
Abstract
Background:
Semi-structured programmes are available to promote knowledge of lung ultrasound (LUS) among intensivists, and in many neonatal units, LUS is increasingly utilised in the diagnosis of Respiratory Distress Syndrome (RDS).
Aims and Objectives:
This study seeks to qualitatively evaluate the LUS performed by sonographers of varying experience levels, while quantitatively assessing the agreement in LUS scores between an expert and them in Neonates with RDS.
Methods:
This is a single-centre, mixed-methods study with 10 participants who conducted LUS scans on 61 neonates less than 34 weeks of gestation diagnosed with RDS. The LUS scans were qualitatively and quantitatively assessed by a non-participant expert using a scoring system that included six zones and a total score.
Results:
The mean birth weight was 1.3 ± 0.2 kg. The mean gestational age was 31.1 ± 1.6 weeks. Qualitative analysis revealed that all participants demonstrated adequate image quality in LUS imaging. The ICC between the expert and other sonographers for the total scores ranged from 0.98 to 0.99, indicating excellent reliability. The kappa values for zone-wise interrater agreement demonstrated almost perfect agreement (0.81 to 1) in 60% of measurements and substantial interrater agreement (0.61 to 0.8) in 36.66% of measurements.
Conclusion:
This study has demonstrated adequate quality of LUS scans conducted by sonographers of varying experience levels. This study has demonstrated that neonatal LUS is easy to learn, simple to practice, and consistent with sonographers of varying experience levels.
Introduction
Diverse aetiologies can cause respiratory distress in neonates, and the most common cause is Respiratory Distress Syndrome (RDS).[1] RDS warrants rapid diagnosis and treatment. RDS has been diagnosed based on the clinical findings and conventional X-ray of the neonatal chest so far.[2] In many neonatal care units, lung ultrasound (LUS) is increasingly employed in the diagnosis of RDS.[3] The advantages of LUS are rapid diagnosis and reduced exposure to irradiation. Point of Care Ultrasound (POCUS), including LUS and other sonograms, is increasingly used by intensivists in paediatric and neonatal care.[4]
The thin chest wall of the neonate makes it easy to perform the LUS scan. The diagnosis of RDS is made by the presence of B-lines with or without consolidations.[5] Many scoring systems are available to quantitatively diagnose RDS.[6] These scores are not only used in the diagnosis but are also used in the decision-making regarding the need for surfactant/ventilation and to prognosticate the disease.[7]
There are many semi-structured programmes to propagate the knowledge of LUS that are being offered to the intensivists.[8] These programmes provide a brief hands-on training to the trainees, and the trainees continue to learn LUS in their clinical practice and become experts in it. A significant limitation in the further propagation of LUS use in everyday clinical practice is ensuring its reproducibility and consistency between sonographers of varying experience levels. So far, all published studies have utilised an expert sonographer in their study to perform the scoring, the results of which cannot be generalised to all sonographers, who have varying levels of experience.[7,9] There are limited studies that have evaluated the consistency between sonographers of varying experience levels, and this study aims to address this gap.[10,11]
Aims and Objectives
This study aims to qualitatively evaluate the LUS performed by sonographers of varying experience levels and quantitatively evaluate the agreement in LUS scores between them in neonates with RDS.
