
Abstract
The classification of patients with migraine who develop chronic daily headache is controversial, with some classifying such patients as ‘transformed migraine’. We compared patients with intermittent migraine attacks and patients with transformed migraine in terms of mean headache intensity on days with headache, depression, pain-related anxiety and headache-related disability. Patients classified clinically as also having tension-type headache were excluded. Aside from the number of days with headache per month, patients with intermittent migraine attacks and patients with transformed migraine were very similar in terms of all parameters studied. Our results support the concept that these two headache groups are closely related.
Introduction
Diagnosis of a headache disorder is typically based upon criteria of symptoms and characteristics. The most widely used diagnostic criteria at present are those of the International Headache Society (1), which rely on the clinical features of the patient's history including headache duration, location, severity, other pain characteristics, exacerbating factors and associated symptoms. Despite such efforts at classification, not all headaches fit well into these established criteria. For over a decade it has been observed that some patients who initially meet all migraine diagnostic criteria experience increasing headache frequency over time and eventually develop chronic daily headache (2, 3). This evolution from intermittent to chronic daily headaches is the basis of the ‘transformed migraine’ classification. According to Silberstein et al. (4), transformed migraine (TM) is characterized by episodic migraine, which often begins in the teens or twenties and then ‘transforms’ into a more frequent, and often less intense, headache. Associated migrainous features (e.g. photophonia and nausea) may also become less severe. Analgesic overuse may be associated with this migraine transformation (2, 3, 5), yet despite terminating the analgesic overuse some patients with this syndrome do not improve (6). Also, some patients appear to develop transformed migraine in the absence of analgesic overuse (3) and therefore it is unclear what mechanism(s) produce the transformation from intermittent to persistent headache.
Only a minority of migraine patients undergo this evolution from intermittent migraine attacks to a pattern of very frequent and often daily headache. The 1-year prevalence of migraine in adults in western countries is approximately 15% (7% in males, 24% in females) (7, 8). If only individuals with self-defined severe headaches are included, approximately 18% of adult females and 6% of adult males suffer from migraine (9). The prevalence of transformed migraine is much lower, approximately 1.3–2.4% (10, 11). Like migraine, TM is much more common in women than in men, with migraine showing a female : male ratio of approximately 3 (7, 8) and TM showing a female : male ratio of 2.4 (10). This similar sex ratio might suggest a close relationship between patients classified as migraine using IHS criteria (1) and patients classified as TM using the criteria of Silberstein et al. (4) and also raises the possibility that these headache types are part of a continuum of migraine headache.
The diagnostic entity of transformed migraine is not accepted by all (12) and there are those who feel that many of these patients are best classified as patients with migraine attacks and chronic tension-type headache attacks. At the same time, it has been proposed that migraine and tension-type headaches are separate disorders, because the prevalence of tension-type headaches was found to be similar in patients with migraine and in patients who did not have migraine (13).
Our objective was to compare two groups of patients, one group with IHS migraine and one group with TM (4), on measures of depression, pain-related anxiety and headache-related disability, in order to help determine if these two headache diagnoses are related.
Methods
Procedures
All patients referred to a university subspecialty headache clinic in Calgary were sent headache diary sheets and several questionnaires, including the Beck Depression Inventory (BDI), the Pain Anxiety Symptom Scale (PASS) and the Headache Disability Inventory (HDI), several months prior to their appointment. Completed questionnaires and headache diaries were brought by the patients to their first appointment, at which time a headache diagnosis was made by one of the two clinic neurologists. Patients with migraine were diagnosed according to IHS diagnostic criteria and patients with migraine who had headache on more than 15 days a month were diagnosed with TM according to the criteria of Silberstein et al. (4).
Patients
Entry criteria for this study included a diagnosis of migraine or TM. Patients who had been given a diagnosis of other headache types (i.e. tension-type headache) in addition to migraine were excluded. Also excluded were patients who, for any reason, had not completed all the questionnaires or kept headache diaries.
Assessment measures
Beck Depression Inventory (BDI)
The 21-item BDI (14) measures the severity of key symptoms associated with clinical depression (e.g. sadness, hopelessness, fatigue, loss of pleasure, feelings of failure, guilt, suicidal ideation, irritability). The BDI scoring system produces a total score ranging from zero to a maximum of 63, with ranges of scores indicating the presence of different levels of depression.
