
Abstract
Snakebite is a significant public health concern in tropical and subtropical regions. Globally, it is estimated that 4.5–5.4 million snake bites occur each year, of which 1.8–2.7 million results in clinically evident envenomation, with an estimated mortality ranging from 81,000 to 138,000 annually. India has 52 species of venomous snakes and accounts for nearly 50% of the global deaths attributed to venomous snakebite. The incidence and pattern of snakebite vary across different geographical areas and are influenced by factors such as climate, ecology, biodiversity, snake distribution, and human population density. The present study included fatal snakebite cases subjected to medico-legal autopsy at the Department of Forensic Medicine and Toxicology, Patna Medical College, Patna. Information about demographic profile (age, sex, occupation, and socioeconomic status), geographical area, seasonal trends, site and pattern of bite, local tissue changes, and manner of bite was documented in a standardized proforma and analyzed accordingly. In this study, the majority of victims were males in the 21–30 year age group, predominantly engaged in agricultural work, and most bites were accidental in nature. Hands and feet were the most common sites affected. Most cases occurred during the rainy season. In the majority of victims, two fang marks were identified at the bite site, accompanied by subcutaneous hemorrhage, necrosis, swelling, and local cellulitis. Snakebite burden is highest among males aged 21–30 years, most of whom belong to economically weaker rural populations engaged in farming occupations.
Introduction
Although venomous snakes have been recognized in India since ancient times, the nation continues to face significant challenges in reducing mortality associated with snakebite envenomation. 1 In recognition of its major global health impact, snakebite was included in the World Health Organization (WHO) priority list of neglected tropical diseases in June 2017. Worldwide, more than 3,000 snake species have been identified; however, only around 250 are classified by the WHO as medically important due to the clinically significant toxicity of their venoms. 2 Snakebite represents a significant public health concern and medico-legal problem, particularly in tropical and subtropical regions of the world. Globally, it is estimated that 4.5–5.4 million people are bitten by snakes each year, of which approximately 1.8–2.7 million cases progress to clinically evident envenomation. The estimated global mortality attributed to snakebite ranges from 81,000 to 138,000 deaths annually. Regarding global variation in envenomation and snakebite mortality, the highest burden is observed in sub-Saharan Africa, South Asia, and South-East Asia. 3 In India, there are 52 species of venomous snakes, 4 of which 24 are considered as most important. 5 India is responsible for nearly 50% of the estimated worldwide mortality resulting from venomous snakebite envenomation. 6 As per the Registrar General’s Million Death Study, India reports nearly 50,000 snakebite deaths every year, whereas the global mortality estimate is about 125,000 deaths annually, of which more than 75,000 occur in Asia. 7
Incidence and frequency of snakebites vary in different geographic regions, depending on several factors such as climate, ecology, biodiversity, distribution of snakes, and human density. 8 Although snakebite is a frequent medical emergency, it predominantly affects rural communities, where individuals often initially seek treatment from local traditional healers rather than accessing formal healthcare facilities, thereby contributing to increased mortality. When the bite or subsequent signs of envenomation are not promptly recognized, victims may delay presenting to a healthcare provider. Snakebite-related mortality has been shown to correlate strongly with poverty, misidentification of the offending species, inappropriate management by untrained traditional practitioners, inadequate transportation and referral systems, delayed arrival at medical centers, and improper or suboptimal administration of anti-snake venom therapy. The present socio-demographic study was conducted on fatal snakebite envenomation cases subjected to medico-legal autopsy at Patna Medical College, Patna, Bihar, to illustrate the prevailing situation in the state. 9
Materials and Methods
This retrospective, hospital-based study was conducted on fatal snakebite victims who underwent medico-legal autopsy in the Department of Forensic Medicine and Toxicology, Patna Medical College, Patna, from July 2020 to November 2023, and included a total of 46 cases.
Inclusion Criteria
Only those hospitalized cases with a confirmed history of snakebite documented in the treatment records, along with corresponding systemic and local clinical findings consistent with snakebite envenomation, were included in the study.
Exclusion Criteria
Brought dead cases with a history of snakebite were excluded.
The details regarding age, sex, and residence were obtained from the inquest papers. Occupation, the circumstances of the bite (manner), area of occurrence of instances, socioeconomic status, identification of snake, time of snakebite, season, and pattern of local changes were gathered from treatment records retrieved from the Medical Record Department. During the autopsy, sites of bites and the pattern of bite marks on the body were noted.
The data were compiled into a structured proforma and analyzed using descriptive (mean, standard deviation) and inferential statistics (chi-square (χ2) test for association and p value). Statistical processing was carried out with Statistical Package for the Social Sciences (SPSS) Statistics version 31, and findings have been displayed using tables, graphs, and charts.
