
Abstract
We set out to review early descriptions of chronic migraine and medication-overuse headache. The International Headache Society (IHS) recently gave criteria for chronic migraine and medication-overuse headache. Chronic migraine was absent from the 1988 IHS criteria. Peters and Horton described ergotamine-overuse headache in 1951. In the 1980s it was more fully appreciated that overuse of other acute headache medications could increase headache frequency. We reviewed published English-language papers and book chapters. Willis (1672), Oppenheim (1900), Collier (1922), Balyeat (1933), and von Storch (1937) all described chronic migraine. Lennox (1934), O'Sullivan (1936), Silfverskiöld (1947), Graham (1955), Friedman (1955), and Lippman (1955) wrote about ergotamine-overuse headache. Graham (1955), Friedman (1955), Lippman (1955), and Horton and Peters (1963) outlined withdrawal protocols. Chronic migraine has been mentioned in the literature for centuries, while medication-overuse headache has been written about for decades. Graham, Friedman, and Lippman deserve credit for separately reporting the first ergotamine withdrawal programmes.
Keywords
Introduction
The second edition of the
2004 International Headache Society classification criteria for chronic migraine (1)

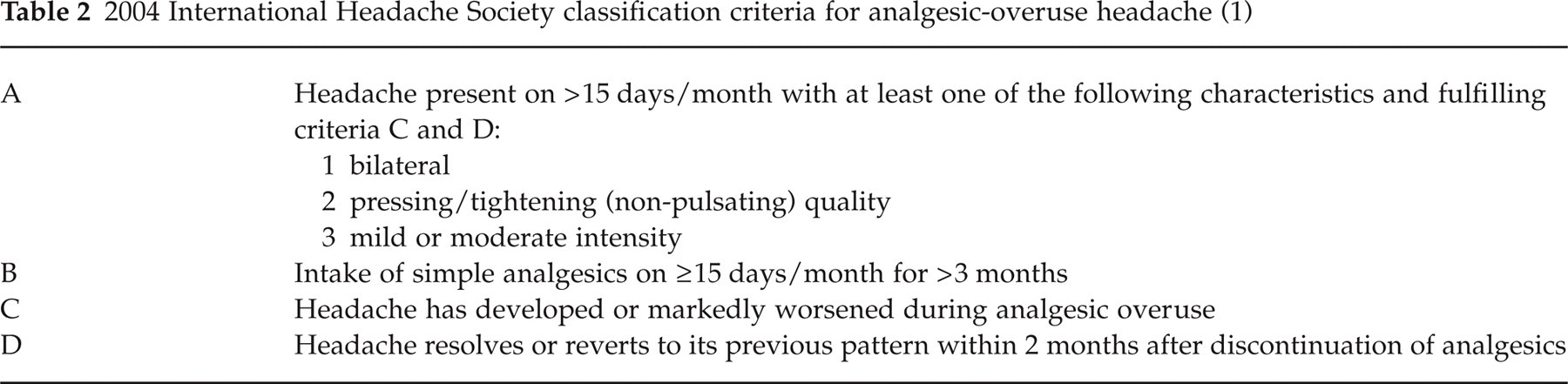
2004 International Headache Society classification criteria for analgesic-overuse headache (1)
Peters and Horton of the Mayo Clinic clearly described ergotamine-overuse headache in 1951 (3). According to Isler, medication-overuse headache had been misconstrued as restricted to ergotamine in English-language publications, but the paradoxical effect of compound analgesics in the perpetuation of headache had been amply discussed in Switzerland, in German, in the 1950s (4, 5). Swiss watch industry workers would spread their sandwiches with painkillers (4). Isler comments that a German-language paper by Kielholz in 1957 showed that abuse of over-the-counter analgesic compounds with phenacetin led to chronic headache in over 30% of female workers in some factories (5, 6). This chronic headache was explained as a phenacetin hangover headache, and ergotamine compounds (sometimes combined with barbiturates) were used to replace the phenacetin compounds (5). The ergotamine-containing compounds soon became a greater nuisance than the phenacetin compounds (5). These Swiss observations had no impact on the international literature, as they were not published in English and perhaps because the researchers focused on the renal disease caused by phenacetin (5).
In a 1975 German-language paper, Wörz et al. noted that the continuous use of mixed analgesics could lead to the development or deterioration of chronic headache (7). In 1980, Wörz discussed the paradoxical effects of analgesic drug mixtures in patients with chronic pain, the majority of whom had chronic persistent headache (8). Sixteen of 30 patients were dependent on ergotamine- or dihydroergotamine-containing compounds, but 14 of 30 were dependent on analgesic drug mixtures void of these substances (8). He (8) noted:
