
Abstract
Snake bite envenomation is a global health concern which is often overlooked. The World Health Organization (WHO) reports an annual estimate of 50,000–90,000 deaths worldwide due to snakebite. Snakebite outcomes vary based on factors like venom presence and type. Clinical features range from fang marks to bleeding, swelling, pain, and necrosis at the bite site. Elapid and certain Viperidae venom cause gradual neuro-paralysis, initially affecting eye and facial muscles, leading to ptosis, blurred vision, and diplopia. The diagnostic workup should consider quick assessment of the routine blood tests such as complete blood count, basic metabolic profile, prothrombin time, fibrinogen value and creatine kinase value. Oxygen therapy and intubation may be necessary for respiratory distress in neurotoxic snake envenomation. Analgesia, preferably opioids, is required for severe pain in viper bites. Supportive therapy includes establishing IV access, administering fluids, and vasopressors for hypovolemia. Antivenom administration is recommended for severe envenomation based on WHO guidelines, targeting systemic bleeding, shock, limb swelling affecting multiple joints, acute kidney injury, necrosis, and gangrene. There is a need to continue and conduct further research in the field of snake envenomation effects in Asia, America, Australia, Africa, and Europe. Cardiovascular and respiratory support is vital, and anti-snake venom (ASV) administration must consider potential adverse reactions. There is a need to focus on enhancing first aid, protocols, and long-term complication follow-up is essential. Research on anti-venom development and point-of-care tests for venom identification is pivotal for global snakebite management.
Introduction
Snakebite envenomation is a global health concern often overlooked, contributing significantly to the burden on healthcare services. The World Health Organization (WHO) has an annual estimate of 50,000–90,000 deaths globally due to venous snakebite. 1 In 2016, 81,000–138,000 deaths were recorded, with 1.8–2.7 million envenomation cases reported in Africa, Southeast Asia, and South Asia. 2 Limited access and awareness in these regions complicate clinical outcomes, as people rarely seek medical help or report incidents due to a lack of awareness about snakebite management. 3
Venomous snake species, particularly from the Viperidae, Elapid, and Atractaspididae families, pose a significant threat. 4 Apart from fatalities, snakebite envenomation leads to lasting complications, such as vision loss and limb amputation due to necrosis and gangrene. 5 In India, with 236 snake species, only a few are venomous, including the Cobra, Russel’s Viper, Saw-scaled viper, and Common Krait, responsible for most envenomation cases. 6
Factors contributing to the increasing morbidity and mortality include poor awareness, inadequate healthcare facilities, limited support, and the unavailability of anti-snake venom (ASV). In South Asia, most cases affect those employed in the agrarian sector. Recognizing the severity, the WHO urged member nations in 2018 to adopt strategies to address snakebite.7, 8 This review seeks to explore published articles on snakebite envenomation management strategies.
Methods
Literature Search Strategy
PubMed, ScienceDirect, and Web of Science were used to search articles on snake envenomation management. Keywords included snake envenomation, snake bite, management, and complications. The authors screened titles and abstracts, shortlisting relevant articles for review.
Literature Inclusion and Exclusion Criteria
The review includes relevant articles on snakebite management, focusing on reported cases seeking healthcare. It encompasses those reporting to primary healthcare centers and excludes cases not seeking healthcare and articles in non-English languages.