Methods
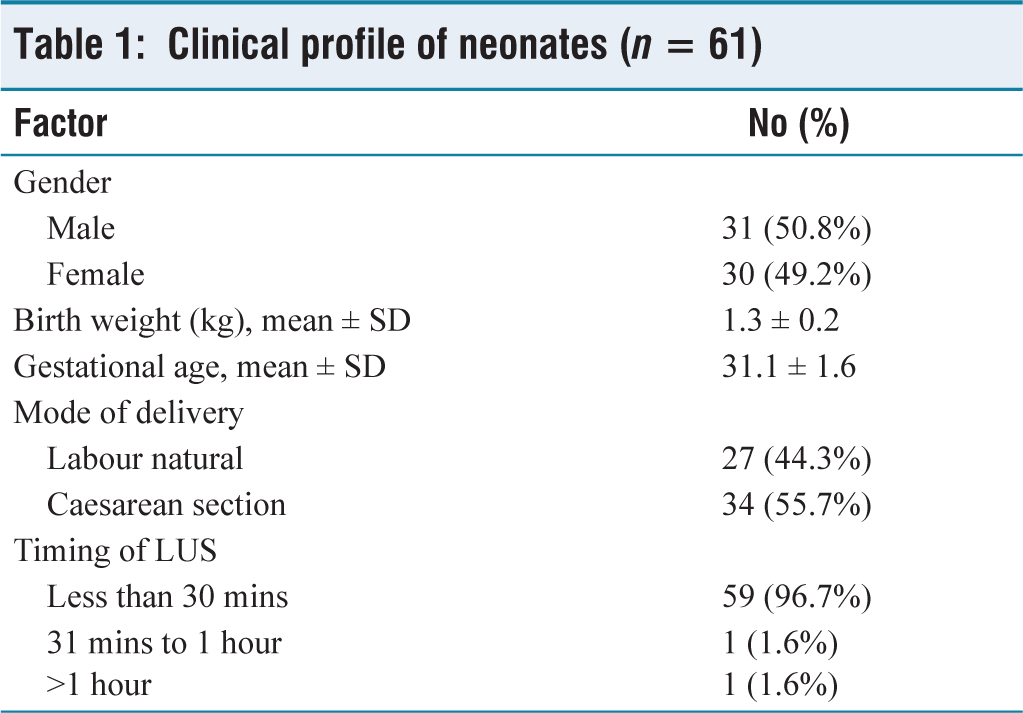
This is a single-centre, mixed-methods study conducted in a neonatal care unit of an urban tertiary care hospital from February to September 2025. The study hospital has a policy of providing formal training in LUS to all faculty and residents upon recruitment. The neonates less than 34 weeks of gestation diagnosed with RDS were included. Neonates with other causes of respiratory distress and neonates with RDS for whom a scan could not be done were excluded. A total of 10 sonographers with varying levels of experience were recruited [Table 1]. A sonographer, with more than 6 years of experience in LUS and a master trainer, who was blinded to the clinical picture, was designated as a reference expert for this study. He assessed LUS both qualitatively and quantitatively. The sonographers with less than 1 year of experience were excluded. Baseline clinical data were collected. RDS was diagnosed based on the history, clinical findings, radiological features, and LUS findings.
Clinical profile of neonates (n = 61)
The Philips Ultrasound system (Model: 3300G) with a high-frequency linear probe (12MHz) was used in the study. Neonates were stabilised, and scans were performed within 1 hour of birth, before or after surfactant administration. The scoring system proposed by Brat et al. was used in this study.[12] The LUS was performed by dividing the lung fields into three fields on either side, and a score from 0 to 3 was assigned for the presence of A or B-lines or consolidations. For each lung field, a point score from 0 to 3 was given (total score ranging from 0 to 18). The LUS scoring was done as follows: 0: A-pattern (A-lines only), 1: B-pattern (3 well-spaced B-lines), 2: Severe B-pattern (coalescent and crowded B-lines with or without subpleural consolidations), and 3: Extensive consolidations. The A-lines denote pleural reflection, and the B-lines denote fluid filling the interstitium. Each of the 10 participants was required to perform 6 to 7 LUS examinations during the study period. They were instructed to report the findings and save the videos on the hard disk of the scan system. All the recorded videos were pooled, and all 10 participants and the expert were instructed to score all the recorded videos. For qualitative analysis, the expert conducted content analysis of the reports submitted by the participants and the archived videos. The parameters evaluated included the accurate visualisation of the lung field, identification and reporting of A and B-lines, detection of consolidations, and precise scoring. Consent was obtained from the parents. Institutional human ethics committee approval was obtained.
Sample Size
The sample size for quantitative analysis was determined based on the study by Puskarz et al., which reported an Intraclass Correlation Coefficient (ICC) of 0.93 between expert and non-expert sonographers.[13] Expecting a similar ICC, with a 95% confidence interval (CI) and an absolute precision of ±5%, the required sample size was 60.