‘In the vicious circle of chronic pain and analgesic dependence, an important incentive for repeated drug intake is aggravation of the pain several hours or some days after drug cessation. In the long run, however, the discontinuation of analgesics is often accompanied by a substantial decrease of pain intensity or a change from persistent into intermittent pain. Therefore, withdrawal of analgesic drug mixtures is effective and appropriate therapy for some patients with chronic pain’ (p. 393S)
In 1982, Kudrow emphasized the paradoxical effects of frequent analgesic use in headache patients, noting that increased analgesic use was associated with increased headache frequency (9). In the same year, Isler noted that overuse of acute migraine medications could cause chronic migraine (10) and Mathew noted that excessive acute medication use influenced the transformation of episodic migraine into daily headache (11). In 1987, Mathew used the term ‘transformed migraine’ to describe this phenomenon (12). Lending support to the concept of medication-overuse headache was a double-blind study of abrupt caffeine cessation published in 1992 (13). In this study of subjects with low to moderate caffeine intake at baseline, the percentage of subjects who reported moderate or severe headache during the placebo period was significantly higher than the percentages during the baseline and caffeine periods (13). In 1994 Silberstein et al. gave formal criteria for transformed migraine (see Table 3) (14). In these criteria, transformed migraine could be associated with or without medication overuse. In 1994 Osborne et al. and Kaube et al. described medication-overuse headache secondary to sumatriptan (15, 16). In 1995 Silberstein et al. modified the diagnostic criteria for transformed migraine, publishing the new criteria in 1996 (see Table 4) (17). There were no definite headache phenotypic requirements in this classification as long as the patient had a history of episodic migraine. The headache had to occur > 15 days per month for > 1 month, and the average headache duration had to be greater than 4 h/day. A patient with daily or near-daily headache could fit the transformed migraine criteria in several ways. The patient could have migraine headache meeting 1988 IHS criteria < 15 days per month associated with phenotypic chronic tension-type headache (CTTH), or have migrainous headaches > 15 days per month meeting all 1988 IHS criteria aside from duration associated with phenotypic episodic tension-type headache, or have migrainous headaches alone meeting all 1988 IHS criteria aside from duration occurring > 15 days per month, or have phenotypic IHS CTTH as long as the patient had a past history of 1988 IHS migraine since the diagnosis of transformed migraine precluded the diagnosis of either episodic migraine or CTTH (17). Transformed migraine has since been called chronic migraine (18). Thus the current IHS criteria for chronic migraine are more restrictive than the Silberstein et al. criteria, in that the patient must have headache fulfilling criteria C (at least two of unilateral, pulsating, moderate or severe pain, aggravation by routine physical activity) and D (at least one of nausea and/or vomiting, photophobia and phonophobia) for IHS 1.1 migraine without aura on ≥ 15 days per month (1).
1994 Silberstein et al. criteria for transformed migraine (after 14)

‘1995’ Silberstein et al. criteria for transformed migraine (after 17)

