
Abstract
Objective
To review the existing evidence to identify the optimum methods for implementing human papillomavirus self-sampling to increase screening uptake for underserved groups.
Setting
Specific groups are less likely to participate in cervical screening. These include individuals from low socioeconomic status groups, ethnic minority groups, younger age groups (25–29), older age groups (≥50), with a physical disability, with a learning disability and with an LGBTQ+ identity. The advent of human papillomavirus self-sampling for cervical screening presents an opportunity to promote equitable access to screening. Implementation for human papillomavirus self-sampling can vary, for example, opt-out or opt-in approaches. However, it is unclear which of these is the best method of offering human papillomavirus self-sampling to underserved groups.
Methods
Six databases were searched through May 2023. Studies comparing cervico-vaginal human papillomavirus self-sampling provision using different implementation strategies with the standard screening pathway in underserved groups were identified. A narrative synthesis was conducted.
Results
In total, 4574 studies were identified; 25 studies were included, of which 22 were from high-income countries. Greater uptake was found for offering human papillomavirus self-sampling compared to standard clinician-based sampling. Directly mailing human papillomavirus self-sampling kits to participants resulted in higher uptake of screening than using an ‘opt-in’ approach or standard recall in low socioeconomic status and ethnic minority groups, and older women. Strategies that used community health workers or educational materials increased uptake in ethnic minority and low socioeconomic status groups.
Conclusions
Directly mailing human papillomavirus self-sampling kits to low socioeconomic status groups, ethnic minority groups and older women has the potential to increase uptake of human papillomavirus self-sampling. Using community health workers to offer human papillomavirus self-sampling should be considered for ethnic minority and low socioeconomic status groups. Further research exploring the preferences of younger women is needed.
Introduction
Cervical cancer (CC) is the second most diagnosed cancer in women under 45 years old. 1 High-risk oncogenic subtypes of human papillomavirus (HPV16, HPV18) cause approximately 70% of CC cases.2,3 As a result of the link between HPV and CC, focus has turned to prevention of persistent HPV infection. 4 The UK has a successful HPV vaccination programme that is offered to 12–13-year-old girls (since 2008) and boys (since 2019). 5 The vaccination programme has been highly effective at reducing the incidence of pre-cancerous changes and CC. 6 This complements the National Health Service (NHS) cervical screening programmes (CSPs) which are offered at routine intervals to women between the ages of 25 and 64.7–10 As of 2024, all UK CSPs replaced cytology-based screening with primary HPV testing. 7 In England, cervical screening currently prevents 70% of CC deaths; however if all eligible individuals were engaged with regular screening, it is estimated that 83% of deaths could be prevented. 11 The introduction of vaginal self-sampling for cervical screening presents a new opportunity to increase screening uptake in the UK by promoting choice in sample collection method.12,13 However, although choice is generally seen as a positive step in patient activation, it is critical to understand the optimum way to implement self-sampling for all eligible individuals to ensure equitable access to screening choices.