Statistical Analysis
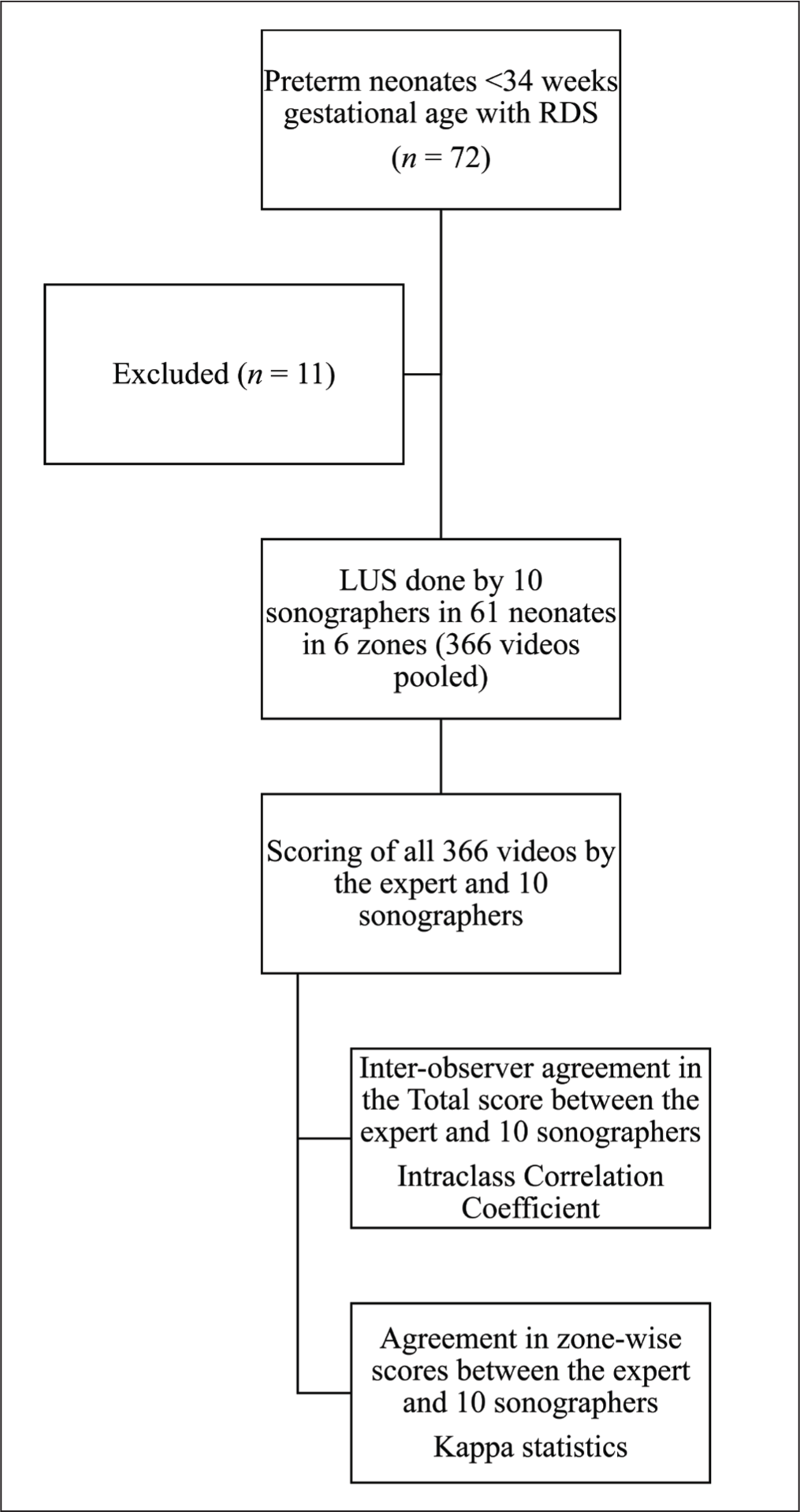
Data were analysed using R software, Version 4.3.1. All categorical data were presented using frequency and percentages, and all continuous data were described using mean and standard deviation. Inter-observer agreement between the expert and each sonographer for the total LUS score was assessed using the ICC derived from a two-way random-effects model (absolute-agreement type), with 95% CI. The ICC was interpreted as follows: <0.5 poor, 0.5–0.75 moderate, 0.75–0.9 good, and >0.9 excellent. Fleiss’ kappa was used to assess the agreement in zone-wise scores between the expert and each sonographer. Kappa values are interpreted as follows: 1, perfect agreement; 0.81–0.99, almost perfect; 0.61–0.80, substantial agreement; 0.41–0.60, moderate agreement; 0.21–0.40, fair agreement; and 0.00–0.20, poor agreement. The research process is summarised in Figure 1.