This paper will review thoughts on chronic migraine and medication-overuse headache from years past published in the English-language literature. Information on chronic migraine and medication-overuse headache was extracted from all English-language texts on headache or migraine as well as from the migraine sections of all neurological texts in the Mayo Clinic History of Medicine Library and in the lead author's private collection.
Chronic migraine
Thomas Willis (1621–1675) (Fig. 1) was a 17th century English anatomist and physician who introduced the word ‘neurology’ and whose name is immortalized in the eponym for the circle of arteries at the base of the brain. Others have reviewed his immense contributions to neurology (19, 20).
Thomas Willis. Courtesy of the National Library of Medicine.
In 1672, Willis published
‘Some years since, I was sent for to visit a most noble Lady, for above 20 years sick with almost a continual Headach, at first intermitting. Growing well of a Feavour before she was 12 years old, she became obnoxious to pains in the Head, which were wont to arise, sometimes of their own accord, and more often upon every light occasion. This sickness being limited to no one place of the Head, troubled her sometimes on one side, sometimes on the other, and often thorow the whole compass of the Head. During the fit (which rarely ended under a day and a night's space, and often held for two, three, or four days) she was impatient of light, speaking, noise, or of any motion, sitting upright in her Bed, the Chamber made dark, she would talk to no body, nor take any sleep, or sustenance. At length about the declination of the fit, she was wont to lye down with a heavy and disturbed sleep, from which awaking she found herself better, and so by degrees grew well, and continued indifferently well till the time of the intermission. Formerly, the fits came not but occasionally, and seldom under 20 days of a month, but afterwards they came more often: and lately she was seldom free. Moreover, upon sundry occasions, or evident causes (such as the change of the Air, or the year, the great Aspects of the Sun and Moon, violent passions, and errors in diet) she was more cruelly tormented with them. But although this Distemper most grievously afflicting this noble Lady, above 20 years (when I saw her) having pitched its tents near the confines of the Brain, had so long besieged its regal tower, yet it had not taken it: for the sick Lady, being free from a Vertigo, swimming in the Head, Convulsive Distempers, and any Soporiferous symptom, found the chief faculties of her soul sound enough’ (p. 44)
Hermann Oppenheim (1858–1919) (Fig. 2) was the acknowledged leader of German clinical neurology during the late 19th and early 20th centuries. He was a favourite assistant of Carl Westphal at the University of Berlin, and was appointed Professor in 1893 (22). Oppenheim's name is eponymously associated with primary torsion dystonia (which he called dystonia musculorum deformans), and a pathological reflex (elicited by applying pressure to the tibia which results in an extensor plantar response in disease of the pyramidal tract). Seven German editions of his

Hermann Oppenheim.
In his 1900 neurology textbook (23), Oppenheim wrote:
‘There is a form of migraine which is characterized by the
James Collier (1870–1935) (Fig. 3) was ‘a [Queen Square] clinical neurologist of superlative ability’ (24). His contemporaries at Queen Square included Gordon Holmes and S. A. Kinnier Wilson (24). Collier, J. S. Risien Russell, and Frederick Batten were credited with the first serious description of subacute combined degeneration of the spinal cord (24, 25).
James Collier. Courtesy of the National Hospital for Neurology and Neurosurgery, Queen Square, London, UK.”UCLH NHS Trust.
In 1922 a new textbook of medicine was issued, edited by Dr Frederick Price. Collier and Dr W. J. Adie wrote the section on neurology, which was a ‘dazzling contribution based largely on personal experience’ (24). In the chapter on migraine, Collier commented that there were migraine cases ‘in which the headache lasts for weeks, or becomes continuous’ (26). He (26) also stated:
‘In some cases of long standing [migraine], the attacks become less severe towards middle life, and a persistent aggravating headache may develop between the attacks. When such a persistent headache is complained of alone, it is very important to inquire about preceding migraine, for the same treatment is applicable to the two conditions’ (p. 1504)
Theodore J. C. von Storch (1905–1965) (Fig. 4) received his MD from Johns Hopkins in 1931. He trained in neurology at Boston City Hospital. In subsequent years he worked at Harvard Medical School and Boston City Hospital, and at the Albany and Montefiore Hospitals in New York. He eventually became a Clinical Professor of Neurology at Columbia. He finished his career as a Lecturer in Neurology at the University of Miami. He was a member of the American Neurological Association.