Observations and Results
A total of autopsies were conducted between July 2020 and November 2023; the hospitalized snakebite cases that proved fatal and were sent for autopsy were 46 (1.8%).
Gender
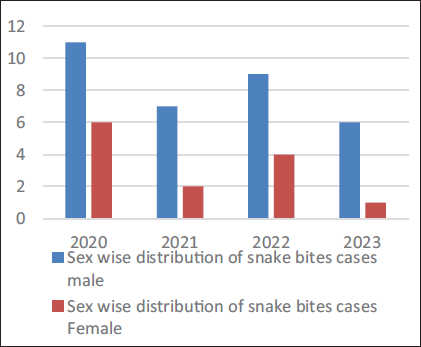
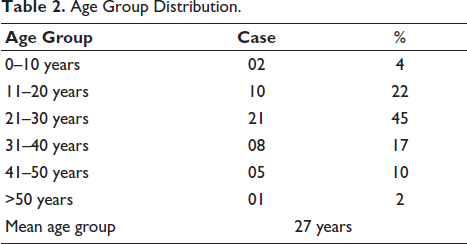
Out of 46 cases, 33 (72%) were male and 13 (28%) were female. The majority of the victims were male; the male-to-female ratio was 2.53:1. In 2022, there was a maximum fatal snakebite case. The mean of snakebite cases during these 3 years in males and females was 8.25 and 3.25, respectively. The χ2 test showed degrees of freedom, p ≈ .003, which was statistically highly significant that indicating less than 0.3% probability that the observed male–female difference occurred randomly (Table 1, Figure 1). This suggests that male predominance in snake bite cases is not due to random variation but likely reflects greater exposure risk. The mean age of snakebite victims in this study was approximately 27 years, indicating that young adults (21–30 years) were the most commonly affected age group, followed by 11–20 years in 10 (22%) cases, and the least was seen in the age group of more than 50 years in 1 (02%) cases (Table 2).
Sex-wise Distribution of Snakebite Cases.
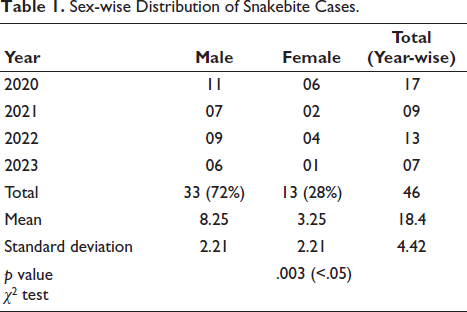
Sex-wise Distribution of Snakebite Cases.
Age Group Distribution.
Locality and Season
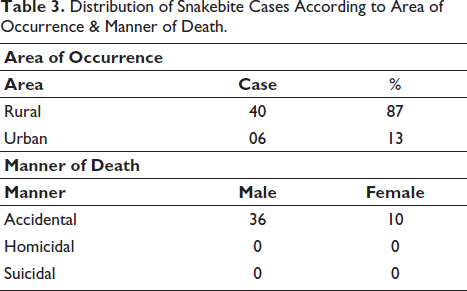
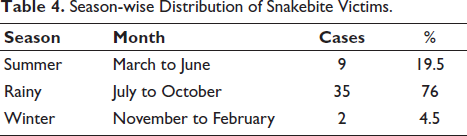
Forty (87%) were from rural areas and 6 (13%) were from urban areas, indicating that rural populations are at significantly higher risk (p < .001) (Table 3). The highest number of snakebite cases (76%) occurred during the rainy season (July–October), followed by summer (19.5%) and winter (4.5%). The predominance of cases during the monsoon period was statistically significant (p < .001) when compared to other seasons (Table 4).
Distribution of Snakebite Cases According to Area of Occurrence & Manner of Death.
Season-wise Distribution of Snakebite Victims.
Occupation
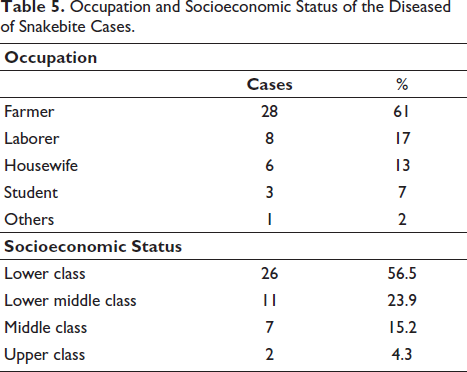
The majority of snakebite victims were farmers (61%), followed by laborers (17%), housewives (13%), and students (7%). The predominance of farmers indicates that individuals engaged in outdoor and agricultural activities were at a significantly higher risk (p < .001) of snakebites (Table 5).
Occupation and Socioeconomic Status of the Diseased of Snakebite Cases.