Burden of the Problem of Snake Bite
Globally, approximately 146.70 million people reside in areas with venomous snakes, often lacking accessible healthcare. 9 India bears half the global burden of snakebite deaths, with many fatalities occurring prehospital due to ASV unavailability. 10 In 2017, the WHO designated snake envenomation as a Category A topical disease.11, 12
Mechanism of Snake Bite
Snakebites, whether from venomous or non-venomous snakes, occur when a snake bites an animal or human. In Asia, the most venomous snakes belong to the Elapidae and Viperidae families.13–16 Viperidae includes Russel’s viper, saw-scaled viper, and various pit vipers, while Elapidae includes cobra, king cobra, and common krait.13–16 Venomous snakes possess fine, needle-like fangs connected to venom glands, injecting venom subcutaneously or intramuscularly based on fang length.17, 18 The fangs extend from the upper jaw and are linked to the snake’s venom gland, a modified salivary gland. 17 The venom delivery method varies depending on fang length. 18
Clinical Manifestations of Snake Bite
Snakebite outcomes vary based on factors like venom presence and type. Clinical features range from fang marks to bleeding, swelling, pain, and necrosis at the bite site. Venom effects may take time to manifest, influenced by post-bite anxiety, movement, catecholamine release, and increased blood pressure, facilitating venom spread to target organs.19–21
The systemic effects of snakebite may manifest as:
Neuro-paralytic effect: Elapid and certain Viperidae venom cause gradual neuro-paralysis, initially affecting eye and facial muscles, leading to ptosis, blurred vision, and diplopia.20, 21 Progression involves bulbar paralysis, limb, neck, respiratory muscle, and diaphragm paralysis.
22
Vascular effect: Hemolysis and coagulation abnormalities (vascular damage, platelet dysfunction, consumptive coagulopathy) may result from snake venom hemotoxins.22–25 This can lead to severe hemorrhage, including epistaxis, hematuria, mucosal, hematemesis, and intracranial bleeding.20, 21 Shock: Hemorrhage, plasma extravasation, heart dysfunction, sepsis, pituitary bleeding, and anaphylaxis can cause hypovolemic shock, jeopardizing the hemodynamic milieu.26–30 Acute renal damage: Kidney damage in snakebite results from hemorrhage, shock, microthrombi formation, and direct venom and myoglobin-induced harm to kidneys.31–34
Approach to Patients of Snake Bite
Snakebite victims, often panicked, necessitate prehospital care with essential precautionary measures to address their distressed state of mind.
Prehospital Care
In the aftermath of a snakebite, prompt attention and assistance are crucial. 35 The victim, aiming to stay calm and avoid panic-induced catecholamine release, should seek help from nearby individuals. Immobilization should be minimized, and efforts made to promptly transfer the patient to the nearest healthcare center. Sucking the bite site or cutting the area with a knife is discouraged.36, 37 While pressure immobilization is suggested in some reviews, its efficacy is limited, and concerns about tissue exposure to venom and increased local pressure exist.38, 39 A study in Myanmar noted its effectiveness against Russell’s viper bite, but caution is advised. 38 Traditional remedies, such as herbs or animal excreta, should be avoided. 40 Capturing the snake is risky, and even a decapitated snake can cause envenomation.41, 42 Instead, photograph the snake for identification. Suction devices have uncertain efficacy, removing only a small percentage of venom. Their use may complicate tissue damage. 43 Overall, adherence to evidence-based practices and swift medical attention are crucial in snakebite management. 44
Hospital Care
Upon hospital admission following a snakebite, a thorough evaluation is imperative, regardless of venom potency. Admission and a 24-hour observation, even for non-venomous bites, are recommended.
General management goals include:
Identifying life-threatening features Efficient analgesia for pain management Minimizing local tissue damage Addressing systemic envenomation features with supportive therapy Preventing and correcting hematologic complications Averting limb loss from compromised vascularity.
A standard airway, breathing, and circulation assessment, coupled with vital checks, ensures prompt attention to vitals and provision of adequate oxygenation and ventilation in case of breathing difficulties.