Theodore J. C. von Storch. Reproduced from GP 1954; IX:140.
Dr von Storch (27) supported Collier's view on chronic migraine, noting in 1937 that
‘There are … exceptions to the invariable inclusion of recurrent headaches in the migraine syndrome. The first occurs when recurrent headaches have, over a period of time, gradually merged into a constant state of cephalgia of varying degree. In such a situation the history of previously recurrent headaches becomes essential’ (p. 247)
Ray M. Balyeat (1889–1961) (Fig. 5) received his MD from the University of Oklahoma in 1918. He eventually became an Associate Professor of Medicine at the University of Oklahoma. In 1925 he founded the Balyeat Hay Fever and Asthma Clinic in Oklahoma City, Oklahoma. He was the president of the American Association for the Study of Allergy in 1931.

Ray M. Balyeat. Reproduced from the cover of The Medical World 1938; 56(7).
In 1933 Balyeat published
‘In a few patients during the late thirties or early forties we have observed a change from the typical hemicrania to chronic headaches, less severe and usually generalized in character. As a rule these patients are never quite free from their headaches. However, they have periods of definite increase in severity which correspond largely to the attacks that they had been accustomed to having. The prodromata and visual aura are often less marked. Nausea may persist, but emesis is rare. About 5% of all our cases fall in this classification’ (p. 68)
He goes on to comment that ‘not unlike the treatment of the patient suffering from chronic asthma, the treatment of the migraine patient who has developed the chronic stage is much more difficult than the one who is entirely free from headaches between attacks’ (28).
Medication-overuse headache
William G. Lennox (1884–1960) (Fig. 6) was a Harvard neurologist well known for his contributions to epilepsy. His name along with Gastaut's denotes a syndrome of encephalopathy with atonic, tonic, and absence seizures (29). He was also interested in migraine, publishing a book on its association with epilepsy in 1941 (30). With Stanley Cobb and Harold Wolff he studied cerebral blood flow and the effect on pial vessels of variations in the oxygen and carbon dioxide content of the blood (31).

William G. Lennox. Reproduced from Mod Med 1951; 19:11.
In 1934 Lennox wrote an article on the use of ergotamine tartrate in migraine (32). He noted that ‘patients whose attacks are terminated when treatment is first instituted may later on fail, at times, to obtain relief, or else the interval between attacks may be shortened’ (32). Of the seven patients with frequent, incapacitating headaches who had almost uniform relief of individual attacks with ergotamine, four had more frequent attacks and three less frequent attacks after starting the treatment (32). Lennox (32) presented the following patient:
‘A housewife, aged 54, has had frequent incapacitating hemicrania with nausea and vomiting since childhood. Besides various medical treatments, she had submitted to removal of her gall bladder and of her cervical sympathetic nerves, without even temporary relief. Headaches which lasted two to three days recurred every week or 10 days. In addition, in recent years she has had almost daily moderate headaches for which she uses headache powders. Ergotamine tartrate has been used subcutaneously for 18 months. Each time it stops the headache, but on some occasions the pain has returned, and there has been a tendency for attacks to recur more frequently. She now takes 0.5 mg subcutaneously almost daily. Her suffering is greatly reduced, but she is till in the coils of this disease’ (p. 1063)
Lennox stated that ‘on the basis of this preliminary experience, it seems probable that patients with frequently recurring and very severe headache may not find permanent help in ergotamine tartrate’ (32). He did not mention tapering ergotamine in patients who used it frequently.
Mary E. O’Sullivan (1902–1950) (Fig. 7) was the daughter of labour leader and social reformer Mary Kenney O’Sullivan and Boston Globe labour editor John O’Sullivan. She received her MD from Boston University in 1931. She trained in neurology at Bellevue Hospital in New York, under the tutelage of Robert Foster Kennedy. She subsequently worked at Bellevue Hospital, the NYU Clinic, the New York Infirmary, and St Vincent's Hospital. At Bellevue she was the chief of the migraine clinic.