High uptake of screening is associated with lower CC incidence and mortality,11,14 but participation in cervical screening in the UK has been steadily declining with coverage decreasing from 75.7% in 2011 to 70.2% in 2021. 15 There are a range of barriers that prevent uptake of cervical screening such as embarrassment and fear of the procedure, inconvenient appointment times, language barriers and gender-discordant sample takers.16,17
Specific groups of the population have been identified as less likely to engage with cervical screening than the rest of the population; these groups are commonly referred to as ‘underserved’ groups. These underserved groups have been identified as women from ethnic minority groups,18,19 members of the LGBTQ+ community, 20 lower socioeconomic status (SES) groups, 21 younger women (aged 25–29),22,23 older women (≥50) 23 and those with a learning disability 24 or physical disability. 25
Human papillomavirus self-sampling (HPVSS) has been identified as a method to overcome some of the barriers associated with clinician-based screening, thereby increasing uptake in non-attenders and reducing screening inequalities. 26 With self-sampling, the individual receives a sampling kit and takes their own cervico-vaginal sample. The sensitivity of these self-collected samples is comparable to that of clinician-collected samples.12,27 Self-sampling has been shown to be an acceptable method of screening to individuals represented in research26,28 and to increase screening uptake among underserved groups. 29 One UK study found offering non-attenders self-sampling generated a 2.25-fold higher participation rate than clinician-based sampling. 30
There are various implementation strategies for HPVSS. Those eligible for screening can be offered the option of ordering their own kits through a website, letter, email or telephone service, or by being given the kit at their general practitioner surgery or clinic. 31 These strategies are broadly known as the ‘opt-in’ approach – where women request their self-sampling kit. The other main strategy is the ‘opt-out’ approach, where self-sampling kits are mailed directly to all who are eligible, without participants having to request a kit. 31 There are benefits with the latter approach, because non-attenders are more likely to engage with screening, however it is a costly method and wastes unused kits. 32
This review builds on a recent meta-analysis, which found that directly mailed kits increased screening participation among non-attenders. 29 However, Yeh et al. did not examine the best ways of implementing HPVSS among underserved groups. 29 Different implementation approaches might be needed for different groups. The European Cancer Organisation has recommended that ‘self-sampling forms a central component of national cervical cancer screening programmes’. 33 Several countries, such as Australia (offering HPVSS in primary care) and Denmark, have already implemented self-sampling as part of their CSPs. 34 The UK plans to follow suit, with preliminary results from UK feasibility trials showing HPVSS can increase screening in non-attenders. 35 CSPs across the UK nations are in discussion about the possibility of implementing HPV self-sampling within their programmes. The aims of this review were (a) to identify the optimum implementation strategy(s) for HPVSS to increase uptake in different underserved groups, and (b) to understand the impact of HPVSS implementation strategies on acceptability of HPVSS in different underserved groups.
Methods
The review was registered on PROSPERO (CRD42023390276) and reported in line with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines. 36
Definitions
HPVSS was defined as the method of an individual collecting their own cervico-vaginal HPV sample (without use of a speculum). 37 This review did not include HPV urine sampling.
Underserved communities were defined as groups who have been identified as less likely to participate in cervical screening. These included those from low-SES groups, ethnic minority groups, younger women (≤29 years), older women (≥50 years), those with an LGBTQ+ identity, those with physical disabilities and those with learning disabilities. 19
The term ‘women’ has been used throughout this review to refer to all individuals who are eligible for cervical screening (i.e. people with a cervix). We note that this may include transmen and non-binary individuals.
Search strategy
Medline, Embase, Scopus, PsycINFO, Web of Science and CINAHL were searched through January 2023 using a combination of search terms for HPV, self-sampling and each underserved group. The search was updated in May 2023 and articles with publication date of 2023 were reviewed. The full search strategy is included in Appendix A.
Study eligibility
The inclusion and exclusion criteria are summarised in Table 1. No country or publication date restrictions were applied. Studies were not limited by design. Only studies that included a sub-group of participants from an underserved group identified above were included.
Inclusion and exclusion criteria.
