
Abstract
Background
Headache is an extremely common symptom of the general outpatient department and also the headache clinic, with prevalence of 48.9% in the general population. None has ever experienced headache in life time. Headache is seen in 1 patient out of 10 general practitioner (GP) consultations, 1 referral out of 3 is headache in neurology OPD, and 1 in 5 of all emergency medical admissions. Of all headaches, around 98% constitute primary headache: migraine without aura, tension headache, and cluster headache. With advancement in various drug modalities, certain headache forms respond less well to the regular approved medications, and some headaches are complicated by the analgesic itself. Steroids have been tried in many subtypes of headache, especially in primary forms of headache with dysautonomia, headache with trigeminal pathway activation and disinhibition, and in certain medication-culprit headaches. This subgroup of headaches is almost a challenge in an emergency for the headache expert as well. So, we need to assess the role of steroids in less well-responsive headaches.
Summary
Current reviewed evidence on the role of steroids in primary headache suggests that steroids have a role in status migrainosus and medication overuse headache when used in the mentioned and monitored manner. Consideration and further exploration of its role in other primary headaches may reveal insight into steroid efficacy as a treatment modality in various subtypes of headache.
Key message
Steroids, when used cautiously in specifically selected primary headaches under supervision, proved miraculous where other modalities failed.
Introduction
Headache is among the most frequently reported neurological complaints in the world and affects almost 50% of women in the general population during their whole lifetime. 1 According to a 2016 study, about 3 billion people have headache; of those, around 1.89 billion have tension headache (highest), and around 1.04 billion have the migraine worldwide. 2 It affects patients’ most productive period of life, causing significant disability and declining quality of living. 3
With all the abortive and preventive medications we use, the efficacy response rates vary from 40% to 70%, according to most studies. Mistreatment or undertreatment of headache disorders leading to recurrent emergency visits takes a toll on the healthcare facilities of a country, along with the economic burden that is caused by the loss of productivity due to headache disorders. Steroids have been studied as a therapy that might decrease the frequency of such recurrences of primary headache (i.e., migraine). These are supposed to prevent neurogenic inflammation. This review discusses the role and status of steroids in headache disorders to delineate their future role.
Rationale of Using Steroids in Migraine
Headache affects all races, all ages, and all socioeconomic clasess. Migraine is the most common type of primary headache and is a malfunctioning sensory phenomenon caused by painful stimuli. Pain occurs peripherally due to trigemino-neurocervical region abnormal excitation at primary level afferents, or it occurs at central level as a result of abnormal modulation at second-order neurons.4–7 Neuropeptides modulate the regulation of cascade inflammation, vasodilation of arterioles, and smooth muscle changes. Intervening the treatment goal in migraine is still a matter of concern with prevailing multimodalities because almost 75% of patients have functional disability affecting severely the quality of life and work absentees, and around 50% require social support. 