Mary E. O’Sullivan. Reproduced with permission from Boston University School of Medicine.
In 1936, O’Sullivan discussed her experience in treating over 1000 attacks of migraine with ergotamine tartrate (33). She did not recommend using oral ergotamine on a daily, preventive basis, noting that ‘migraine is a protracted condition and we do not know what serious effects the daily use of the drug over long periods of time may have on our patients’ (33). O’Sullivan (33) described the following patient with ergotamine-overuse headache:
‘One … [patient] … took the pills, two or three at a time, the minute she felt an attack appearing. This dosage seemed to stall off an episode for that day, but it usually reappeared on the following one, necessitating further therapy. She continued in this manner for several months and was taking therefore two or three pills daily, or approximately 10–21 mg of the alkaloid a week. We have advised against this medication and are administering the drug hypodermically. If the attacks occur twice a week she receives 0.5–1 mg a week, because her headaches are completely terminated by 0.25–0.375 mg when the alkaloid is given subcutaneously’ (p. 1210)
Of her 97 patients treated with subcutaneous ergotamine tartrate, however, only three noted an increase in headache frequency after starting the medication (33). She did not feel this frequency change was due to the ergotamine itself, noting the unpredictable nature of migraine (33). She stated that ‘ergotamine tartrate has no effect on the frequency of attacks’ (33).
Boris P. Silfverskiöld (1912–1993) (Fig. 8) was a Stockholm neurologist. Along with Kirstein, he is credited with the first description of familial startle disease, or hyperekplexia (34, 35). He published extensively on the neurological complications of alcohol abuse.

Boris P. Silfverskiöld. Courtesy of the National Library of Medicine.
Silfverskiöld wrote about ergotamine tartrate (Gynergen) abuse in 1947 (36). He commented that ‘I have chanced upon no less than 7 patients who had begun to take increasingly large doses of Gynergen and had gradually got into a sort of “migraine status” with almost daily attacks’ (36). He (36) further stated:
‘It was common to all of them that they became worse after the Gynergen treatment was begun. The attacks became more and more frequent, they had taken Gynergen more and more often—two injections a week to two a day; in one of the cases besides large quantities of tablets. Finally, a sort of “migraine status” supervened. In three, or possibly four, of the cases a considerable improvement appeared when the abuse of Gynergen was discontinued. It has not yet been possible to persuade the other three to cease their injections’ (p. 284)
Silfverskiöld clarified that ‘I do not wish to maintain that in these seven cases Gynergen medication had a specifically deleterious effect, although that is possible’ (36). He did advise that ‘with increasing frequency of the attacks it will often be appropriate not to increase the dose of Gynergen’ (36).
Peters and Horton clearly identified ergotamine-overuse headache in their classic paper of 1951 (3, 37), and they recommended a withdrawal treatment programme in 1963 (38). Prior authors have reviewed this contribution in detail (37).
John Graham (1909–1990) (Fig. 9) was a distinguished headache specialist from Boston. After graduating

