
Abstract
Background:
Neonatal death is often a harrowing experience for the parents, and bereavement is one of the most important life events for them.
Aim of the Study:
This study aims to quantitatively estimate the grief experienced by the parents after the death of their neonate and to describe it qualitatively.
Methods:
This mixed-methods descriptive study was done in an urban public hospital in South India from July’2024 to December’2024. Focus Group Discussions and In-Depth Interviews were conducted, 1 to 2 months after the death of the neonate (n = 54). The study tool used was the Perinatal Grief Scale to estimate the grief quantitatively. For qualitative analysis, the parents were asked to describe their experiences in the three themes of active grief, despair, and difficulty coping.
Results:
Significantly higher number of mothers had a total score of 91 and above than the fathers (P = .0032). The mothers had significantly higher mean total and sub-scale scores than the fathers.
Introduction
Neonatal death refers to deaths occurring in neonates less than 28 days of life. As per the World Health Organisation fact sheet, about 2.3 million neonates died globally in the year 2022.[1] India has significantly reduced neonatal deaths in the past few decades. It is close to achieving the Sustainable Development Goal of reducing the Neonatal Mortality Rate to 12 per 1,000 live births by 2030. However, a few states like Kerala and Tamil Nadu have already achieved this goal.[2]
Neonatal death is often a harrowing experience for the parents, and bereavement is one of the most important life events for them. Grief following neonatal death is a global phenomenon and is seen across all cultures, races, and countries.[3] It has been associated with mental health disturbances like anxiety, depression, post-traumatic stress, and suicide. The grief following neonatal death is dynamic and varies from person to person and from time to time. The severity of grief is determined by various factors like age, gender, literacy, social support, socio-economic class, and anticipatory grieving time.[4,5] The intensity of the grief decreases over time, usually within 6–12 months. In some parents, it may persist for about 24 months. In the literature, the term Complicated Grief is often used to describe severe forms of grief, which is characterised by prolonged grief of more than 12 months in duration, where the individual is not able to accept the death psychologically and integrate death into life.[6]
In developed countries, many studies have analysed grief reactions, their incidence, associated factors, and the various coping mechanisms available to the parents.[7,8] However, only a few studies have measured grief following a neonatal loss and studied the coping mechanisms in the Indian population.[3,9] In developed countries, targeted bereavement and grief counselling programs are often available for the parents to cope with their neonatal loss.[8,10] However, such bereavement care is not available for parents in the rest of the world. Despite the higher number of neonatal deaths in developing countries, structured grief counselling and coping programs are not available in most neonatal care units, leaving the parents at risk for various psychological problems.[11]
Aims and Objectives
This study aims to quantitatively estimate the extent of grief experienced by the parents after the death of their neonate and to describe qualitatively the grief experienced in three themes—active grief, despair, and difficulty coping—in an urban public hospital in South India.
Methods
This mixed-methods descriptive study was done in an urban public hospital in South India from July’2024 to December’2024. The study hospital is a public hospital run by the state government, and treatment is free to all patients admitted. Convenient sampling was done of all the parents who had their neonatal deaths in the neonatal unit of the study hospital during the study period. The parents who were not willing and those who could not be traced were excluded. In this study, we adopted both a quantitative and a qualitative research design to measure the extent of grief experienced by the parents and to describe it qualitatively in terms of active grief, despair, and difficulty coping. Focus Group Discussions (FGD) and In-Depth Interviews (IDI) were conducted in the hospital, 1 to 2 months after the death of their neonate. Prior intimation and appointment with the investigator were scheduled over the telephone. The sixth author conducted a one-to-one interview on the day of the appointment. Only one author interviewed the parents to avoid bias. Both parents were interviewed separately. Consent was obtained from the parents. Institutional human ethics committee approval was obtained.
The study tool used was the Perinatal Grief Scale (PGS) to quantitatively estimate the extent of grief.[12] The PGS was widely used in many studies worldwide and in India.[13–15] It has 33 questions in 3 sub-scales of active grief, despair, and difficulty coping. There were 11 questions on each sub-scale. Each question is scored from 0 (strongly agree) to 5 (strongly disagree) on the Likert scale. The higher scores were associated with severe grief, and a score of 91 or above was considered a high degree of grief.[16] For qualitative analysis, the parents were asked to describe their experiences in the three themes described earlier in their own words. Open-ended questions were asked to describe their experiences in three themes.