Obtaining History
Gathering the patient’s history post-snakebite involves crucial details such as timing, location, and site of the bite, aiding in epidemiological insights and snake species identification for effective management decisions.20, 21, 44, 45 While identifying the snake is important, overemphasis may lead to time loss; treatment should not solely rely on patient descriptions. 46 Additionally, inquiring about comorbidities like respiratory and heart diseases, along with medication details, is vital, especially for patients on anticoagulants or antiplatelets at risk of bleeding. 47
Clinical Examination
Local Examination
Local examination of the snakebite site is crucial, focusing on identifying two parallel fang marks, assessing swelling, bleeding, and blistering. 48 However, caution is needed, as other creatures may cause similar marks. Absence of fang marks does not rule out snakebite.48–52 Signs of lymph node involvement and lymphangitis, indicated by elevated, red, tender streaks, should be noted. 53 Careful examination for ligature presence, limb ischemia, swelling, necrosis, and infection around the bite site is essential.54–56
Systemic Examination
Neurological assessment in snakebite victims includes checking consciousness and signs of neurotoxicity like blurring of vision, ptosis, facial paralysis, muscle tenderness, and jaw stiffness. Sea snake bites exhibit unique jaw stiffness, differentiable from trismus by jaw opening upon applied pressure. 57 Hemotoxic findings, such as subconjunctival, nasal, gum, oral, and retinal bleeding, require careful examination. Internal hemorrhage in the peritoneal, intracranial, pleural, and pericardial cavities poses life-threatening risks to hemodynamic stability.20, 21
Diagnostic Workup
The diagnostic workup should consider quick assessment of the routine blood tests such as:
A complete blood cell count A basic metabolic profile Prothrombin time Fibrinogen level estimation Creatine kinase level estimation
Additional testing for systemic envenomation features includes liver function tests, urinalysis.
For systemic envenomation features, additional tests like liver function tests, urinalysis, and blood grouping cross-matching may be necessary. The 20-minute whole blood clotting test (WBCT), a simple yet effective test, can assess coagulopathy risk.58–60 Clinical validation studies reported WBCT sensitivity and specificity ranging from 82% to 89% and 82% to 98%, respectively. However, it may miss coagulation problems in some cases.61, 62 Urea and creatinine levels reflect kidney function, and hematocrit evaluation guides volume replacement measures.20, 21
Treatment and Medical Management
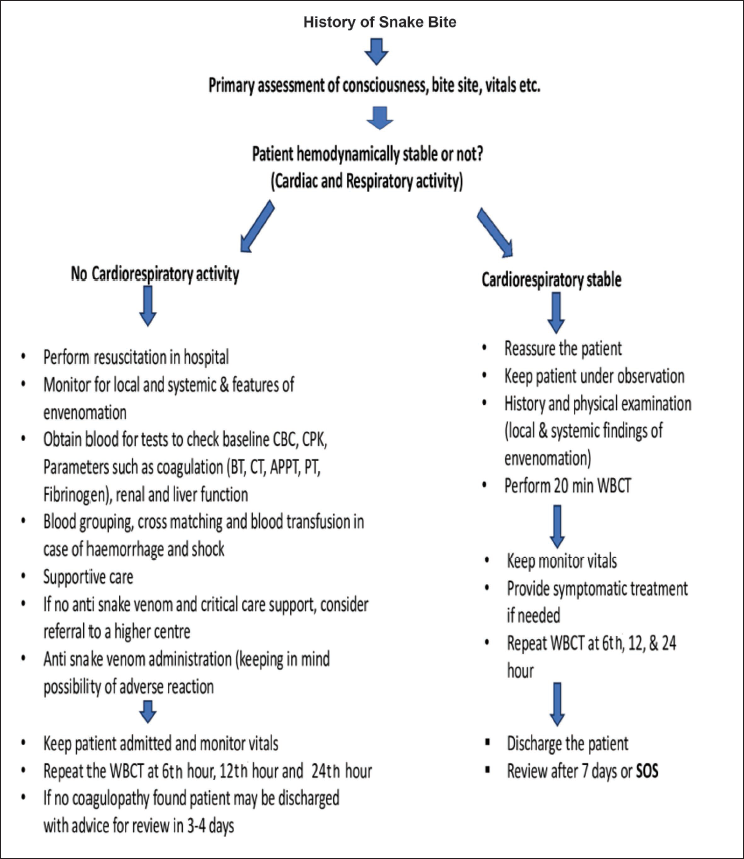
Oxygen therapy and intubation may be necessary for respiratory distress in neurotoxic snake envenomation. Analgesia, preferably opioids, is required for severe pain in viper bites. Supportive therapy includes establishing IV access, administering fluids, and vasopressors for hypovolemia. Figure 1 outlines general snakebite management.