Pain Anxiety Symptom Scale (PASS)
The PASS is a 40-item self-report instrument designed to assess four aspects of anxiety associated with clinical pain symptoms: cognitive anxiety (racing thoughts, agitation and impaired concentration), fearful appraisal (catastrophic thinking and apprehensive expectations), escape and avoidance (behaviours associated with avoidance of activities out of fear of making the pain worse), and physiological anxiety (increased somatic awareness and autonomic physiological arousal associated with pain flair-ups) (15).
Headache Disability Inventory (HDI)
The HDI is a 40-item self-assessment scale designed to facilitate the clinician's assessment of the headache patient's experience (16, 17). The HDI measures the patient's perception of the functional and emotional impact of their headaches, thus quantifying the impact of headaches on daily living.
Headache diaries
The patient diary forms requested that patients record their headache intensity using a 0–10 scale (0 indicated no pain, 10 indicated pain as severe as it could be) for each of three segments of the day (morning, afternoon and evening/night). Any calendar day with a headache intensity score of greater than zero in one of the daily segments was considered a day with headache. Headache frequency was measured as days with headache per month. Headache intensity for a day with headache was determined by averaging the pain intensity values entered by the patient in the three segments during a calendar day (including zeros).
Data analysis
Using the t-test for independent groups, migraine and TM patients were compared on measures of mean number of headache days per month, mean headache intensity on headache days, depression, anxiety and disability.
Results
Of the 121 patients who completed all questionnaires, 87 met study entry criteria: 50 with migraine and 37 with TM (15 with analgesic overuse and 22 without analgesic overuse). Forty (80%) of the migraine patients and 32 (86.5%) of the TM patients were female. Mean patient age was 43 years (range 23–66) for the migraine patients and 37 years (range 17–69) for the TM patients. The diagnoses for the patients excluded included: tension-type headache (n=4), cluster headache (n=2), idiopathic stabbing headache (n=1), new daily persistent headache (n=3), hemicrania continua (n=1), acute post-traumatic headache (n=6), cervicogenic headache (n=2) and patients with more than one type of headache (i.e. migraine and tension-type headache) (n=15) (these 15 patients were all patients with intermittent migraine who had some associated tension-type headaches). Patients with migraine and more than 15 days of headache a month were classified as TM (4).
Days with headache per month
Clinic neurologists generally applied the diagnostic criteria of Silberstein et al. (4), so by definition, all patients in our TM group had more than 15 headache days per month. In fact, most had headache every day. Mean headache days per month for this group was 26.92 (out of a 28-day month) (Fig. 1). Patients diagnosed as migraine typically had headaches approximately 15 days per month or less. As a referral population, our patients were no doubt drawn from the more severe end of the migraine spectrum, but they showed a variety of migraine frequencies. This variety is seen in the mean days with headache per month, which was 9.22 (range 1–18) for the migraine patients (Fig. 1). Original diagnoses were based on clinical features and diary data. A few patients with more than 15 days of headache per month were diagnosed as migraine and not TM by the headache clinic neurologists. A rigid dichotomous approach is not always appropriate in the classification of patients and therefore it seemed reasonable to leave these patients as migraine patients. Despite the few migraine patients with more than 15 days with headache per month, the difference in the number of headache days per month in our two patient groups was highly significant (P < 0.001). There was no overlap between our migraine and TM groups. The highest number of headache days for the migraine group was 18, whereas the lowest number of headache days for the TM group was 22. In fact, for our patient population as a whole, headache days per month showed a bi-modal distribution (Fig. 2), which reinforced our decision to base our patient classification on the clinicians' original diagnosis.

Mean number of headache days per month experienced by the migraine (n=50) and transformed migraine (n=37) patient groups are shown.