Flow diagram of research process
Results
The clinical profile of the neonates in the study group is depicted in Table 1. In the study group, 50.8% of the neonates were males. The mean birth weight was 1.3 ± 0.2 kg. The mean gestational age was 31.1 ± 1.6 weeks. About 55.7% of neonates were born by Caesarean section, and LUS was performed within 30 minutes in 59 neonates.
Qualitative Analysis
The expert sonographer, who was blinded to the clinical picture of the neonates and sonographers in the study group, performed content analysis of all LUS scan reports and the saved videos. The parameters analysed were the correct visualisation of the lung field, the ability to distinguish different zones, the identification and documentation of A and B-lines, the identification of consolidations, if any, and assigning correct scores. All the participants have documented and saved the important LUS findings, such as A-lines, B-lines, and consolidations, if present. The correct visualisation of the lung field and assignment of scores were also perceived as adequate by the expert sonographer. Overall, the expert was fully satisfied with the quality of the LUS scans done by all sonographers. Since he was blinded to the sonographers, he could not appreciate any difference in the quality of scans done among the sonographers in the study group.
Quantitative Analysis
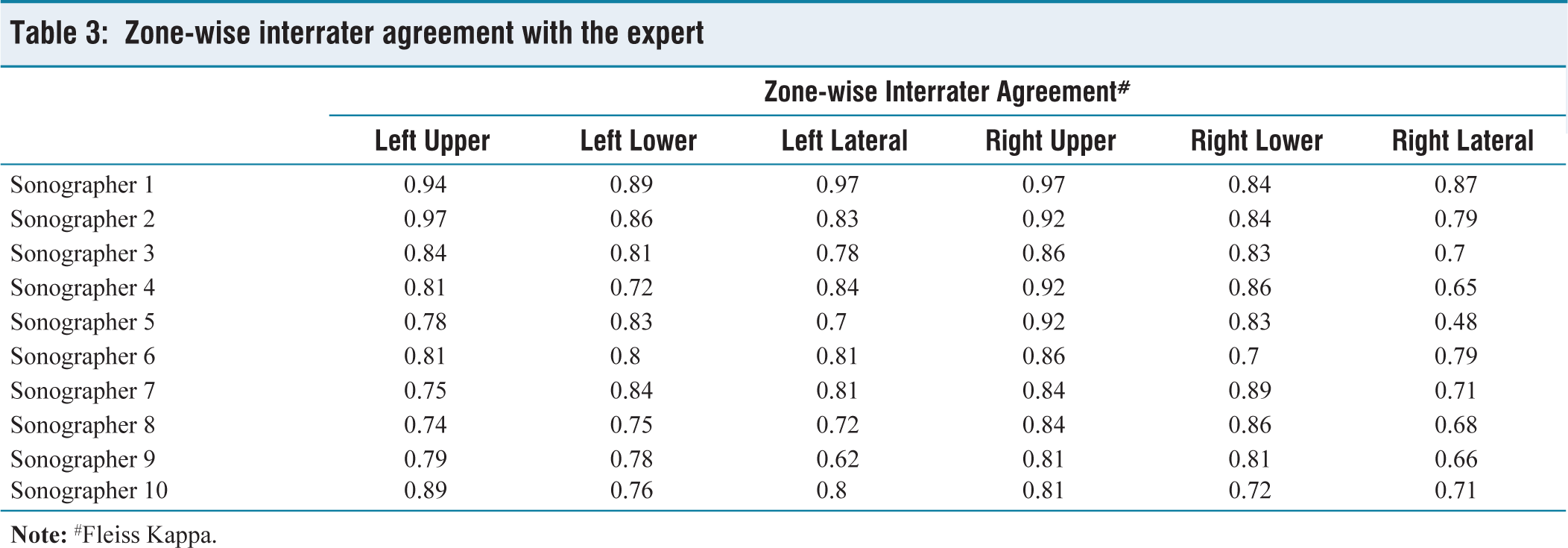
The ICC between the expert and other sonographers for the total scores ranged from 0.98 to 0.99, indicating excellent reliability [Table 2]. The zone-wise interrater agreement between the expert and other sonographers is depicted in Table 3. The kappa values for zone-wise interrater agreement demonstrated almost perfect agreement (0.81 to 1) in 60% of measurements and substantial interrater agreement (0.61 to 0.8) in 36.66% of measurements. The kappa value of the right lateral zone by the fifth sonographer was the least (0.48) observed, indicating moderate agreement.