Statistical Analysis
Statistical analysis was done using R software. All categorical data were presented using frequencies and percentages. Continuous data were described using mean ± standard deviation after assessing the normality assumption with the Shapiro-Wilk test. The mean PGS scores were compared across different categorical demographic and clinical parameters. Variables with 2 levels were assessed using an independent sample t-test, and one-way ANOVA was used for variables having more than two levels. The Chi-square test of independence was used when comparing categorical frequencies between two groups. The non-normal continuous parameters were compared by computing the Spearman Correlation Coefficient or by a two-sample t-test with equal variances, after confirming that the variances were not significantly different with an F-test. The P value was considered significant at a 5% significance level for all comparisons.
Results
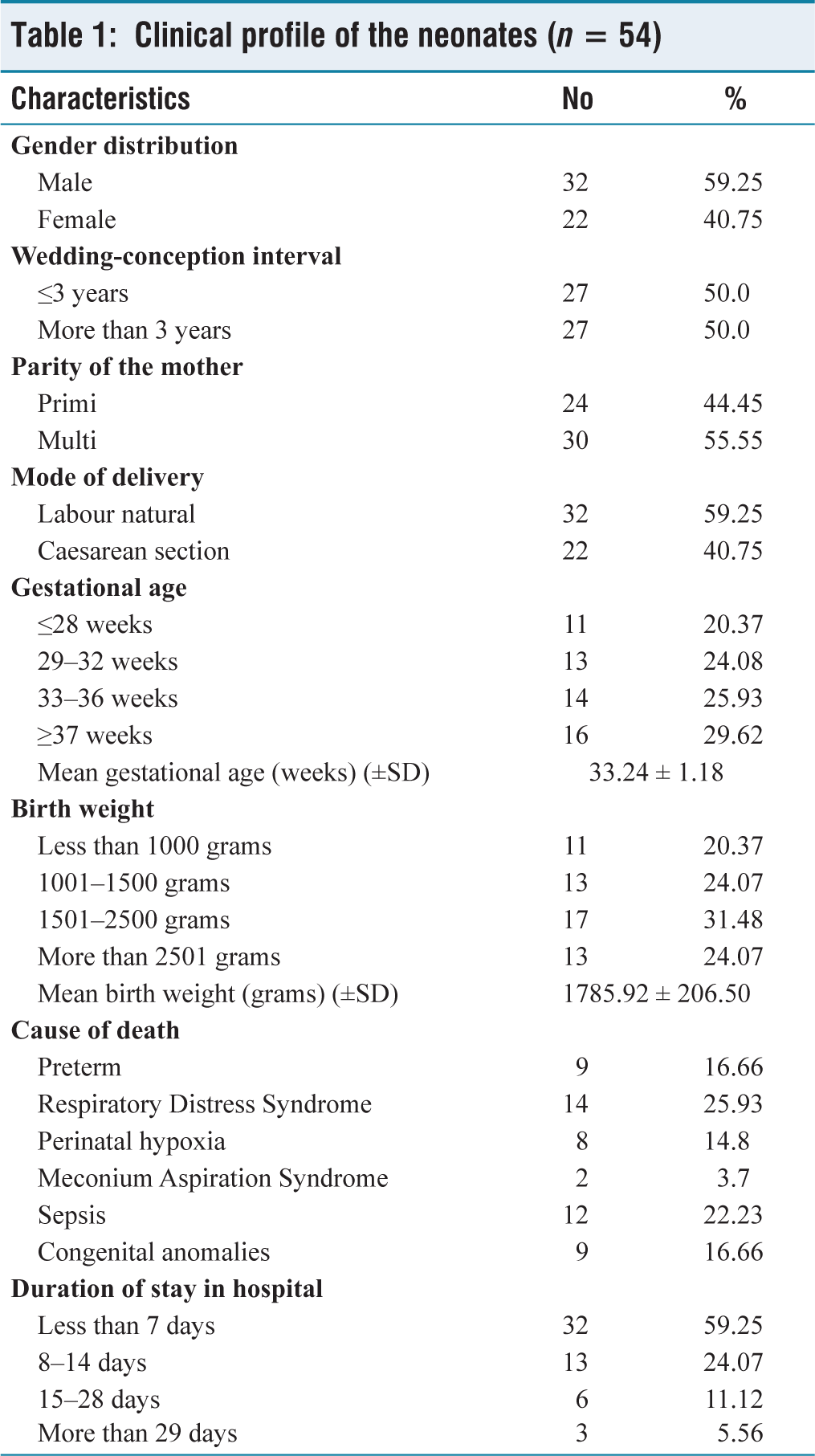
During the study period, there were 2,218 admissions in the neonatal unit, and 146 deaths were reported. After excluding the parents who were not willing and the parents who did not turn up for the interview, the parents of 54 neonates who expired during the study period formed the study group. The clinical profile of neonatal deaths is shown in Table 1, and the socio-demographic profile of the parents is shown in Table 2. On