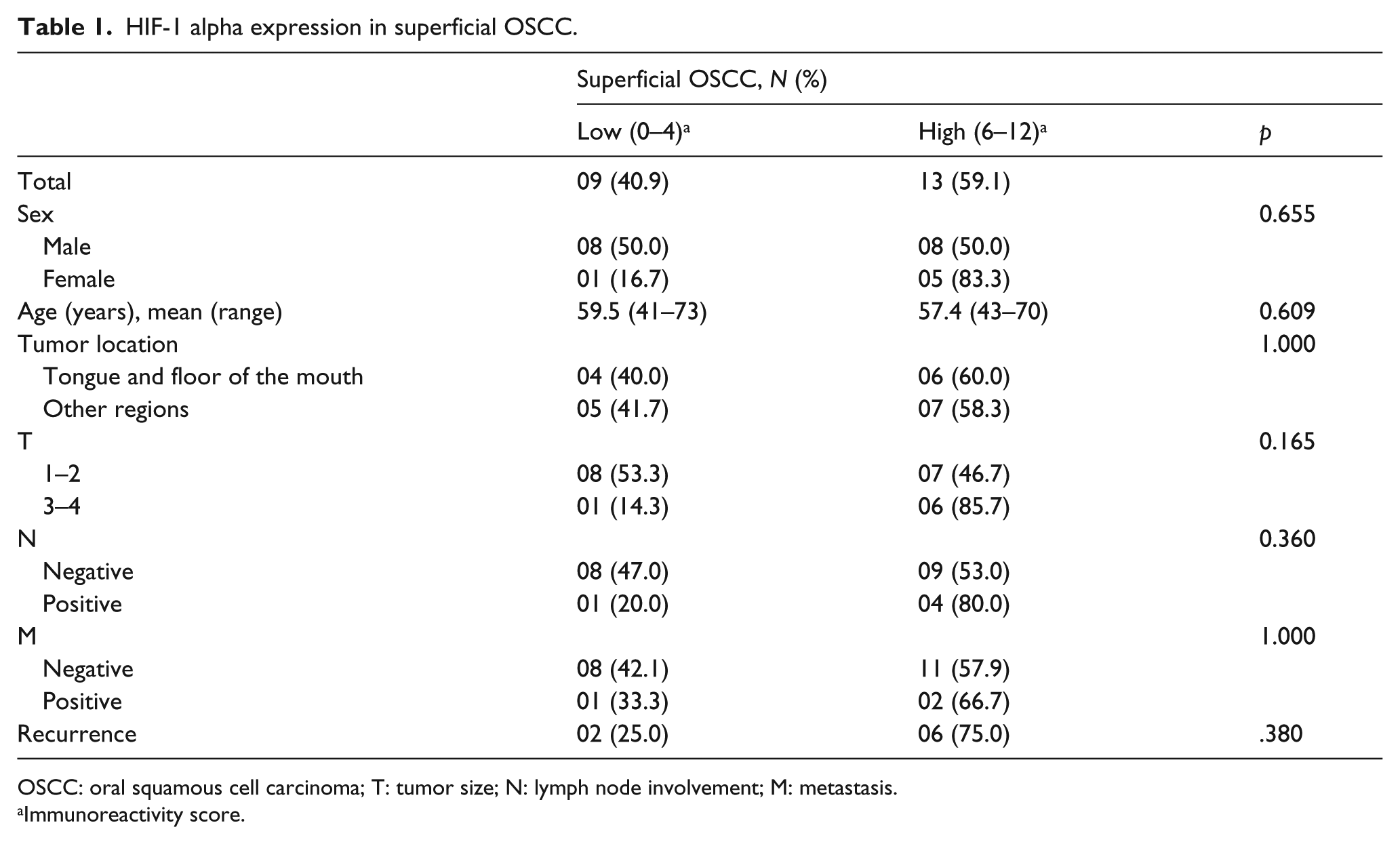
OSCC: oral squamous cell carcinoma; T: tumor size; N: lymph node involvement; M: metastasis.
Immunoreactivity score.

Differential HIF-1 alpha expression in more invasive OSCC. (a) Typical microscopic features of conventional SCC with keratinization and (b) showing high expression of HIF-1 alpha intratumorally. (c) BSCC showing central comedo necrosis (H&E) and (d) HIF-1 alpha positivity only in the dysplastic cells of surface mucosa. (e) Clots of neoplastic cells within afferent lymphatic vessels (H&E) and (f) showing HIF-1 alpha–positive metastatic cells.
HIF-1 alpha expression in intratumoral region and at invasive front of conventional SCC and BSCC.