9 Corticosteroids, the main mediators of stress, secrete in response to unfavorable stimuli resulting in the activation of physiological cascade and behavioral homeostatic mechanisms. Corticosteroids can readily pass blood-brain barrier (BBB) because of their lipophilicity and small size (300 Da) and because they participate in a varied physiological and behavioral phenomena and also take part in their own secretion. 8 Corticosteroids have proven useful for pain relief in other varied neurological conditions; pain medication is recommended in the pain ladder of the World Health Organization (WHO) for moderate-to-severe pain-causing diseases. 10 Corticosteroids inhibit synthesis, which in turn decreases inflammation and reduces permeability of the vasculature, causing edema. Receptors related to steroids are found in the peripheral and central nervous systems and are causative for development, differentiation of growth, and neuronal plasticity. 11 Administering corticosteroids exogenously suppresses the stress response and flurry of inflammation from the hypothalamic-pituitary axis and thus prevents the inflammatory cascade. Corticosteroids extend their suppression of neurological inflammation and reduce pain by modulating neuroplasticity. 12
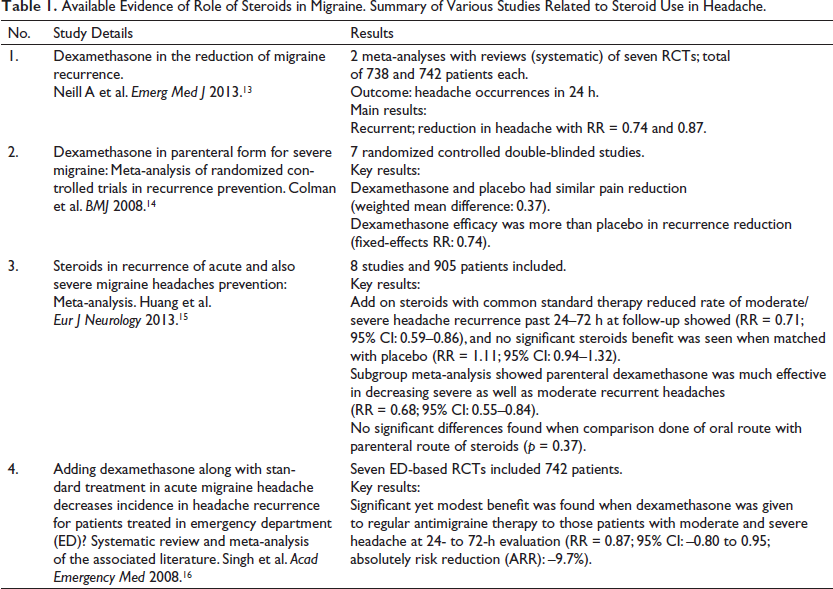
The largest systematic review to date on corticosteroids in migraine attack management included 25 studies (n = 3989; 37.5 years was the median age; interquartile period range, or IQ range, 35–41 years; male to female ratio 1:4.23; IQR 1:2.1–6.14; and 52% ED-based, 56% of the randomized-controlled) and 4 systematic analyses (Table 1). Nineteen studies (76%) showed favoring benefits of corticosteroid in outcome benefits; non-inferior outcomes with corticosteroids were shown in six (24%) studies. The median absolute reduction of risk was around 30% (range varied from 6%–48.2%), 11% (6%–48.6%) for 24 h, and 72 h of recurrence of headache. Parenteral dexamethasone was found to be the most commonly administered steroid (56%) at a median single dose of 10 mg (range being 4–24 mg). Adverse effects were also easily tolerable. Higher disability with status migrainosus, incomplete relief in pain, and history of previous headache recurrence predicted outcome favorability. 17 Latev et al. failed to demonstrate any benefit of long-acting depot corticosteroids (160 mg methylprednisolone acetate IM) over dexamethasone (10 mg IM) in migraine patients with moderate and severe intensity who presented to the emergency department (ED) in their randomized, blinded clinical trial. 18 Various randomized trials and meta-analyses of data concluded the benefit of steroids in the prevention of the recurrence of primary headaches. Dexamethasone in a single dose prevents recurrence in about 10% of patients with higher doses, and the effect persists for more than 3 days. It has a benign side effect profile with better tolerability. Steroids can be safely used as abortive therapy for preventing the recurrences of migraine. Though steroids used to be restricted for primary headaches because of their side effects and immunosuppressive profile, making people more vulnerable to infections.
Available Evidence of Role of Steroids in Migraine. Summary of Various Studies Related to Steroid Use in Headache.