analysing the clinical profile of the neonates who died, about 59.25% were male, and 59.25% were born by natural labour. About 70.38% were preterm neonates, and about 75.93% had a birth weight of less than 2,500 grams. The mean gestation age of the neonates in the study group was 33.24 ± 1.18 weeks, and the mean birth weight was 1,785.92 ± 206.50 grams. On analysing the cause of death, 25.93% of deaths were due to RDS and about 16.66% were due to prematurity. Congenital anomalies like congenital diaphragmatic hernia and congenital heart diseases were the cause of death in 16.66% of deaths. About 59.25% of neonates stayed in the hospital for less than 7 days, and 5.56% of neonates stayed for more than 28 days. About 7 neonates (13%) were born after Assisted Reproductive Treatment (ART) or after previous neonatal deaths for the parents.
Clinical profile of the neonates (n = 54)
Socio-demographic profile of the parents (n = 54)
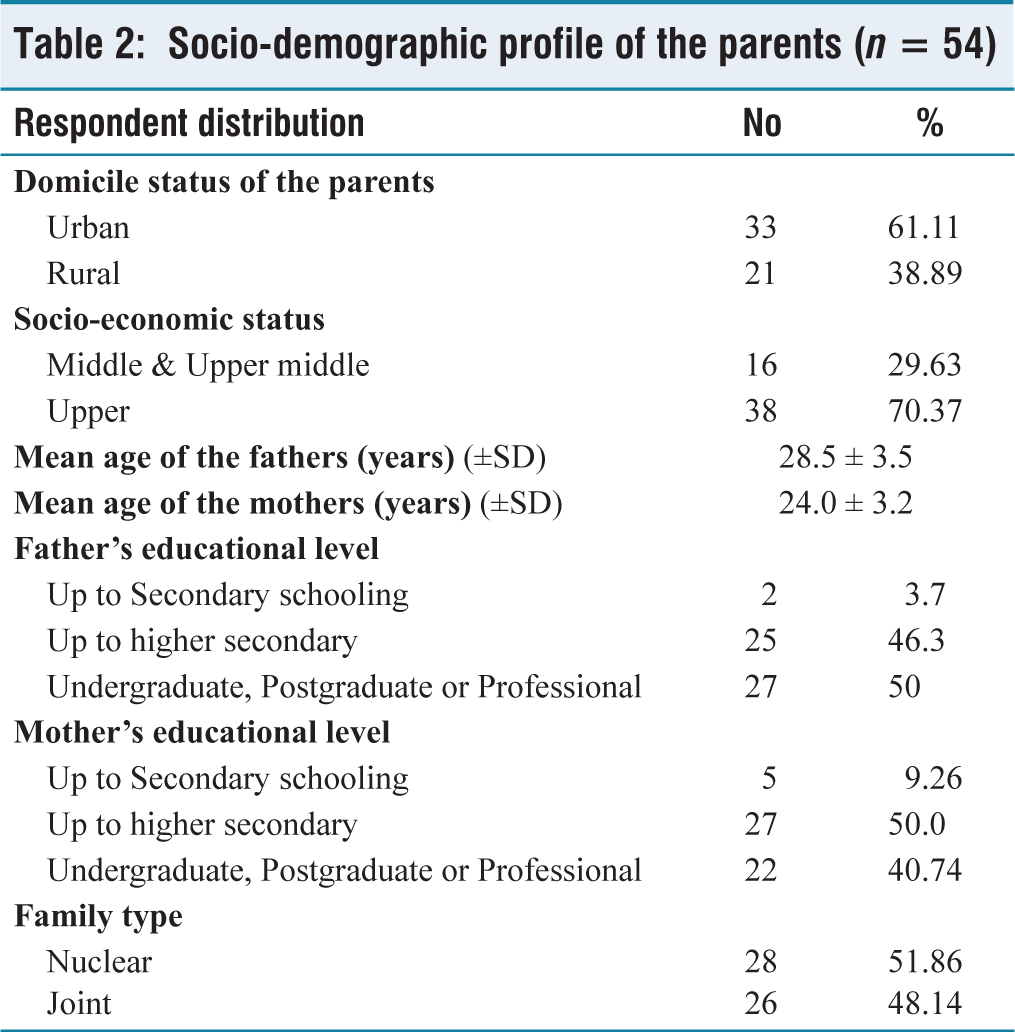
Analysing the demographic profile of the parents, about 38.89% of them hailed from rural areas, and 70.37% of them were from the upper socioeconomic class, as per the Modified BG Prasad Scale. The mean ages of the fathers and mothers were 28.5 ± 3.5 years and 24.0 ± 3.2 years, respectively. About 48.14% of fathers and 38.88% of mothers had an undergraduate level of education. About 51.86% of parents were living in a nuclear family.