Socioeconomic Status
The snakebite victims mostly belonged to the lower socioeconomic class 26 (56.5%), followed by the lower middle class 11 (23.9%), middle class 7 (15.2%), and upper class 2 (4.3%). The relationship between lower socioeconomic status and higher snakebite incidence was statistically significant (p < .001) (Table 5).
Pattern of the Bite/Fang Marks
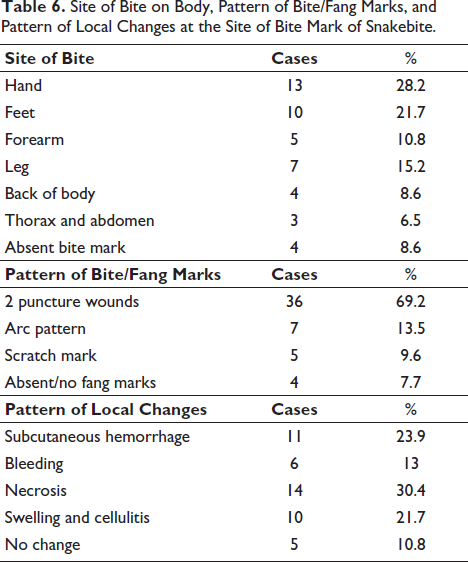
Out of various pattern of bite or fang marks of poisonous snake the most common, two pin point fang marks were present in 36 cases (69.2%), followed by arc pattern in 7 cases (13.5%), scratch mark in 5 cases (9.6%) and rare pattern of absent bite or fang marks in 4 (7.7%) (Table 6).
Site of Bite on Body, Pattern of Bite/Fang Marks, and Pattern of Local Changes at the Site of Bite Mark of Snakebite.
Site of Bite on Body
Most common bite marks were present over hands, 13 cases (28.2%), followed by feet, 10 cases (21.7%), forearm, 5 cases (10.8%), leg, 7 cases (15.2%), back of body, 4 cases (8.6%), thorax and abdomen, 3 cases (6.5%). In 8.6% of cases, bite marks were not identified (Table 6).
Pattern of Local Changes
Out of various local signs and symptoms after snakebite, necrosis was the most common in 14 cases (30.4%), followed by subcutaneous hemorrhage in 11 cases (23.9%), swelling and cellulitis in 10 cases (21.7%), and bleeding in 6 cases (13%). There were 5 cases (10.8%) in which no local changes were evident (Table 6). The overall site and local changes showed a statistically significant association with occupational exposure and outdoor activity (p < .001).
Manner of Death
All snakebite cases were accidental in nature. No homicidal or suicidal cases were observed. Among accidental deaths, males (78%) were more affected than females (22%) (Table 3).
Discussion
In the Indian medico-legal system, deaths resulting from snakebite are considered unnatural, and statutory regulations mandate that such cases must be subjected to medico-legal post-mortem examination. 10 In India, snakebite mortality has historically been predominantly linked to the “Big Four” species, namely the Russell’s viper, Indian cobra, saw-scaled viper, and common krait. 11 Venomous snakes are predominantly classified within the families Viperidae (vipers), Elapidae, Atractaspidae, and Colubridae. Among these, Colubridae represents the largest group, accounting for nearly 60% of all snake species. The Atractaspidae, which have more recently been grouped under the Viperidae family, include species adapted for burrowing and are characterized by the unique ability to protrude their fangs laterally without fully opening the mouth. 12 The snakes most commonly associated with human mortality in India are cobra (Najanajanaja), krait (Bungarus caeruleus), Russell’s viper (Viperarusselli), and saw-scaled viper (Echiscarinatus). 13 From a clinical perspective, venomous snakes are commonly grouped into hemotoxic types (vipers) and neurotoxic types (cobras and kraits). 14 Snake venom is a complex mixture predominantly composed of proteins and peptides, both enzymatic and non-enzymatic in nature, which collectively account for more than 90% of its dry weight. 15
Clinical manifestations of snakebite in humans vary considerably depending on the species involved, but in general consist of local pain, edema, blistering, and necrosis. Systemic effects of neurotoxic species include blurred vision, ptosis, and respiratory paralysis. Haemostatic toxins, such as the hemorrhagins, cause spontaneous bleeding in the gingival sulci, nose, skin, and gastrointestinal tract. Fatalities result from cerebral hemorrhage or massive retroperitoneal bleeding. Renal involvement in snakebite envenomation may present as glomerulopathy, vasculopathy, tubular necrosis, or interstitial nephritis, and is commonly associated with bites from both hemotoxic and neurotoxic species. Although identification of the offending snake can be valuable for guiding management in certain regions, it is often not feasible in routine clinical practice. 16 The outcome of a snakebite is influenced by multiple variables, such as the species involved, the anatomical site of the bite, the volume of venom delivered, and the individual’s underlying health status. In most cases—irrespective of whether the snake is venomous or non-venomous—some degree of local tissue reaction is usually observed. 17
Snake venom is an extremely complex mixture composed of proteins, peptides, non-protein toxins, lipids, carbohydrates, amines, and various other bioactive molecules. Its biochemical composition demonstrates considerable variability across different taxonomic levels. 18 Furthermore, venom composition may vary substantially among snakes from different geographical regions, and even among individuals within the same population. These biochemical differences may also be influenced by factors such as diet, age, season, and environmental conditions. To some extent, the wide spectrum of clinical manifestations observed following snakebite can be attributed to this complexity and variability in venom composition. 19
