
Abstract
Introduction
Migraine ranks as the second most prevalent primary headache disorder. It is the major cause of disability among patients with primary headache disorder, causing significant functional impairment, which include both physical and psychological components.1, 2 According to the Global Burden of Disease (GBD) Survey around 1·04 billion had migraine, with an estimated global prevalence of 14.7% in both genders, and it was found to rank third among the most common disease worldwide.1–4 Although migraine has an insignificant association with mortality, headache disorders adversely affects disability-adjusted life years (DALYs) in excess to the collective neurological disorders. 5 Migraine also has a sizable impact on vitality of patient’s leisure and social activities.6, 7 Measurement of migraine-specific quality of life (MSQoL) and migraine-related disability (Migraine Disability Assessment Scale, MIDAS) are important approaches in comprehensive evaluation and management of migraine.8–11 Despite the high prevalence rates it continues to be underdiagnosed and undertreated. Clinicians often tend to focus on therapeutic aspects and fail to acknowledge the functional disabilities and psychological impact of the disease, leading to a shortcoming in a multifaceted approach to the disease. There is a paucity of data in Indian population, pertaining to the disability and level of well-being in migraine patients. Hence, this study aims to assess the severity and factors predicting disability and impairment in quality of life (QOL) secondary to migraine.
Materials and Methods
This is a descriptive study done at a tertiary care hospital. One hundred and eight consecutive individuals with migraine visiting headache clinic were interviewed by same neurologist. The diagnosis of migraine headache, with or without aura, was made using updated definition of the International Headache Society. 12 Persons aged 18–19 years with the diagnosis of migraine participated in this study. Individuals with other types of headache either primary or secondary headaches, and those with medical co-morbidities were excluded.
An organized set of questions were used to collect information regarding demographic factors of the population under study. Details of headache attributes comprising of duration since symptom onset, duration of acute attacks, and frequency were analyzed. The Headache Impact Test-6 (HIT-6) was used to quantify the disruption in the daily life of the patient caused by migraine. 13 This questionnaire that comprises six primary constituents, includes factors ranging from intellectual impairment to social dysfunction. Elevated scores imply a proportionately unfavorable effects of headache on the daily functioning of the respondent. MIDAS9, 14, 15 was used to quantify migraine-related incapacitation over a three-month period. This score is computed based on quantification of absenteeism from work or school, reduced fruitful output both at work and home, hampering of educational enterprises, and dysphoria in leisure activities. The higher score indicates more severe disability. MSQoL version 2.1 was used to assess the QOL in migraineurs. 16 This questionnaire, which comprises of 14 components, encompasses all aspects of health associated routine functioning of life by focusing on three central aspects of the individual’s role as a family member, in society and his/her emotional well-being. Higher scores in these domains suggest that QOL is more adversely affected. The Hamilton Anxiety Rating Scale (HAM-A) was used to quantify the magnitude of anxiety. It comprises of 14 components each of which incorporates a set of clinical manifestations, which in turn compute both the mental and physical burden of anxiety. 17 Hamilton Depression Rating Scale (HAM-D) was utilized to gauge depression among the study patients. It has 17 elements concerned with symptoms of depression encountered by the patient over the preceding week. 18
In this study, we aimed to estimate the severity of disability and impairment in QOL secondary to migraine and to enumerate and analyze the factors predicting severity of the same. Moreover, we also aimed to probe the additional impact of coexisting psychiatric dysfunctions—anxiety and depression on overall QOL.
Data were analyzed using SPSS software version 18.0. 19 Computation of discrete variables was done using measures of central tendency. Computation of qualitative/non-numerical values was done using frequency and percentage. The normalcy of the data was checked by applying the Kolmogorov–Smirnov test. Analysis of correlation between psychiatric comorbidities and results from the aforementioned scales were done using the Spearman’s rank correlation coefficient. P value less than .05 was considered statistically significant.