Showing General Management of Snakebite.
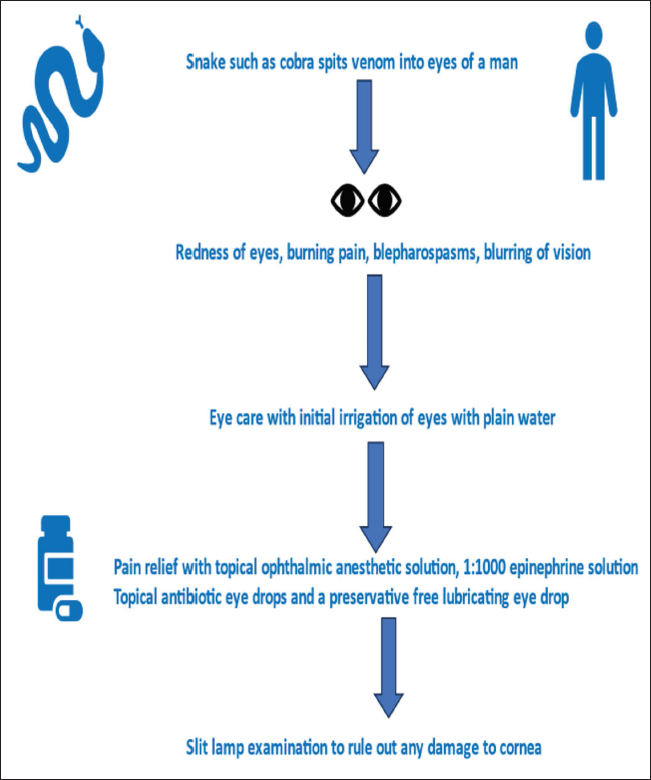
Cobras can spit venom into the eyes, causing severe discomfort and potential vision loss. Approach detailed in Figure 2.
Showing Treatment Approach for Snake Venom Ophthalmia.
Antivenom administration is recommended for severe envenomation based on WHO guidelines, targeting systemic bleeding, shock, limb swelling affecting multiple joints, acute kidney injury, necrosis, and gangrene.20, 21 Antivenoms are specific immunoglobulins from sheep or horse plasma hyperimmunized with regional snake venoms. 63 Early antivenom use effectively reduces neurotoxicity, myotoxicity, bleeding, renal damage, and tissue necrosis.20, 21, 64 Coagulation defects show partial correction within six hours post-antivenom.65–70 In the USA, CroFab, an anti-crotalid antivenom, addresses envenomation from various species effectively.71–74 However, complete recovery is not guaranteed, and antivenom efficacy in fully reversing envenomation features remains uncertain.20, 21, 65
Additional Therapeutic Requirements in Snake Envenomation
In neostigmine administration is crucial in elapid bites (cobra, krait, coral snakes) to counteract neurotoxicity by inhibiting peripheral cholinesterase and increasing acetylcholine levels, preventing paralysis.66, 67 Tetanus toxoid is recommended after coagulopathy ruling out, with booster administration if ruled out. Aspiration of large tense bullae minimizes rupture risk, and antibiotics address infection signs. Surgical debridement or amputation may be necessary in severe cases, with fasciotomy rarely required. 68 In eye entry cases, irrigation with water, saline, or milk minimizes venom effects. Severe eye pain may necessitate detailed examination, antibiotics, and cycloplegic eye drops. 69
Critical Points to Consider About ASV
ASV administration poses an anaphylaxis risk, necessitating careful observation for two hours post-administration. 26 The utility of pre-administration skin sensitivity tests lacks definitive evidence. Following FabAV, 8% of patients developed acute adverse reactions. 70 The North American Snakebite Registry showed that 2.3% of adults and 2.7% of children developed responses to FabAV, including rash (0.9%), hypotension (0.9%), and bronchospasm (0.9%). Another study on 1,340 patients reported a 1.4% incidence of acute adverse reactions to FabAV. 71 Anaphylactic reaction management involves withholding ASV and administering adrenaline, antihistamines, and glucocorticoids.72, 73 Late reactions (type III hypersensitivity) may require oral antihistamine or glucocorticoid prednisolone courses. 74 WHO recommends a five-day course for late reactions, with varying incidence (5%–56%) across studies.75–77
Long-term Sequelae to be Considered in Snake Envenomation Patients
Long-term complications post snake envenomation are under-researched. 78 A meta-analysis from Sub-Saharan Africa (1970–2010) reported 5,908–14,614 annual incidents of amputations due to tissue necrosis. 79 In Sri Lanka, 3% of 816 snakebite patients developed complications like joint stiffness and muscle wasting. 80 Blindness from eye exposure to venom was documented. 81 Chronic renal failure can lead to acute damage. 82 Neurological issues, including paralysis and cognitive decline, result from hemorrhagic disorders. Chronic hypopituitarism, presenting as fatigue and hormonal imbalances, persisted for over a decade post-envenomation in some South Asian cases.83–84