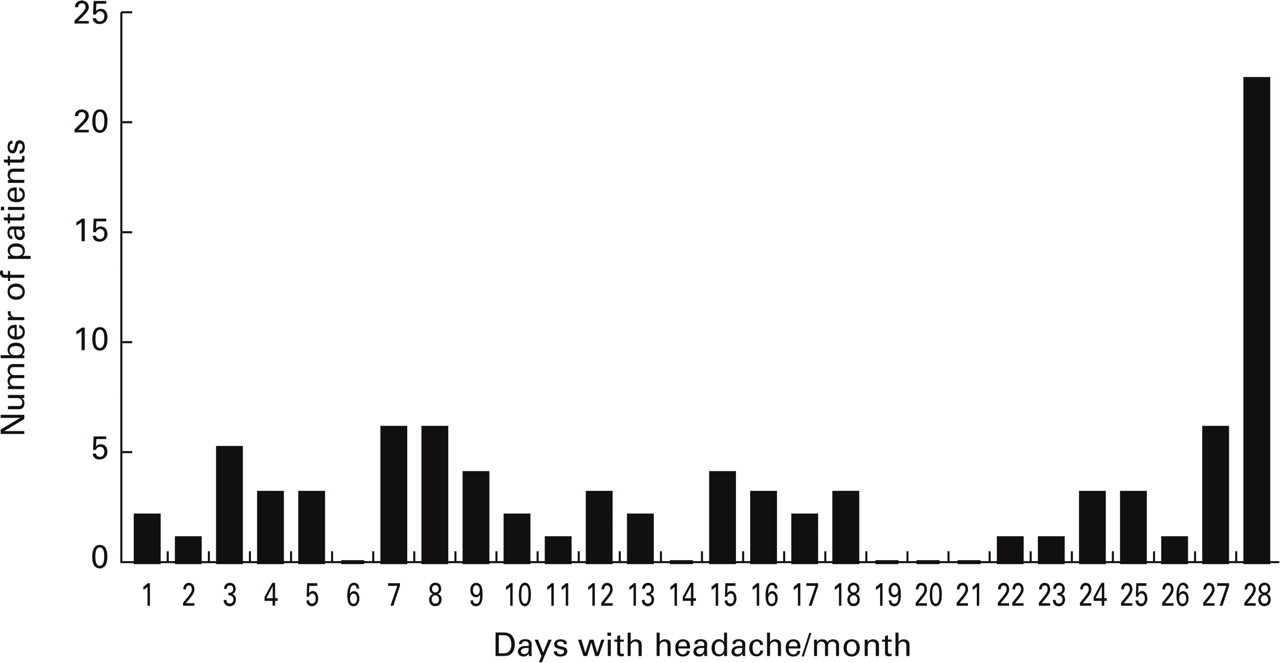
The number of patients reporting various numbers of headache days per month are shown. No patients reported 19, 20 or 21 headache days per month, suggesting a natural separation between patients with migraine and transformed migraine.
Headache intensity
Although migraine attacks are often said to become milder when patients evolve to a more chronic daily headache pattern, this was not apparent in our patient groups. Measuring intensity as mean headache intensity on calendar days with headache, we found that patients with TM had a slightly higher mean headache intensity (3.85 on a scale of 0–10) as compared with migraine patients (3.09 on a scale of 0–10). This difference was not significant (Fig. 3). Headache intensity scores for the TM patients ranged from 1.71 to 9.29 (median intensity 3.54) and 0.94–10 (median intensity 2.89) for the migraine patients.

Mean headache intensity on calendar days with headache is shown for the migraine patient group (n=50) and the transformed migraine patient group (n=37). Patients rated headache intensity on a scale of 0–10, with 10 representing pain as severe as it could be.
Depression
As a group, patients with TM had slightly higher mean scores on the BDI (10.65 ± 9.27) than the migraine patients (8.82 ± 7.39); however, this difference was not significant. The majority of both migraine and TM patients (> 70%) had levels of depression in the ‘none to mild’ range (Table 1).
Beck Depression Inventory scores in patients with migraine and transformed migraine

Pain-related anxiety
Analysis of the pain-related anxiety data revealed that the migraine and TM patient groups did not differ in their mean scores on the PASS fear, cognitive anxiety, escape/avoidance or physiologic subscales. Also, no differences were found between groups on total PASS scores (Table 2).