Results
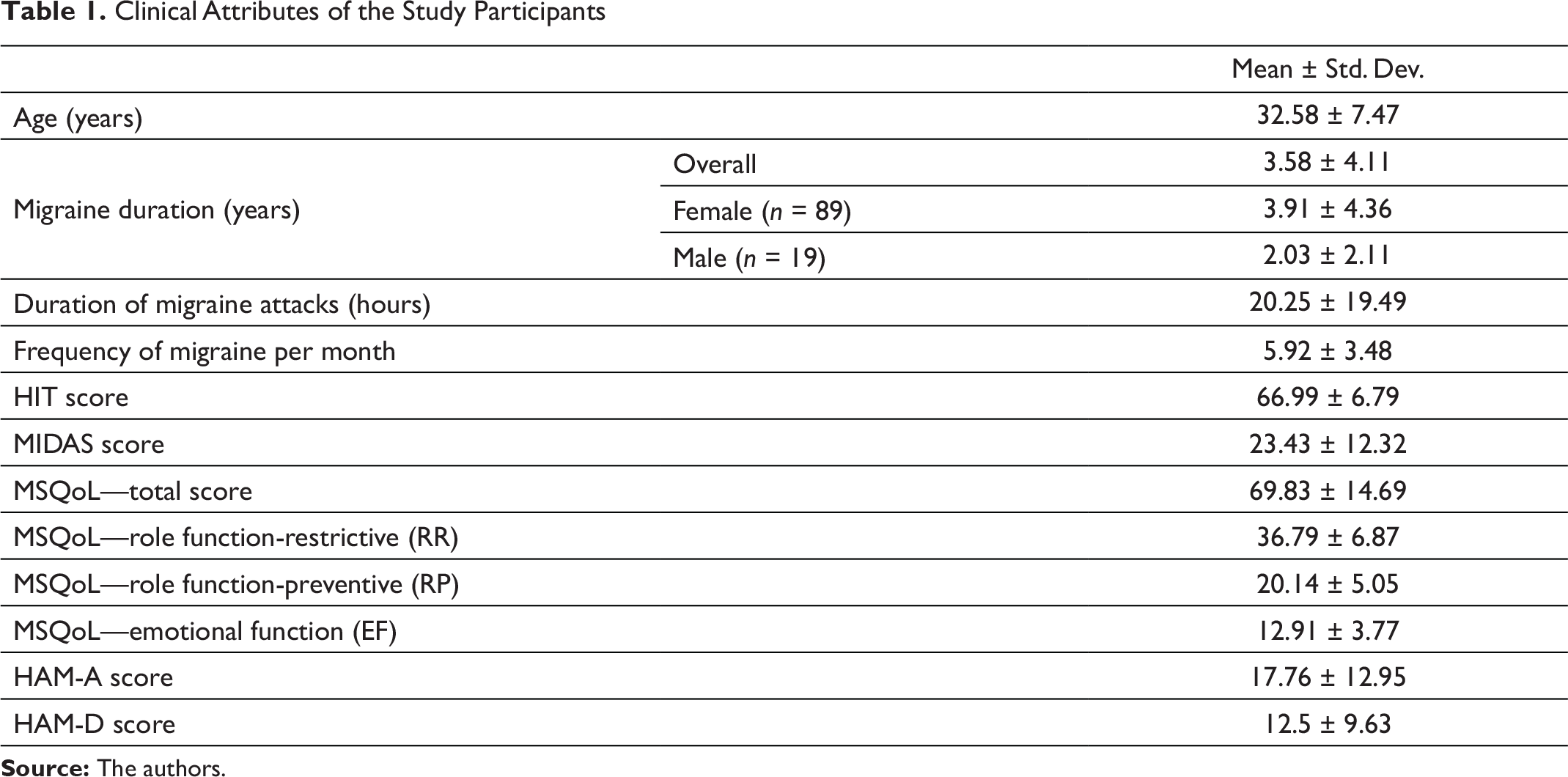
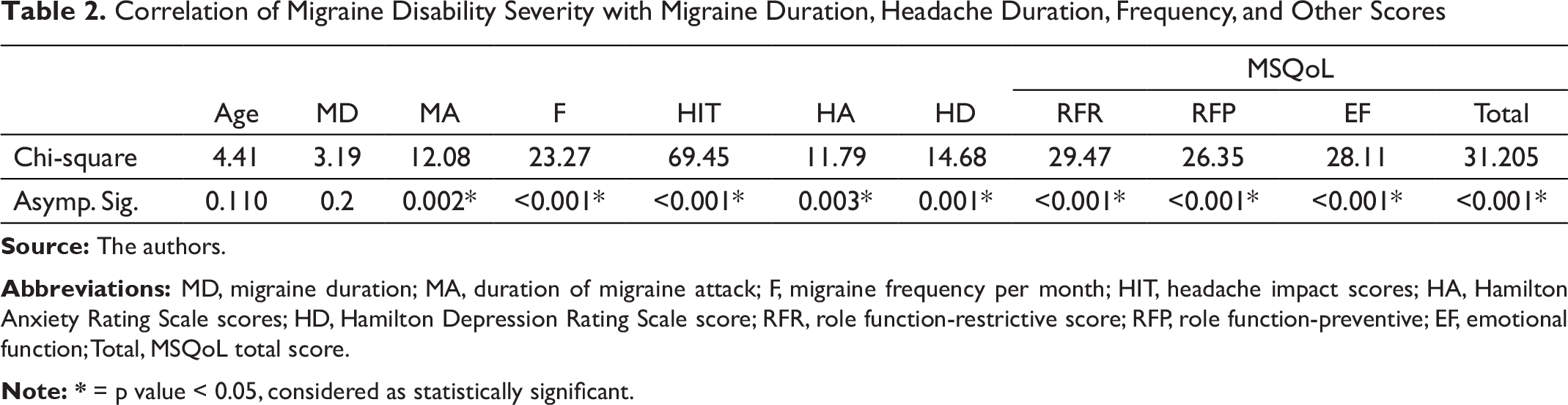
A total of 108 migraineurs were studied of which 89 were females. The age of the study group was 32.58 ± 7.47 years, and most were in the age group of 20–21 years. The clinical attributes of the study participants are explained in Table 1. With increasing age of the individuals, the duration of migraine attacks and migraine duration were more. However, age did not have an effect on frequency of migraine episodes. The HIT scores in the study was 66.99 ± 6.79, indicating headaches had substantial to severe impact on them. The MIDAS score was 23.43 ± 12.32 and most were found to have a grade III to grade IV disability indicating significant migraine-related disability. In Table 2, migraine disability severity is correlated with other parameters as shown there. The duration of migraine attacks, more frequent migraine attacks per month along with higher HIT score and coexisting anxiety and depression had a positive co-relation with severity of disability. MSQoL score was 69.83 ± 14.69. The MSQoL in all the domains was affected significantly. When MSQoL scores were compared with other parameters as shown in Table 3, there was a positive co-relation of MSQoL scores with duration of migraine attacks, frequency of migraine, MIDAS score, HIT score, HAM-A and HAM-D scores, and a negative co-relation with migraine specific QOL. As shown in Table 4, there was coexisting psychiatric comorbidity of anxiety in 30.6% and depression in 27.8%. Those with coexisting anxiety and depression had more frequent migraine attacks, longer duration of migraine attacks along with statistically significant effect on migraine QOL.