Post Hospital Admission Discharge Decision
The decision of discharging the patient from the hospital should be taken based on evaluating certain critical requirements such as:
Patient has received the antivenom course. Vitals have become stabilized. Any hematologic parameters are normalized and there is no bleeding anymore. Pain is controllable with oral analgesics. Patient can tolerate oral diet. Any pending consultation with neurologist, ophthalmologist, vascular surgeon is completed.
Scope for Future Research in this Field
There is a need to continue and conduct further research in the field of snake envenomation effects in Asia, America, Australia, Africa, and Europe. There is a need for conducting studies in the following areas:
High yield studies on the efficacy of first aid measures in snake envenomation including application of immobilization techniques which are presently employed in the field. Detailed, meticulous studies to assess the efficacy and safety profiles of the various antivenoms which are used in the various countries of the world. The potential risk of adverse reactions to antivenoms poses an ethical concern in convention phase I and phase II trials.
85
In a few literatures, it has been recommended that model-based trials, as done for anti-cancer research, may be done for studying the research and development of ASVs.86–87 Clinical trials to assess the clinical manifestations in envenomation by different snake species and for snake species identification. Observational studies to do follow up for long term complications in victims of snakebite for determining the clinical progression, severity, and common long-term sequelae in different geographic regions of the world depending on the type of snake species and subspecies. Clinical trials to develop cost-effective and easily available point of care test kits for diagnosis of the snake species venom from the blood and other biological fluid of the patient. Studies to assess the efficacy and safety of adjunctive treatment such as use of phospholipases A two inhibitors such as Varipladip and Varipladip-methyl, and toxin specific monoclonal antibodies and aptamers, and matrix metalloproteinase inhibitors such as Batimastat and Marimastat.87, 88
Conclusion
Snakebite, a global health concern, leads to significant morbidity and mortality due to poor healthcare accessibility and ASV unavailability. Managing snakebite has evolved, emphasizing initial reassurance, patient immobilization, and prompt hospital transfer. Identifying fang marks and assessing neurotoxic, hemotoxic, and myotoxic effects guide treatment. Baseline investigations, including blood clotting tests, kidney, and liver function tests, are crucial. Cardiovascular and respiratory support is vital, and ASV administration must consider potential adverse reactions. Focus on enhancing first aid, protocols, and long-term complication follow-up is essential. Research on anti-venom development and point-of-care tests for venom identification is pivotal for global snakebite management.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Not applicable.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.