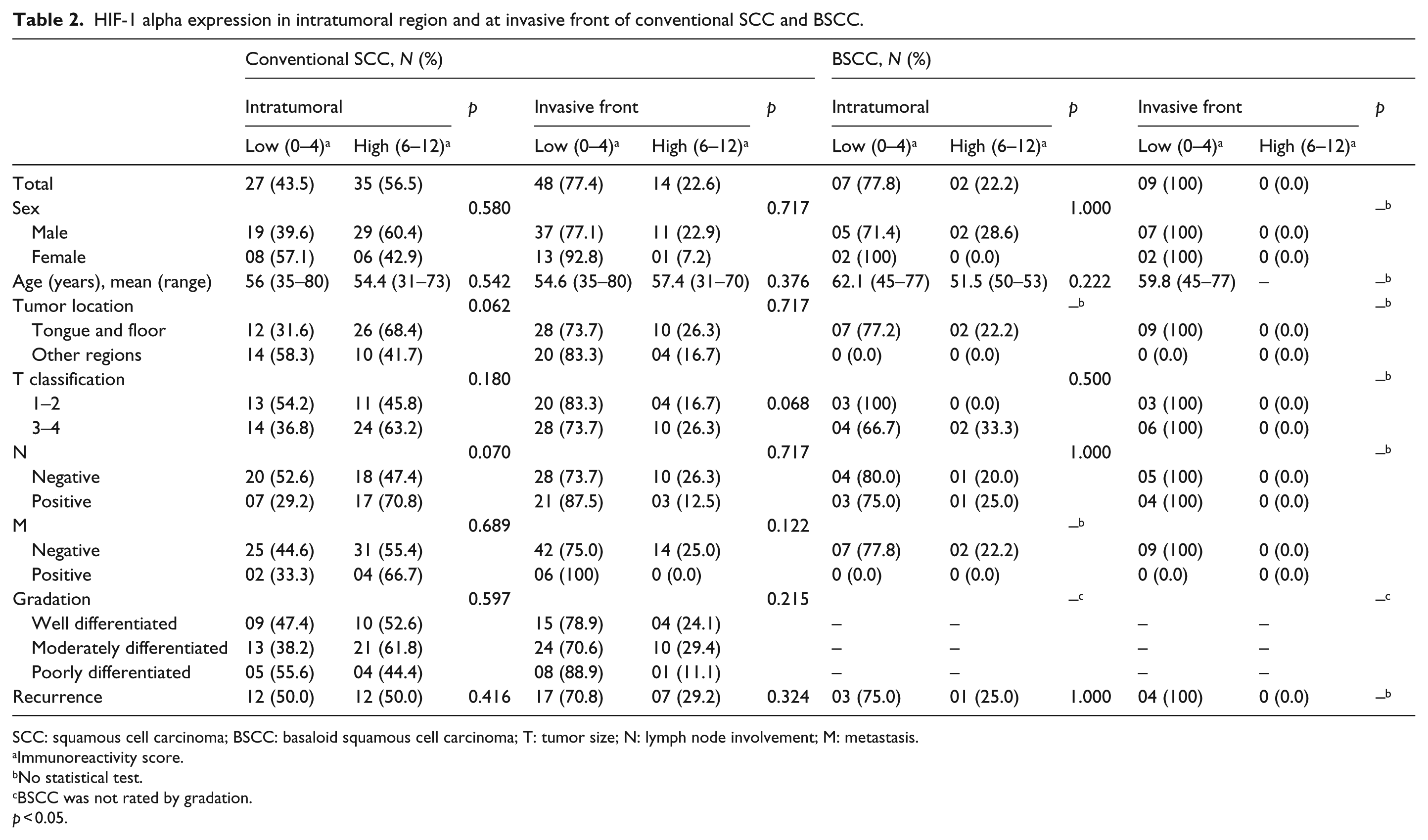
SCC: squamous cell carcinoma; BSCC: basaloid squamous cell carcinoma; T: tumor size; N: lymph node involvement; M: metastasis.
Immunoreactivity score.
No statistical test.
BSCC was not rated by gradation.
p < 0.05.
Risk of death and survival rate are independent of HIF-1 alpha expression
Analysis of the results obtained indicated a higher risk of death due to nodal involvement (p = 0.020; OR = 2.843; interaction contrast (CI) = 1.183–6.834) and independent of HIF-1 alpha expression (Table 3). No increased risk of death was attributable to HIF-1 alpha expression to tumor subtype, gradation, or recurrence. Overall survival was higher in superficial OSCC, followed by conventional SCC and BSCC (p = 0.436; Figure 3(a)). The survival time ranged from 1 to 110 months. Patients with BSCC survived up to 12 months (Figure 3(d)). Metastatic tumors correlated with a poor survival (p = 0.011).
Correlation of clinicopathological data and risk of death.

OSCC: oral squamous cell carcinoma; SCC: squamous cell carcinoma; BSCC: basaloid squamous cell carcinoma; T: tumor size; N: lymph node involvement; M: metastasis.
OR: relative risk.
95% CI: confidence interval.
Statistical analysis, multivariate Cox test *p < 0.005.

Kaplan–Meier survival analysis and HIF-1 alpha expression in patients with OSCC. (a) Overall survival rate according to tumor subtype. (b) Significantly high survival rate in HIF-1 alpha–positive superficial OSCC. (c) Better patient outcome in invasive OSCC with high HIF-1 alpha expression. (d) Survival curves of BSCC showing poor survival rate in patients with low HIF-1 alpha expression. (e) Poor patient outcome in nodal metastasis with HIF-1 alpha–positive neoplastic cells.