Cluster Headache
Episodic cluster headache treatment comprises abortive treatment (e.g., high-rate flow oxygen, effective triptans, and/or intranasal route lidocaine) and preventive forms of medication (e.g., verapamil/lithium) that decrease the number of attacks with successful termination of the ongoing episode. The preventive drug of choice is verapamil. Due to the delayed action time of verapamil (10–14 days) with slower titration, there is a need for short-term preventive medication. Corticosteroids have been used in this indication for the last four decades, but the evidence behind this came from observational studies and one small randomized controlled trial. 19
Corticosteroids use as the transitional therapeutic option in managing (cluster headache) as a sub-occipital injection for GON block has been established by a few placebo-controlled RCTs.20, 21
According to this single-center retrospective comparative study (n = 140), 22 81 (57.9%) patients received oral steroids and 59 (42.1%) received GON block as a short-term prophylactic therapy for cluster-type headache (also CH). Of the 40 headache patients with treatment responses, 24 patients received one type as a transitional therapy, compared to 16 patients who received both therapies. Most respond to oral steroids when compared with GON injections; the partial response was rated as 82.7% in contrast to 64.4%, and few had a full response (50.6% in contrast 35.6%). The results lead the authors to conclude that the majority of patients with cluster headaches responded both to prednisone and to GON injections, with higher responders to oral steroids. Recently, Mark Obermann and colleagues 23 provided strong evidence for favoring the use of oral steroids as a transit alternative. Around 116 patients with episodic type of cluster headaches who had acute bouts were randomly distributed in blinded fashion to receive 100 mg of the oral route of prednisone for a 5-day period and then taper to 20 mg every 3 days (i.e., total of 1100 mg over 17 days; n = 53), or placebo (n = 56). Steroids were used as an additional treatment for the oral type of verapamil. Participants in the prednisone group had a mean of 7.1 (SD 6.5) number of attacks within the first week compared with 9.5 (6.0) attacks in the placebo group (difference –2.4 attacks, 95% CI –4.8 to –0.03; p = 0.002). The benefits of using prednisone were evident for the number of events during the initial 28 days, the number of days with attacks during the first period week, the rate of patients who achieved complete cessation of events after the initial 7 days, and the 50% responder rate (RR) at day 7 and at day 28 (secondary line endpoints). One prospective observational study showed the use of a steroid in the form of 10 mg of triamcinolone mixed in 1 mL of sodium chloride and 1 mL of bupivacaine in a concentration of 0.5% for blocking both the greater as well as other lesser occipital nerves and observed that more than 80% of patients were complete or at least partially responsive. A study in 83 chronic cluster headache patients showed steroid effects for a median 21-day duration benefit when used as a single injection in the greater occipital nerve (GON). 24
Medication Overuse Headache
Treatment of medication overuse headache (MOH) involves withdrawal of the causative medicine, preventive therapy, and rescue therapy for the withdrawal symptoms of headache. Among these, withdrawal of causation is the best measure for MOH. The role of the corticosteroids in relieving MOH comes from treating the withdrawal headache. The rationale behind using corticosteroids in the treatment of MOH came from studies that used a combination drug therapy (steroids with TCA in one study and steroid benzodiazepine and metoclopramide in the other) and demonstrated a significant decrease in the severity and intensity of headaches as well as analgesic usage.25, 26 In a Brazilian study (n = 400) aimed at assessing the effect of using a short course of prednisone in orally administered form as detoxification for patients with chronic headaches from overused medication, 85% of the patients had relief in frequency, and none presented with severe headache during the first 6 days. Over the next 10 days, 46% of patients had minimum of two headache-free days, and 58% had less severe headache. A marked relief in headache numbers with a mean as 0.83 and P < .001 was noted after 30 days. 27 One double-blind RCT using a 6-day course of oral steroids for the treatment of withdrawal headache in MOH failed to demonstrate any statistically or clinically significant benefit. 28 In their small proof-of-concept double-blinded placebo-controlled trial (n = 20), Pageler et al. 29 demonstrated that total hours of intense headache in first the 72 and 120 h were significantly less in the prednisone-taking patient group. The EFNS headache panel mentioned in their guideline to treat MOH that corticosteroids (60 mg prednisone/prednisolone) are much more effective in treating withdrawal symptoms. 