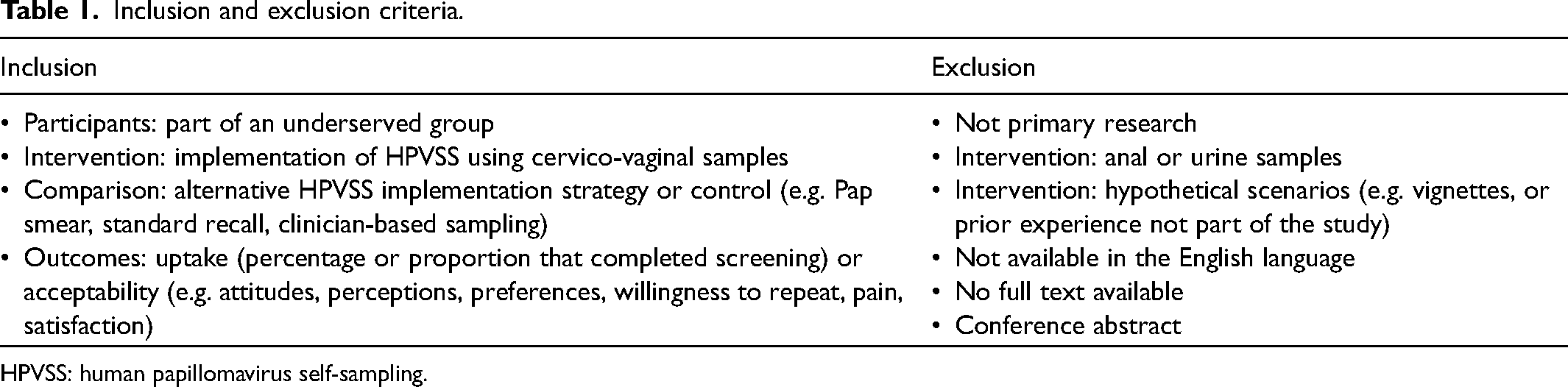
HPVSS: human papillomavirus self-sampling.
Data extraction and synthesis
Initial title and abstract screening was performed to identify relevant articles (OM). Articles were then screened at full text (OM). Twenty per cent of all articles were independently screened by a second reviewer (AK) at each stage. Discrepancies were resolved through discussion. Endnote reference managing software was used to manage exported papers.
Data extraction was completed by one reviewer (OM) using a piloted data extraction sheet (Appendix B) which included: authors, year, country, study design, study population, aims, screening interventions, outcomes measured and main findings. Due to the heterogeneity of the data, a narrative approach was used to synthesise the evidence. The synthesis was conducted using four stages of narrative synthesis: preliminary synthesis of studies, exploration of relationships in the data, theory development and the assessing robustness of the synthesis. 38
Assessing bias
One reviewer assessed the quality of the studies. The Cochrane Risk-of-Bias (RoB-2) tool was used to assess risk of bias in the randomised studies. 39 The Risk Of Bias In Non-randomised Studies – of Interventions (ROBINS-I) tool was used to assess risk of bias in the observational studies.40,41
Results
Study selection
Database searching retrieved 4574 articles (Figure 1). After de-duplication, 1582 citations were screened at the title-abstract level. Ninety-five full-text articles were screened; 24 articles were identified as meeting the eligibility criteria and 71 articles were excluded (reasons listed in Figure 1 and Appendix C). From the repeated search, 54 articles were screened and one relevant article was identified. Thus 25 articles were included in the review.