John Graham. Reproduced with permission from the American Headache Society.
Graham believed that there were two types of migraine (big and small), and did not accept the concept of tension-type headache (44). He alluded to this in his 1955 monograph on migraine when he stated that ‘headaches that present primarily [with] the features of the “tension headache” … [may] nevertheless have a vascular element that responds to ergotamine tartrate’ (45). He lists these ‘tension headaches’ under the title ‘migranoid disorders’ (45).
Graham referred to medication-overuse headache and chronic migraine as ‘migraine status’ (45, 46). It is clear in reading his writings that he is not referring to IHS status migrainosus when he uses this term. When describing the duration of migraine in his 1955 text (45), he states:
‘The pain may last only a few minutes in mild attacks, or may go on for several days in severe attacks; occasionally, the frequency of individual attacks may become so great that the patient is suffering from continuous headache and may said to be in “migraine status”’ (p. 21)
He further defined migraine status in 1968 when he wrote that ‘a few unfortunate individuals may experience increasingly frequent attacks of common migraine until they become daily in occurrence and the patient may be said to be in “migraine status”’ (46).
Graham agreed with Lennox, Peters, and Horton that ‘frequent doses of ergot, although they stop the headache of the moment, tend to foster the development of the next headache’ (45). In those circumstances, he recommended that ‘withdrawal of ergot, usually under hospital conditions, and substitution of other forms of therapy seem indicated if the patient can be persuaded to comply’ (45).
Graham (45) summarized his thoughts about medication-overuse headache in 1955:
‘When [migraine status] occurs, plans should be made for a long and difficult siege. Hospitalization of the patient is almost a
The steroids Graham was referring to were cortisone and ACTH (45). He commented that ‘in certain desperate situations of “migraine status” their use may be justified’ (45). Graham stated in 1968 that his ‘status migraine’ patients ‘nowadays usually have become physiologically dependent on ergot derivatives, but the same undesirable state may be reached without their help’ (46).
Caro Lippman (1886–1954) (Fig. 10) graduated from Harvard Medical School in 1910. He also studied under Paul Ehrlich in Germany. He subsequently established a private practice in San Francisco. Lippman gave the first description of the ‘Alice in Wonderland’ syndrome, which refers to distortions of body image usually in the setting of migraine with aura (47, 48). He also coauthored a book entitled

Caro Lippman.
Arnold Friedman (1909–1990) (Fig. 11) was a New York neurologist and headache specialist. He received his MD from the University of Oregon. He interned and took his residency training at Los Angeles County Hospital, and did a fellowship in neurology at Harvard Medical School (51). In 1945 Friedman founded the Headache Unit at Montefiore Hospital in New York City, the first such specialized clinic in the world (51). Friedman was the Chairman of the