Clinical Attributes of the Study Participants
Clinical Attributes of the Study Participants
Correlation of MSQoL Scores with Migraine Duration, Headache Duration, Frequency, and Other Scores
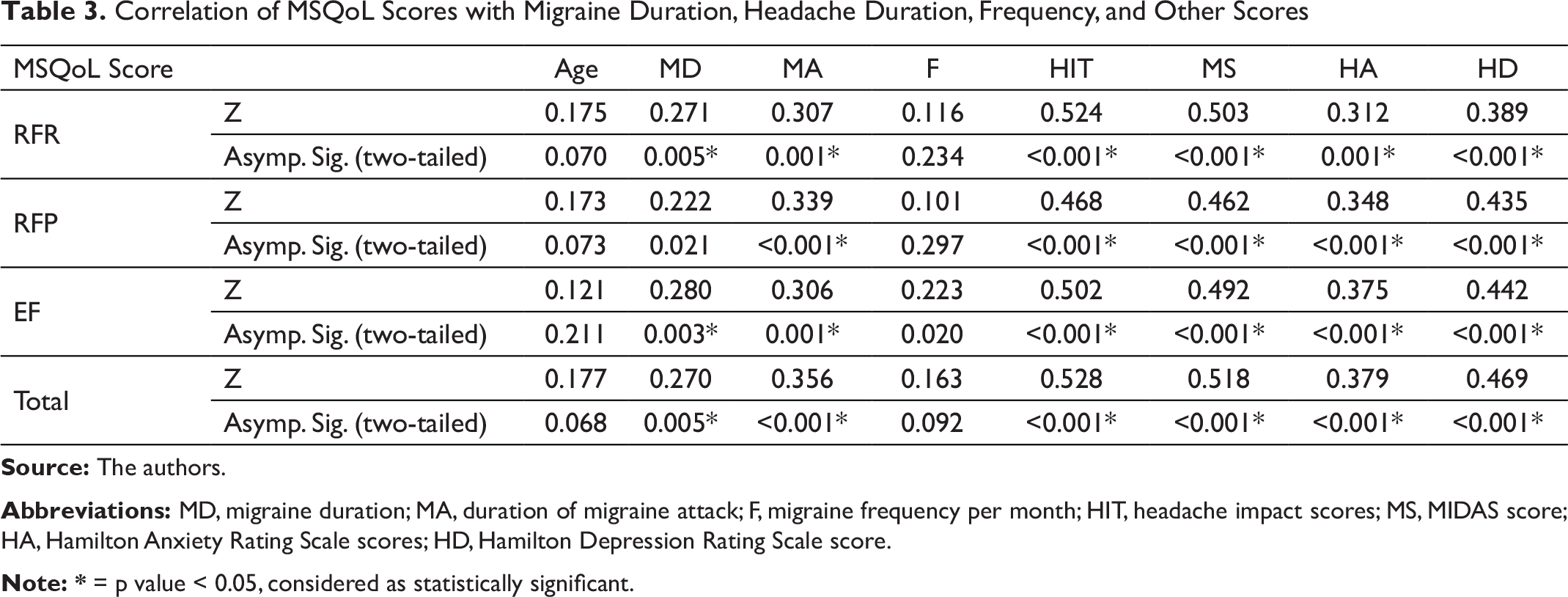
Abbreviations: MD, migraine duration; MA, duration of migraine attack; F, migraine frequency per month; HIT, headache impact scores; MS, MIDAS score; HA, Hamilton Anxiety Rating Scale scores; HD, Hamilton Depression Rating Scale score.
Correlation of Psychiatric Comorbidity with Quality of Life
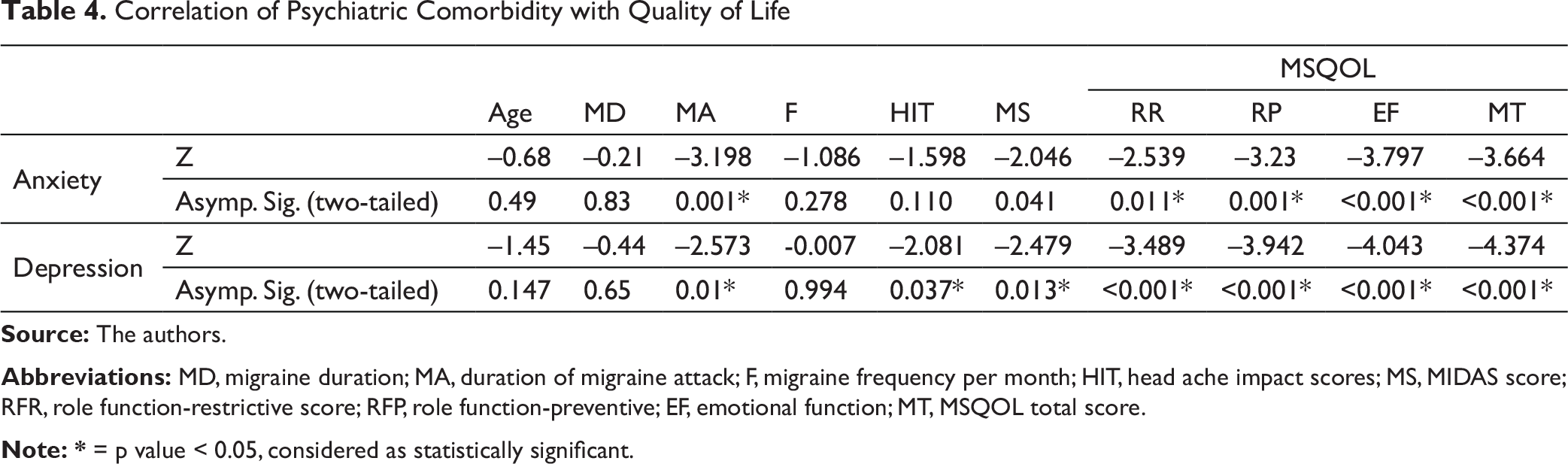
Abbreviations: MD, migraine duration; MA, duration of migraine attack; F, migraine frequency per month; HIT, head ache impact scores; MS, MIDAS score; RFR, role function-restrictive score; RFP, role function-preventive; EF, emotional function; MT, MSQOL total score.