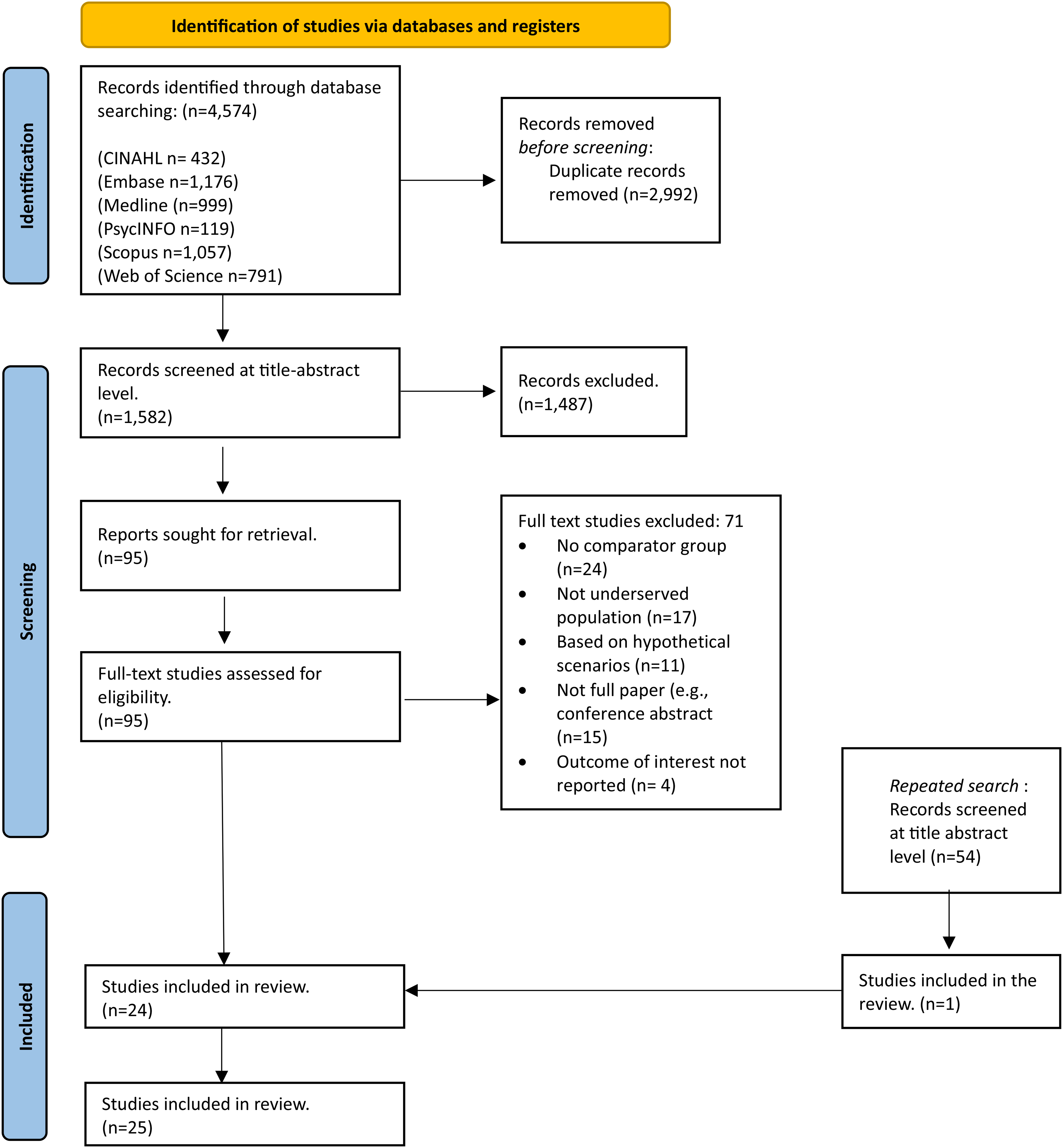
PRISMA flow diagram of study selection process.
Study characteristics
The study characteristics of the 25 studies are shown in Table 2. The studies have been grouped by underserved group. Fifteen of the studies were randomised controlled trials (RCTs) and nine were observational (four prospective cohort and five cross-sectional) studies. One study combined the data from two RCTs, 42 so the two original studies were appraised for their risk of bias.43,44 Articles were published between 2005 and 2023. There was a total of 132,039 participants aged between 25 and 70 across the studies. Sample sizes of the included studies ranges from 63 to 25,061. The included studies came from 13 countries (eight from the USA,45–52 four from the UK,53–56 two from New Zealand,57,58 two from Finland59,60 and one from each of the following countries: Australia, 61 Belgium, 62 Denmark, 63 France, 64 Hong Kong, 65 India, 66 Jamaica, 67 Mexico 68 and the Netherlands 42 ). Twenty-two studies were conducted in high-income countries. Nineteen studies only included ‘non-attenders’. The definition used to classify ‘non-attenders’ varied by study, therefore individual definitions have been included for each study (Table 2). No studies reported on people with an LGBTQ+ identity, physical disabilities or learning disabilities, and only one reported on younger women. 56 Comparators have been listed in Table 2 as study authors reported them (e.g. Pap smear, cytology-based). These screening methods are near identical in procedure; therefore the term clinician-based sampling has been used to refer to them in the synthesis.