Quantitative Estimates
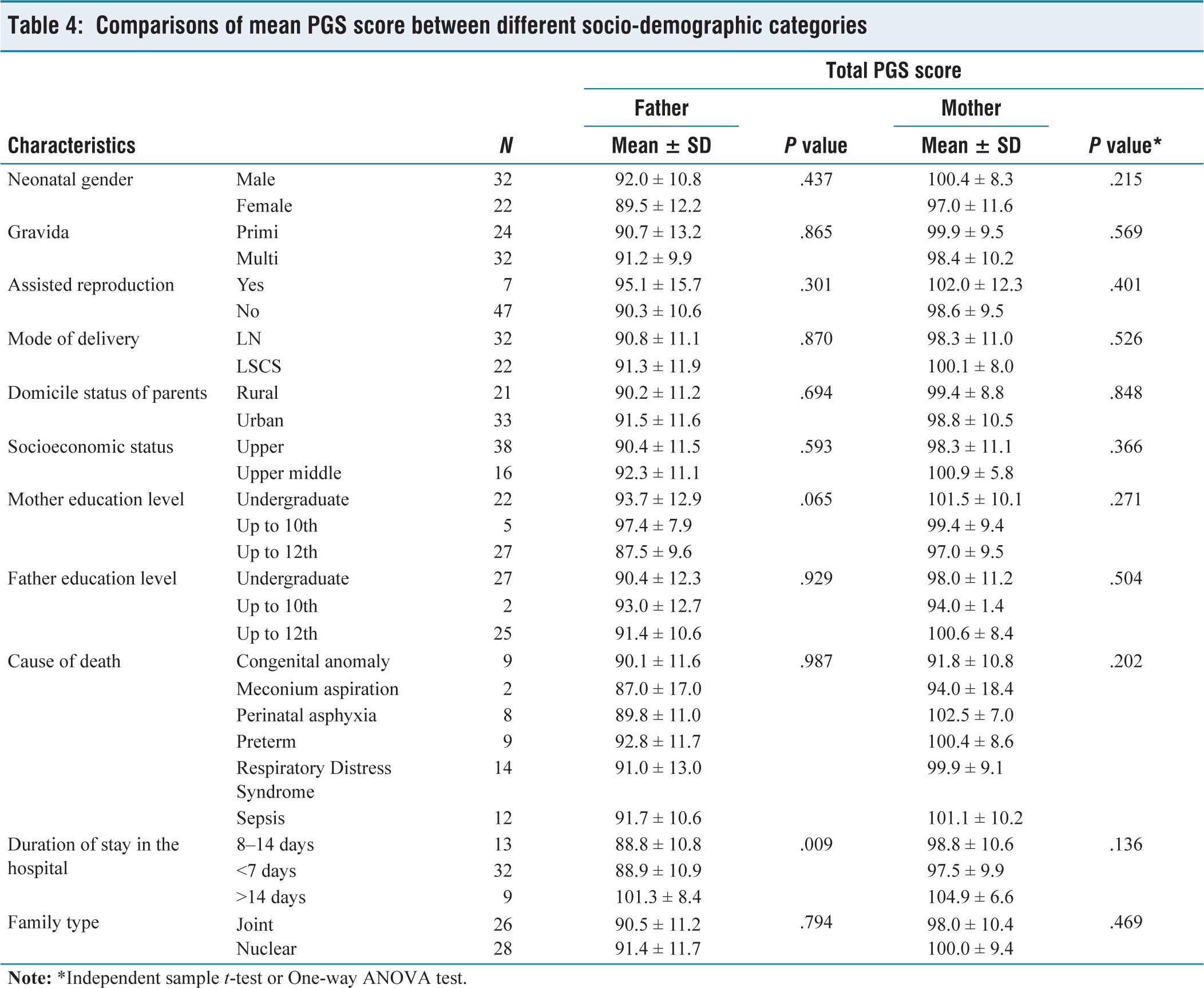
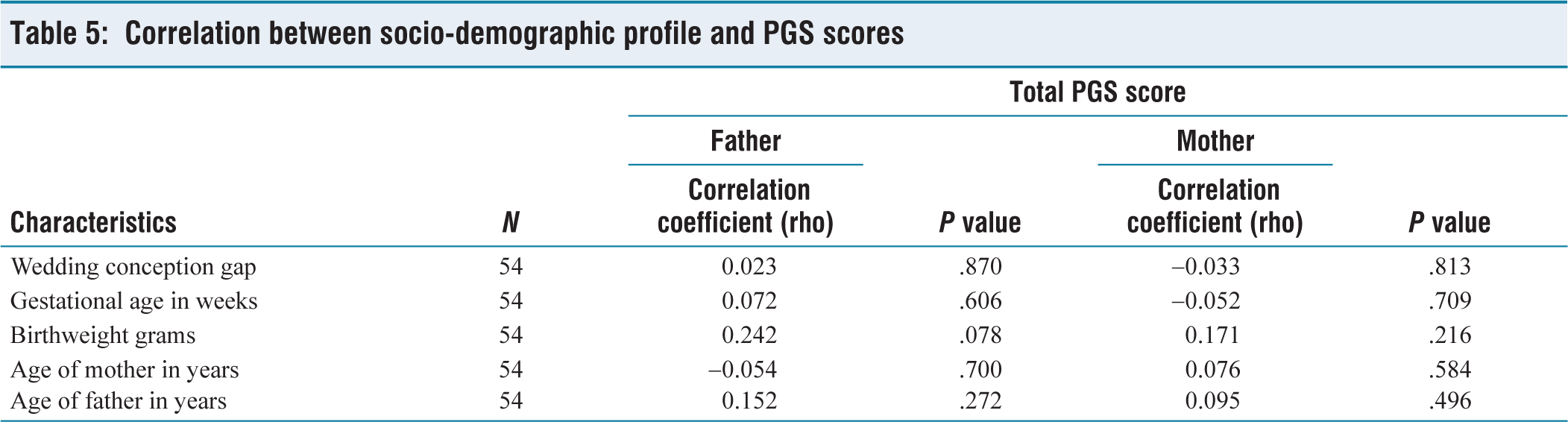
The PGS total scores and subscale scores for the fathers and mothers are shown in Table 3. Significantly higher number of mothers had a total score of 91 and above than the fathers (P = .0032). The mothers had significantly higher mean total and