Profile of sonographers and their intraclass correlation coefficient with the expert

Zone-wise interrater agreement with the expert
Discussion
In this single-centre study, qualitative analysis of the LUS scans was done. So far, only quantitative studies of interrater agreement in neonatal LUS have been available.[13,14] These studies used LUS images or videos done by experts for scoring by inexperienced sonographers. The quality of the LUS images and videos captured by experts cannot be extrapolated to inexperienced sonographers. To overcome this bias, in this study, we analysed the quality of LUS scans done by sonographers of varying experience levels, and no difference in the quality of scans performed was observed between them.
In the quantitative analysis, we have demonstrated that formal training and continuous practice of neonatal LUS enable all paediatricians to easily perform neonatal LUS, and their scores are comparable to experts having more than 3 years of experience. The ICC demonstrated by experts and other sonographers in this study was between 0.98 and 0.99, respectively. In a study by Puskarz-Gasowska et al., the ICC between experienced and inexperienced sonographers demonstrated excellent reliability on total LUS scores.[13] They have shown the outstanding reproducibility of LUS scores irrespective of the level of experience of the sonographer. A study by Giocoma Brusa et al. demonstrated significant inter-observer agreement in the diagnosis of Transient Tachypnea of Newborn.[14] A study by Victor Sartorius et al. showed that increasing the frequency of the scan probe increased the scores given in LUS.[10] In the present study, we used a higher frequency probe. On analysing the zone-specific kappa, 60% of all measurements had substantial agreement. However, the left lower zone had a lower kappa value among a few sonographers. This is due to the interference of the cardiac shadow in the interpretation, which has been reported in many studies.[15,16] Though the kappa values were lower in some zones, they had no bearing on the total scores. Given the nature of the disease, RDS being a homogenous disease involving the entire lungs uniformly, these minor zone-level variations will not affect the total score significantly.[17]
This study has demonstrated that the neonatal LUS is easy to learn, simple to practice, and easily reproducible. This is in contrast to other POCUS imaging procedures, which require more advanced and more structured training to ensure reproducibility, which makes these results not generalised to other POCUS imaging procedures.[18,19] The significant challenge in the neonatal care units in day-to-day practice is the validation of the scores assigned by the operators of varying levels of experience.[19] The process of validation should be continuous, and a similar exercise should be done periodically.[20,21] The limitation of this study is that it is a single-centre study.
Conclusion
This study has demonstrated adequate quality of the LUS scans performed by sonographers with varying experience levels. Significant reliability, diagnostic accuracy, and interrater agreement of LUS scores were observed between them and an expert. The ease of learning with formal training, easy reproducibility of the LUS scores, and good diagnostic accuracy make neonatal LUS an essential bedside tool for the rapid diagnosis of RDS.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Acknowledgements
The authors would like to thank all the participants and the nurses working in the centre.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Obtained (No: 2025/3273).
Informed consent
Obtained.
Credit author statement
Dr M. Balaji, Dr T. Palanivelraja, Dr. R.Aiswarya and Dr V. Anurekha were involved in the acquisition, analysis, and interpretation of data.
Dr V. Anurekha, Dr S. Gobinathan, and Dr K. S. Kumaravel drafted the article and revised it critically for important intellectual content.
All the authors have participated sufficiently in the work and take public responsibility for appropriate portions of the content.
All the authors read and approved the final version before submission.
Data availability
The data that support the findings of this study are available on request from the corresponding author.
Use of artificial intelligence
Not used.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.