30 Rabe et al. 31 conducted the first large, randomized, prospective, placebo-controlled, double-blinded study to investigate the utility of short-term steroids while treating MOH. Ninety-six consecutive patients with MOH were randomized to withdrawal treatment with 100 mg of prednisone or the placebo over a period of 5 days, and withdrawal features, including headache extremity and intake of any rescue therapy, were noted for 14 days after randomization. Although there was no difference noted between the two studied groups regarding the hours of moderate and/severe variety of headache during the initial 3 and then 5, at 14 days of withdrawal, the prednisone-taking group opted to use a lesser amount of acute treatment analgesics during the initial 1–3 days. However, this disparity in medication intake did not present by day 5 or day 14. In a retrospective non-randomized study of bridging therapy using IV benzodiazepine and steroids (5 days of daily infusion of methylprednisolone and diazepam) in patients with MOH demonstrated that at the fifth day, 82% of patients remained headache symptom-free, and 48% of patients never took any painkillers during the 5-day treatment. After 3 months, the intervention arm showed a much greater reduction of both headache period days in terms of months (9.4 contrast 3.0) and drugs (19.7 contrast 6.5), a higher rate of patients having ≥50% reduction of monthly headaches (p = 0.019) and symptomatic of drug consumption (p = 0.000), than the control group. 32 Though subgroup difference in terms of related analgesic responsible for MOH is not yet specified. In another randomized, placebo-controlled, single-blinded pilot trial in MOH patients (n = 83) who were not responsive to prophylaxis of 3 months received withdrawal therapy on inpatient using methylprednisolone in 500 mg of intravenous (IV) or paracetamol in 4 g IV dose or placebo IV as bridging therapy. Authors found methylprednisolone 500 mg of i.v. non superior over placebo. The two groups showed no difference in decreasing headache frequency, rescue medications amount during withdrawal period of 5 days, withdrawal symptoms but steroid proved to be slightly superior in reduction of rebound headache severity during the second day of the withdrawal. 33 In summary, steroids has shown promising results during detoxifying phase of drug-overuse headache in both oral or intravenous form. MOH or rebound type of headache patients shows less withdrawal symptoms and less detox headache when given both as inpatient or outpatient treatment along with topiramate as the best in managing prophylaxis phase of MOH. Corticosteroids as short course of oral prednisolone eased the process of detoxification in MOH and this result also obtained when used as a repeat intravenous therapy in an inpatient unit. 34
Steroids in Headache in Emergency Unit
Steroids have been used for severe migraine attacks in the emergency room as either oral or parenteral for treating sustained or status migrainosus, hemicrania continua, cluster headaches, and immunosuppressant-induced headaches in transplant patients. Short courses of rapid action-type oral corticosteroids (prednisone and/or dexamethasone) tapering relieves disabling pain in status migrainosus. Intravenous methylprednisolone in form of single dose or as outpatient unit infusion or as repetition of dosing in in hospital strategy unit can be used to break long-duration migraine attacks. There are case reports of HC attacks being successfully eliminated by multiple times infusion forms of methyl prednisolone. 35 Methylprednisolone is also quiet effective for subsiding acute onset attacks of paroxysmal type hemicrania (PH) and short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT) and short-lasting type unilateral neuralgiform headache attacks with cranial autonomic symptoms called (SUNA). Baraldi et al. concluded that methylprednisolone proves advantageous action in comparison to prednisone though in less degree. 36
Conclusion
With the emergence of newer treatments, both pharmacological and neuromodulatory, in the management of primary headaches, corticosteroids have played some role. These have been used for decades for pain management. Corticosteroids use for short periods in primary headaches where other treatments have failed shows evidence of breaking the pain cascade with improvement in pain scales by reducing the intensity of pain and in turn improving quality of life. There is also scope for RCTs in the fields of cluster-type headaches and MOH to establish the role of steroids in treatment. Moreover, steroids have a favorable side effect profile. In conclusion, resistant, disabling primary headaches, trigeminal cephalgias, and some medication overuse headaches become better with the use of a short steroid regime.
Footnotes
Acknowledgements
The authors acknowledge their technical staff and the patients with headaches who attend the neurology outpatient department, with whom we could experience steroid benefits.
Authors’ Contribution
Priyanka V. Kashyap—writing, editing, and information analysis.
Sounak Chabri—collecting information, writing, editing, and formatting the script.
Statement of Ethics
Not required.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.