sub-scale scores than the fathers. On analysing the PGS scores across various neonatal factors and socio-demographic factors of the parents, no significant difference was observed between them [Tables 4 and 5]. The grief experienced was universal.
PGS scores distribution
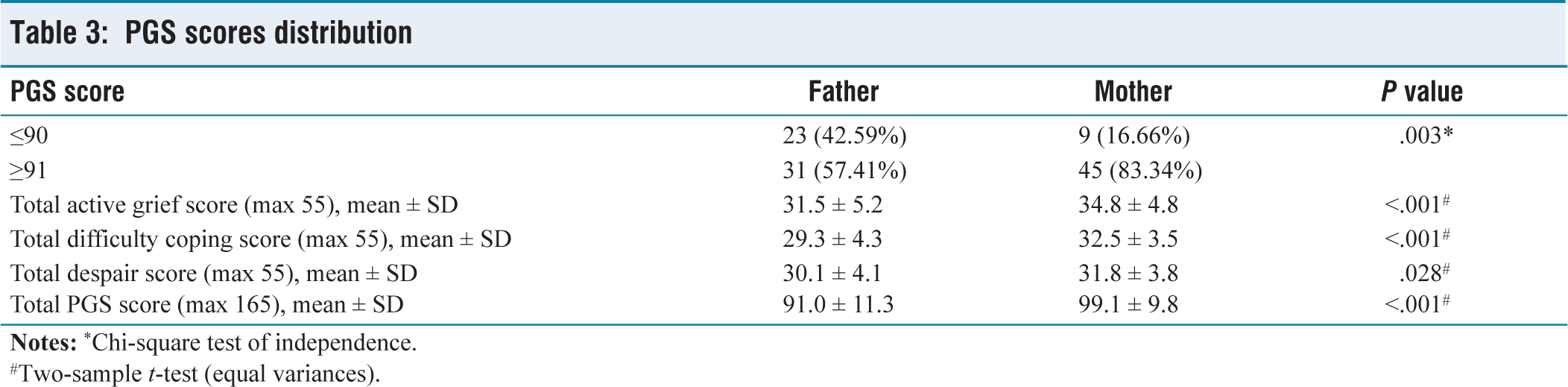
#Two-sample t-test (equal variances).