Discussion
Primary headache disorders interfere with the normal daily functioning of a person both at the workplace and home. In addition to negatively influencing the patient by reducing the productivity, it also causes a strain on the family members and on the society at large. Consequently, both professional and personal dimensions are adversely affected. Thus, migraine is regarded as a incapacitating disease that can notably reduce the QOL of sufferers.20, 21 As found in many other studies,21 migraine was disproportionately more in females. In this study, migraine was known to be highest in the individuals aged 30–39 years, which is similar to other studies,21 affecting the sufferers at one of the most productive phases of their life. Though studies22 have reported gender differences having an impact on QOL, there was no gender difference on impact of QOL in the present study; however, males used to seek earlier medical care. Multiple studies23, 24 done in the past have found that most of the migraineurs had moderate to severe disability (MIDAS grade III and IV), which is also similarly seen here. Despite the absence of neurological deficits, morbidity due to intense pain and associated symptoms disrupts the normal functioning of an individual. In our study, headache attributes, such as pain intensity, duration of migraine, and frequency, were found to negatively correlate with health-related quality of life (HRQoL), in concordance with other similar studies.24–26 Migraine-related disability as evidenced in this study is also a significant predictor of poor HRQoL. 27
Migraine is also associated with emotional and mental distress and in recent times focus has been on disease specific disability and impairment on QOL including presence of coexisting psychiatric diseases. Similar to other studies,26, 28, 29 our patients were found to have coexisting anxiety and depression. Concurrent presence of anxiety and depression was noted to add to the magnitude of disease-related disability and diminished QOL. 30 Our study is concordant with many other studies done worldwide.31–34
Conclusion
The present study concludes that among migraineurs seeking treatment there was a moderate to severe impairment in disease specific QOL and related disability. The longer duration, more frequent migraine attacks and headache with substantial to severe impact are predictors of migraine-related disability and MSQoL. Coexistent psychiatric diseases further worsen migraine-related disability and reduce QOL. Hence, evaluation of migraine headache must be comprehensive and should also include assessment of psychiatric status of the patient, thus providing an efficacious management.
Limitations of the Study
The scales utilized in this study were disease specific. However, comprehensive criteria assessing overall general health status of the individual were not considered by us.
The study sample size chosen was small as this was a pilot study done to look for a comprehensive management of migraine. However, future research using larger sample size and strategies for reducing bias is needed.
Author Contributions
P. R. was involved in conceptualizing and designing the study, review of clinical studies and literature, acquisition of data, preparation and editing of manuscript.
N. S. C. was involved in designing the study, review of clinical studies and literature, acquisition of data, preparation of manuscript.
H. S. was involved in conceptualizing and designing the study, review of clinical studies, acquisition of data, preparation and editing of manuscript.
R. K. was involved in analysis of data and statistics
The manuscript complies with ICMJE guidelines.
Ethical Statement
This study was approved by IEC (institutional ethical committee). All the participants were briefed about the study and were involved after taking written informed consent.
Ethical Committee Approval Number
JSSMC/IEC/2308/12 NCT/2015-16.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.