Pain Anxiety Symptom Scale scores in migraine and transformed migraine

∗±1 standard deviation.
Disability
Headache-related disability as measured by the HDI functional subscale, emotional subscale and total score did not differ between the migraine group and the TM group (see Table 3).
Headache Disability Inventory Scores in patients with migraine and transformed migraine

∗±1 standard deviation.
Discussion
Our objective was to compare patients with episodic migraine and TM on a number of parameters. We relied on the clinical diagnosis made by headache clinic neurologists to separate our patients into two groups. The neurologists used IHS diagnostic criteria (1), the criteria of Silberstein et al. for TM (4), the clinical history and physical examination, and the headache diaries brought in by the patients to their first visit. Patients who were felt by the neurologists to be suffering also from tension-type headaches to a degree that merited a separate diagnosis for these patients with relatively severe headache disorders were excluded, in order to exclude patients who might have tension-type headaches as their main headache disorder, but who also had some additional migraine attacks. As our focus was to compare patients with intermittent migraine and TM it seemed reasonable to keep our patient groups as well defined as possible. Although it has been shown that most migraine patients also have some tension-type headaches (13), in our setting only those migraine patients with relatively severe and clear-cut tension-type headaches in addition to their migraine would have received this diagnosis in addition to their migraine diagnosis. These patients were excluded from our study.
The diagnosis of TM is not accepted by all (12), and although diagnostic criteria exist (4) it remains problematic. One issue is that a relatively arbitrary figure of headache on greater than 15 days/month is used to separate patients with episodic migraine from those with TM. Our data suggest that this may not be the best ‘cut-off point’. In our patient population of 87 patients, all of whom had diary data, the patients showed a bimodal distribution of headache days per month. Patients appeared to either suffer from headache on 18 days per month or less, or had headache virtually every day. This may reflect the pathophysiological mechanisms that underlie the transition in some migraine patients from intermittent to very frequent headache.
More longitudinal prospective studies are needed (12) before we can hope to understand the relationship of chronic daily headache syndromes to the episodic headache types. However, as long ago as 1982, Mathew et al. (18) reported that in a series of 80 patients with chronic daily headache presenting to a headache centre, 76% had a history of episodic migraine in the past before the chronic daily headache developed. In 1987, Mathew et al. (19) further pointed out that some patients with a very similar chronic daily headache syndrome with many migrainous features appeared to have ‘daily’ migraine headaches from the start. Rothrock et al. (20) found that patients with chronic daily headache who evolved from episodic migraine, or who had chronic daily headache from the onset with many migrainous features, showed a large number of clinical and demographic similarities to patients with episodic migraine. Our objective was to explore further the differences and similarities between patient groups with episodic migraine and those with TM. If patients with TM evolve from a particularly small subset of migraine patients, or if in fact TM patients have more in common with chronic tension-type headache patients, significant differences between our two groups should have emerged.
By definition, our patients with TM had many more headache days per month than those with intermittent migraine. Mean headache intensity on calendar days with headache was not, however, significantly different between the two groups. This finding must be interpreted with caution, as patients were actively treating their headaches with symptomatic medications during the study. In addition, each daily mean headache intensity value was the mean of three intensity values recorded during the three time segments recorded each day in the diary. Low intensity values or even zero intensity levels during some segments of the day could therefore reduce the mean intensity level from that day's peak headache intensity value, and this is likely to account for the relatively low mean headache intensities of between 3/10 and 4/10 found in both patient groups, even though these were relatively severely affected headache patients.
Depression is more common in patients with migraine than in non-headache controls. In patients with relatively severe migraine, the lifetime prevalence of major depression was approximately three times higher than in a control group without a history of severe headache (21). Breslau et al. (22) found a lifetime prevalence of depression in patients with migraine of 40.7% as compared with 16% in non-headache controls. In our patients with intermittent migraine headaches, only 18% showed evidence of a moderate or severe depression on the BDI. However, this figure cannot be directly compared with that of Breslau et al. (22), as the BDI assesses only current depression, as opposed to a lifetime prevalence of depression. A lower prevalence rate in our study would therefore be expected. In fact, our mean BDI score of 8.8 in our intermittent migraine patients is very similar to a mean BDI score of 7.8 found by Holroyd et al. (23) in a sample of migraine patients who were seeking treatment at a university headache clinic.