Comparisons of mean PGS score between different socio-demographic categories
Correlation between socio-demographic profile and PGS scores
Qualitative Analysis
The qualitative analysis of the grief experienced by the parents was divided into three domains: active grief, despair, and difficulty coping. The parents were analysed by INI or FGD. All the mothers in this study experienced severe grief immediately after the death of their baby. They expressed anger, guilt, disbelief, severe pain, and helplessness. The initial expression of active grief is anger in most parents. Some parents’ anger was directed towards the Doctors, nurses, and the hospital. They expected some form of consolation or counselling from the hospital. A mother who is working as a data entry operator said,
When I felt the whole world had stopped on hearing my baby’s death, the hospital seemed to move on as if nothing had happened. It may be another day for the hospital, but for me, it was the end of the world, as this baby was born after a long period of waiting. No one consoled me, and none of my relatives were allowed inside the ward.
Many other parents also expressed similar experiences. Few mothers felt depressed (n = 7), and some of them felt they would be better if any treatment were provided. Many parents were haunted by the memories of their late neonate even after a month. A mother from a rural area said, Even now, I keep expecting to hear her voice in my dreams. I still do. I still wonder what I will do without her in my life. Some parents who were anticipating of poor outcome for the neonate experienced guilt. A 24-year-old father who lost his neonate due to congenital diaphragmatic hernia said,
Even though we had been informed about the baby’s defect during the scan, we held on to hope that everything would be fine. But now we feel that the consanguineous marriage was the cause for the death of the baby.
In some parents, the guilt was extreme, leading to suicidal thoughts. In IDI, one mother said that she attempted suicide and was saved by her husband.
On analysing the despair component in the IDIs, parents who had undergone ART had more despair than other parents (n = 7). The despair results from many years of treatment and the costs involved. A 31-year-old father said, We spent nearly a lakh for this pregnancy. We expected the baby to be fine & healthy. Losing him broke our hearts and left us emotionally drained while the financial strain made it even harder to heal. Few mothers (n = 4) doubted that they would again conceive or if the next one would also die of some illness. One mother said
the security personnel were very strict and did not allow my husband inside the ward. All the women had their babies with them in the ward. I was the only mother in the ward without a baby. It was very painful and I felt lonely
For analysing difficulty coping, both IDIs and FGDs were used. Most parents (n = 25) experienced difficulty facing their families and friends. Only a few parents felt that the family and friends were supportive and understanding. A mother hailing from a rural area, who lost her neonate to congenital heart disease, said,
He was my third child, my precious son. He was sick. I knew it. The doctor told us. I begged God to let him stay. But still, I lost him. My mother-in-law blamed me for giving birth to a sick son. What hurt the most was not his death but being told it was my fault for repetitive deaths.
Many of the parents feared for their future (n = 9). They feared facing society, relatives, and friends. They resorted to blaming themselves and increasing their feeling of guilt. Most parents appreciated the support given by the hospital in transporting the dead neonate in a mortuary van (n = 42). Few mothers said that the relationship dynamics changed after the death of the neonate. One mother who lost her neonate to perinatal hypoxia said, My husband is in great stress, and he is not speaking to me like before. He thinks I have not taken adequate care during pregnancy. We fight a lot now. I don’t know when this will end. Since the questions were open-ended in the qualitative analysis, many parents volunteered suggestions. Most of the suggestions were for improvement in the counselling sessions. A father who lost his neonate due to congenital heart disease said,
Doctors knew that my child would not survive. But they did not openly admit that. We were in great distress for the past 7 days. If we had been told about the poor outcome, we would have been mentally prepared.