Arnold Friedman. Courtesy of the National Library of Medicine.
Friedman was well aware of ergotamine-overuse headache. In a 1955 paper (53) on ergotamine tolerance in patients with migraine, he noted that:
‘Over a period of time, each patient noticed that the attacks were appearing more frequently and that the response to the same dosage became less dramatic. Each patient gradually began to increase the dosage of the medicament, some on the advice of the physician, others without his knowledge. With differences in time, each patient arrived at the same end-point, namely, daily episodes of migraine and a daily intake of ergotamine’ (p. 884)
In one patient, Friedman withdrew the ergotamine by using dihydroergotamine for 2 days and decreasing doses of amobarbital (sodium amytal) for 10 days (53). In 1959, he (54) outlined his ergotamine withdrawal protocol further:
‘In our experience these patients can be taken off the medication quite comfortably in three to five days by using adequate doses of Compazine or Sodium Amytal. Such therapy should be done in a hospital setting or under strict surveillance at home’ (pp. 241–242)
Discussion
Chronic migraine
The concept of chronic migraine has been mentioned in the literature for centuries. Thomas Willis documented a patient with chronic migraine in 1672. Willis was treating Anne, Countess of Conway, a noted English philosopher. Anne's headaches began at age 12, occurred intermittently for a period of time, and then became continuous. She died at age 48 of unclear causes (21). Her refractory headaches were also treated by William Harvey, Robert Boyle and others (21). About Willis’ description of Anne's headaches, Critchley (21) wrote in 1937:
‘We may pause for a while to ask ourselves what diagnosis would probably be made to-day in Lady Conway's case. Intractable and prostrating headaches, appearing first at puberty and persisting for 36 years, intermittent at first, almost certainly indicate a severe and chronic form of migraine. Their association with vomiting (mentioned in a letter from her brother), their frequent unilateral situation, their appearance “upon every light occasion”, the concomitant photophobia and intolerance to noise, their duration of 36 hours to four days, their conclusion in a heavy and disturbed sleep, are all strongly confirmatory. The absence of intellectual change, of epileptiform seizures, and of somnolence furthermore confirm the diagnosis of migraine and serve to exclude the grosser intracranial disorders such as tumour, aneurysm or hydrocephalus’ (p. 47)
The comments of Collier concerning chronic migraine and its treatment in 1922 seem to predict the results of the 2000 Spectrum Study. The Spectrum Study examined sumatriptan's effectiveness in treating the range of headaches seen in migraine patients (55). In a double-blind, placebo-controlled, multiple-attack study, Lipton et al. investigated migraineurs who also had phenotypic tension-type headache and patients with exclusive tension-type headache. Oral sumatriptan was equally effective in tension-type headache for the group of patients who had migraine and tension-type headache, but ineffective for the patients who had tension-type headache without any other headache types. The authors of the Spectrum Study thus suggested that the attacks of episodic tension-type headache and the attacks of migraine were pathophysiologically related, even though their symptom profiles varied (55).
Oppenheim, Balyeat, and von Storch described chronic migraine, although Balyeat more clearly defined it. There is a separate section in Balyeat's migraine book entitled ‘chronic migraine’, and the term is included in the index. The photo of a chronic migraine sufferer published in his text will be familiar to all headache specialists (Fig. 12). The four cases at the end of Balyeat's book would meet the ‘1995’ Silberstein et al. criteria for transformed or chronic migraine, although they would probably not meet the current IHS criteria for chronic migraine because the acute exacerbations do not clearly occur 15 or more days per month. Although his allergic theory has not stood the test of time, Balyeat's clinical observations have. His comment that 5% of his patients had chronic migraine is interesting, since CDH occurs in approximately 4% of the population (56).

A patient of Ray Balyeat's with chronic migraine. The legend in his 1933 book (28) read ‘Patient with chronic migraine. Note expression of one worn and depleted from continued pain. Headaches began at 5 years of age and have occurred every 3 or 4 weeks since, until 5 years ago, at which time they became continuous. There are now periods of exacerbation, during which time evidence of cortical involvement is always present. Not uncommonly a migraine patient during the late thirties or early forties will develop chronic headache’. From Balyeat R. Migraine: diagnosis and treatment. Philadelphia: J.B. Lippincott, 1933. Reproduced with permission from Lippincott Williams & Wilkins. ”Lippincott Williams & Wilkins.
Medication-overuse headache
Medication-overuse headache has been written about for decades. Lennox mentioned that headache frequency could increase with frequent ergotamine use, but he did not identify the need to taper the ergotamine in this circumstance (32). O’Sullivan recognized that daily oral ergotamine was to be avoided and described a patient with daily headaches secondary to daily ergotamine intake (33). However, she commented that subcutaneous ergotamine use had no significant effect on headache frequency (33). Silfverskiöld further described ergotamine-overuse headache, but took a non-committal position (36), and did not describe it with the clarity of Peters and Horton (3). Graham, Friedman, and Lippman deserve credit for separately reporting the first ergotamine withdrawal programmes in 1955 (45, 50, 53). Friedman described his ergotamine withdrawal protocol further in 1959 (54), and Horton and Peters published their withdrawal protocol in 1963 (38).
Chronic migraine and medication-overuse headache are not new concepts. The criteria offered by Silberstein et al. for transformed or chronic migraine were a great help in spurring interest and research. Formal IHS criteria should encourage further investigation.
Copyright disclaimer
All attemps have been made to locate the copyright owners of the photos and artwork used within this article. Copyright ownership has been acknowledged where available.
Footnotes
Acknowledgements
The authors thank Mayo Clinic history of medicine librarian and archivist Alexander E. Lucas for his assistance in collecting biographical information and historical images.