As a group, the patients with TM in our study had slightly higher mean scores on the BDI than the patients with episodic migraine. This difference was not statistically significant and therefore it is difficult to determine the clinical relevance of this difference as most patients in both groups scored in the ‘no’ or ‘mild’ depression range. However, it is noteworthy that 29.7% of TM patients showed moderate or moderately severe depression, compared with only 18% in the migraine group. This might support the hypothesis that depression can be one factor that may lead to migraine transformation to a chronic daily headache pattern (19). Our failure to find a major difference between the episodic migraine and TM groups in terms of scores on the BDI suggests that these two groups have a similar biology.
Our finding that migraine and TM patients did not differ in terms of pain-related anxiety was unexpected. It might have been expected that the migraine patients would have lower levels of anxiety than the TM group, as patients who experience more frequent headaches might experience more anxiety because of their pain. On the other hand, it could be suggested that migraine patients would have higher levels of anxiety because they would be more likely to have an anticipatory element due to having intermittent pain. As a result they might be more anxious about their next headache. However, our findings revealed that not only did migraine and TM patients not differ on our measure of pain-related anxiety, but both groups reported relatively low levels of anxiety compared with the established norms of the PASS test in other painful conditions (McCracken et al.) (15). Our findings again suggest that migraine and TM are closely related headache disorders.
Our finding that mean headache-related disability, as measured by the HDI, was very similar in our two patient groups was also unexpected. TM patients are often considered to be quite disabled because of their high headache frequency. However, clinicians may have over-estimated the disabling effects of frequent headaches and under-estimated the amount of disability caused by intermittent migraine attacks. It may be important that our two patient groups had only a small difference in their mean headache intensity, particularly if headache intensity is the major determinant of headache disability. Our observations are consistent with those of Jacobson et al. (16), who also observed, using the HDI, that self-perceived headache disability increased with increasing headache intensity, whereas headache frequency did not significantly impact self-perceived disability.
Some limitations of this study should be mentioned. First, the intention of this study was to compare migraine and transformed migraine patients on measures of depression, pain-related anxiety and headache-related disability. While these factors are likely to also be impacted by other headache types, analysis of these headache types was not the purpose of this study. The results of our study may not generalize to the entire migraine population as our patients were drawn from a referral population and no doubt represent the more severe end of the migraine spectrum. Also, our sample size may not have been sufficient to detect small differences between our two patient groups.
Measurement of headache intensity also can be problematic. We used in our analysis the patient's mean headache intensity on calendar days with headache. Patients recorded their overall headache intensity for each of three segments in the day. It is possible that our comparisons of headache intensity between the two groups might have given different results if we had determined headache intensity in a different way, for example asking patients to provide their peak headache intensity for each day. Finally, it may be argued that patients who present with tension-type headache in addition to migraine may in some respects resemble transformed migraine patients and therefore this group should have been included in this study. As the purpose of our study was to compare patients with a well-established diagnosis of migraine or transformed migraine with the exclusion of such confounding variables as additional diagnoses, we excluded patients who had been given other headache diagnoses. However, an exploratory analysis showed that patients with a combined diagnosis of migraine and tension-type headache did not differ from patients with migraine or transformed migraine.
Despite the limitations of this study, our findings indicate that, aside from the number of days with headache experienced per month, patients with migraine and TM have more similarities than differences. They show only small differences in BDI scores and do not differ on measures of pain-related anxiety, headache-related disability or mean headache intensity on days with headache. Our results must be interpreted with caution as not enough information is available on how various headache types affect these parameters. However, our findings do suggest that patients currently classified as transformed migraine are indeed a part of the migraine disorder spectrum and not a distinct type of headache. Further research is needed to determine how transformed migraine is related to other migraine types.
Footnotes
Acknowledgements
This work was supported by Pfizer Canada Inc. We also gratefully acknowledge the contributions of Ms Constance Riess who tabulated the diary data, Ms Anila Umar who entered much of the data, and Mrs Pat Moss who helped prepare the manuscript.