Most parents expected some words of consolation from the Doctors and nurses once the neonatal death was declared.
Discussion
The neonatal care in India is witnessing great improvements in recent years.[2] The neonatal mortality rate is decreasing year after year. But the grief experienced by the parents after neonatal death is less studied in India.[3,9] Only a few studies are available in India that describe the grief they experienced. Most of these studies are not done at public hospitals. This study explores the grief experienced by the parents in a public hospital.
The mean PGS score of fathers and mothers in this study was 91.0 ± 11.3 and 99.1 ± 9.8, respectively. Das MK et al. described the grief experienced by the parents after child death and stillbirths qualitatively in the year 2020 in North India.[11] They reported a median PGS score of 107 after stillbirths and 86 after neonatal deaths. The median PGS score after neonatal death was lower in that study than in the present study. The difference may be because the present study analysed the grief after 1 to 2 months of neonatal death, whereas that study analysed the grief after 6–9 months.
In a study by Marawah et al. from North India, mothers experienced higher levels of grief, remorse, anxiety, and depression.[17] The mothers also experienced stigmatisation, spousal abuse, and rejection by their families. But none of these were found in the present study. This may be due to the better educational and socio-economic class of the participants in the present study. In a study from Ghana, the mothers did not experience any disturbance in the relationship with their husbands, and their coping strategies were similar to the parents in the present study.[18] In a study from the Netherlands, in about 30% of mothers, grief persisted even after 6 years of the neonatal death.[18] This study reiterates the need for continuous support for the bereaved parents. In a study by Harper et al. the parents asserted financial implications as a major difficulty in coping, similar to the present study.[19] The mothers in this study experienced more grief than the fathers. In studies from Europe and North America, similar experiences were reported.[20–22] The fathers react differently to grief than the mothers. A study by Roberts et al. among poor rural women in central India observed significantly higher perinatal grief among the rural women when compared to urban women.[23] However, such a difference in grief scores between rural and urban parents was not observed in the present study.
Most of the mothers expressed disappointment about the absence of any consolation from the Doctors and nurses immediately after the declaration of death in the present study. In India, the public hospitals are more focused on providing clinical services to the patients. Their psychological consequences are often ignored in a busy hospital setting. As the prevalence of severe grief is more than 83% in mothers in the present study, the need for structured bereavement care and grief counselling services becomes imperative. Many studies in developed countries have identified the lack of knowledge among health care personnel on handling bereaved parents.[24] Education and training are important for both the parents and health care personnel to overcome the grief.[25] Many hospitals in developed countries have a structured bereavement program to support these parents.[25–28] However, such structured programs are not in place in developing countries. Grief counselling should also become a part of public health care in developing countries also, and all healthcare providers should be trained in it. This study had a few limitations. Long-term follow-up of the parents was not done to analyse the persistent grief, and the study was done in a single centre.
Conclusion
In this study, a significantly higher number of mothers had severe grief than the fathers. The grief was universal as it was found to transcend various socio-demographic profiles. The parents felt the absence of bereavement care practices in the hospital was disappointing. Some parents had difficulty coping with the grief socially. In developing countries like India, neonatal care is essentially clinical, and the care is mostly directed towards the treatment of the medical condition alone, ignoring the psychological impacts that it will have on the parents. With improving neonatal care in India, the bereavement care practices should become a standard of care, and the long-term mental health of the parents after their neonatal loss should be ensured.
Footnotes
Acknowledgements
The authors would like to thank all the participants and the nurses working in both centres.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Obtained.
Informed consent
Obtained.
Credit author statement
Dr M. Danishraja, Dr. M.S. Balamurugan, Dr P. Kumar, and Dr V. Anurekha were involved in the acquisition, analysis, and interpretation of data.
Dr V. Anurekha, Dr S. Gobinathan, and Dr K.S. Kumaravel drafted the article and revised it critically for important intellectual content.
All the authors have participated sufficiently in the work and take public responsibility for appropriate portions of the content.
All the authors read and approved the final version before submission.
Data availability
The data that support the findings of this study are available on request from the corresponding author.
Use of artificial intelligence
Not used in this study.