Metastatic neoplastic cells and their respective primary tumors overexpressed HIF-1 alpha
Nodal involvement was immunohistochemically analyzed in 24 cases (Table 4), which mostly spread from conventional SCC (79.2%), superficial OSCCs (12.5%), and BSCC (8.3%). Interestingly, HIF-1 alpha–positive tumor cells were detected in 91.7% (p < 0.001) of metastatic lymph nodes regardless of tumor subtype (Figure 2(e)). Additionally, HIF-1 alpha–positive neoplastic cells were detected inside afferent lymphatic vessels (Figure 2(f)). HIF-1 alpha immunostaining pattern in nodal invasion was similar to that of corresponding primary tumors. Interestingly, expression of HIF-1 alpha was high in the corresponding primary tumors (58.3%). These data were significant in superficial OSCCs (p < 0.001; Table 4). Low HIF-1 alpha expression was concomitant with highly keratinized metastatic tumors. Although HIF-1 alpha expression was typically low in the invasive front region (p = 0.003), metastatic BSCC showed high expression of HIF-1 alpha inside corresponding primary tumors.
HIF-1 alpha expression in metastatic lymph nodes and the primary tumor.

OSCC: oral squamous cell carcinoma; SCC: squamous cell carcinoma; BSCC: basaloid squamous cell carcinoma.
Immunoreactivity score.
No statistical test due to small sample.
p < 0.005.
Discussion
Low oxygen tension seems to be an important factor in increasing the risk of metastasis and mortality in cancer. The hypoxic environment induces HIF-1 alpha transcriptional activity in niches of stem-like tumor cells, regulating the expression of several genes, including those involved in angiogenesis, glucose metabolism, and cancer cell invasion and metastasis. 4 HIF-1 alpha overexpression has been correlated with poor prognosis in cancers from the lung, breast, prostate, and glioma.9,11–13,22,23 In OSCC, the clinical relevance of the hypoxic condition is still controversial. 14 Some studies have correlated high levels of HIF-1 alpha with poor prognosis, tumor progression, and regional metastasis.4,6,15–18 Other authors reported HIF-1 alpha as a predictor of good patient outcome.15,19 In addition, HIF-1 alpha expression has been reported in the early stages of OSCC and in proximal dysplastic epithelium.19–21,24
In this study, HIF-1 alpha had different expression patterns in different OSCC subtypes and topographies. No other clinical data were correlated with HIF-1 status. Superficial OSCC showed overexpression of HIF-1 alpha in most tumor cells, suggesting its role in growth pattern in the early stages of development. Some authors have shown that high HIF-1 alpha expression is correlated with early transformation, indicating that HIF-1 alpha is a marker of cancer risk.14,21 Moreover, Mendes et al. 25 suggested strong expression in tumor margins, which defines a high risk independent of any other factor. In conventional SCC, heterogeneous expression of HIF-1 alpha was registered intratumorally, suggesting this protein plays an important role in progression from precursor lesions to invasive cancer. Indeed, BSCC seems to have a distinct growth pattern independent of HIF-1 alpha expression. Therefore, each OSCC subtype appears to have a distinct microenvironment and behavior.
The hypoxic environment seems to drive metastasis in several tumors. In oral SCC, HIF-1 alpha expression correlates with nodal involvement. 15 Herein, high HIF-1 alpha expression was associated with nodal metastasis, a process that probably involves the intratumoral region, suggesting a metastatic process under the hypoxic condition. Further studies are required to determine the plasticity of metastatic cells and their behavior in primary tumors.
An increased risk of mortality has been associated with increased HIF-1 alpha expression in several cancers. 25 In OSCC, the clinical relevance of low oxygenation in primary tumors is controversial regarding patient prognosis. Disease-free survival is associated with high HIF-1 alpha levels.19,20 However, in this study, Kaplan–Meier analysis showed that low oxygen tension is associated with better prognosis. 26 A multivariate analysis of overall survival showed a twofold increased risk of death in patients with regional nodal involvement. Similar results were reported by Eckert et al. 16 and Liang et al. 15 No positive correlation was observed between HIF-1 alpha expression and patient outcome. However, the survival rate is lower when HIF-1 alpha is overexpressed in the primary tumor. Further studies on OSCC are required to achieve a clearer understanding of the biological changes that are involved in cancer cell adaptation to a hypoxic environment and that are essential for proliferation and metastatic spread.
In conclusion, low oxygen tension seems to be involved in the growth pattern in early OSCC and in intratumoral niches of conventional OSCC, but not in BSCC. Indeed, the results obtained suggest that the regional metastasis driven by hypoxic environment in conventional OSCC may facilitate regional metastasis.
Footnotes
Declaration of conflicting interests
M.R. has received research grants through Company Coordenação de Aperfeiçoamento Pessoal de Nível Superior (CAPES) scholarship from Brazil.
Funding
This study was funded by CNPq-Conselho Nacional de Desenvolvimento Científico e Tecnológico, Brazil (No. 471879/2012-6 Universal 14/2012).