According to the WHO, snakebite is one of the most neglected tropical diseases and primarily affects the rural poor population. 20 In the present study, the male-to-female ratio was 2.53:1, indicating that males were more frequently affected, likely due to greater outdoor occupational exposure. This finding is consistent with previous studies reported from Madhya Pradesh, 21 Maharashtra, 22 and Karnataka. 23
Although fatal outcomes were observed across all age groups in the present study, the 21–30-year age group was most commonly affected. Similar findings have been reported in earlier studies, in which individuals between 21 and 50 years of age were identified as being at the greatest risk. 24 The marked reduction in fatalities beyond the age of 50 years is likely related to decreased involvement in agricultural activities among older individuals. An additional contributory factor may be reduced outdoor exposure during evening hours in this age group. 25
Globally, snakebite disproportionately affects populations residing in rural regions.3, 26, 27 In the present study, snakebite mortality was approximately 6.6 times higher in rural settings compared to urban areas. Previous literature has reported several contributors to this increased rural mortality, including poorly constructed housing, greater agricultural exposure, preference for traditional healers, and limited accessibility to timely anti-venom therapy. 28
Most human snakebites occur during the monsoon season because of flooding of the habitat of snakes and their prey. The breeding habits of frogs closely follow the monsoons, and rats and mice are always close to human dwellings. 29 The highest number of cases was recorded during July, August, September, and October, which coincides with the monsoon period in Bihar. In contrast, very few cases were observed during November, December, January, and February, likely due to reduced snake activity and relative hibernation during the winter season.
Hands (28.2%) were the most frequently affected site, followed by feet (21.27%), and this pattern aligns with findings from earlier research.29–31 This may be attributed to manual field work and barefoot farming during the monsoon season, where poor visibility and the likelihood of accidentally stepping on snakes—especially when fields are abundant with prey—increase the risk of bites. Harrison et al.9, 32 demonstrated a positive association between snakebite envenomation and poverty. In the present study as well, the lower socioeconomic group constituted the majority of victims (56.5%).
Snake poisoning is mostly accidental, 46 (100%); however, homicidal and suicidal snakebites are very rare. In ancient Egypt, snakebite was historically described as a method of execution, where victims were reportedly exposed to venomous snakes intentionally. Homicidal use of snakes has occasionally been documented in literature, wherein an agitated snake was directed toward a victim with harmful intent. However, such cases are extremely rare, and in the published record, only one documented instance exists in which an elderly couple was killed in an attempt to simulate accidental snakebite envenomation. 33 Few cases were reported to commit suicide by snake bite, namely Queen Cleopatra, 34 and others.35–39
Bleeding manifestations are frequently observed following bites by viperine species. 40 Local bleeding and swelling are primarily caused by the action of venom enzymes (proteases, phospholipases) and vasoactive toxins, which enhance vascular permeability. 41 Systemic bleeding occurs as a consequence of thrombocytopenia along with an associated defibrination syndrome. 42 Cerebral vascular involvement after snakebite is rare. In a study by Mosquera et al. 43 cerebrovascular complications were documented in 2.6% of 309 cases, predominantly hemorrhagic in nature, with ischemic events being infrequently observed.
Conclusion
Snakebite mainly affects male individuals of low socioeconomic status, particularly those residing in rural areas who are primarily engaged in farming activities. The 21–30 years age group is most challenged, whereas people above 50 years are less affected. Although snakebite incidence fluctuates throughout the year, the majority of cases occur during the rainy season. Public awareness initiatives are essential to encourage victims to seek immediate medical attention at hospitals rather than resorting to traditional healers, so that the crucial initial hours after envenomation can be appropriately utilized at tertiary care centers. Farmers should also be motivated to use protective gear during agricultural activities, and governmental agencies must ensure adequate safety measures for this high-risk group. There is a strong need for the formulation and implementation of a national program for snakebite prevention, focusing on improving quality of care, enhancing health education, providing financial support to reduce dependence on non-mechanized farming practices, and ensuring the implementation of WHO guidelines for snakebite management in the South-East Asia Region.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Not required (based on hospital and autopsy records).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.