Summary characteristics of included studies: comparing cervico-vaginal human papillomavirus self-sampling (HPVSS) provision using different implementation strategies with the standard screening pathway in underserved groups.
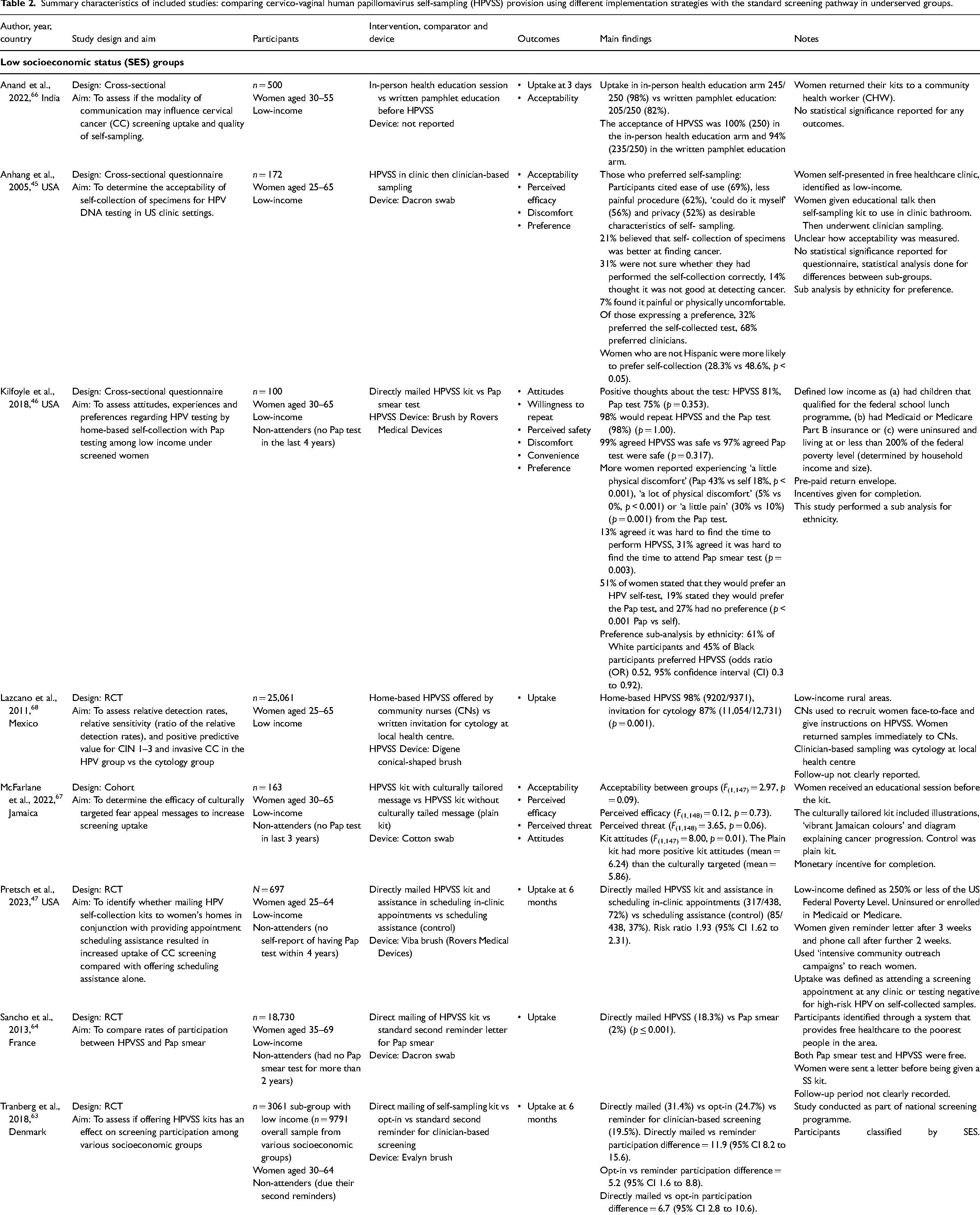
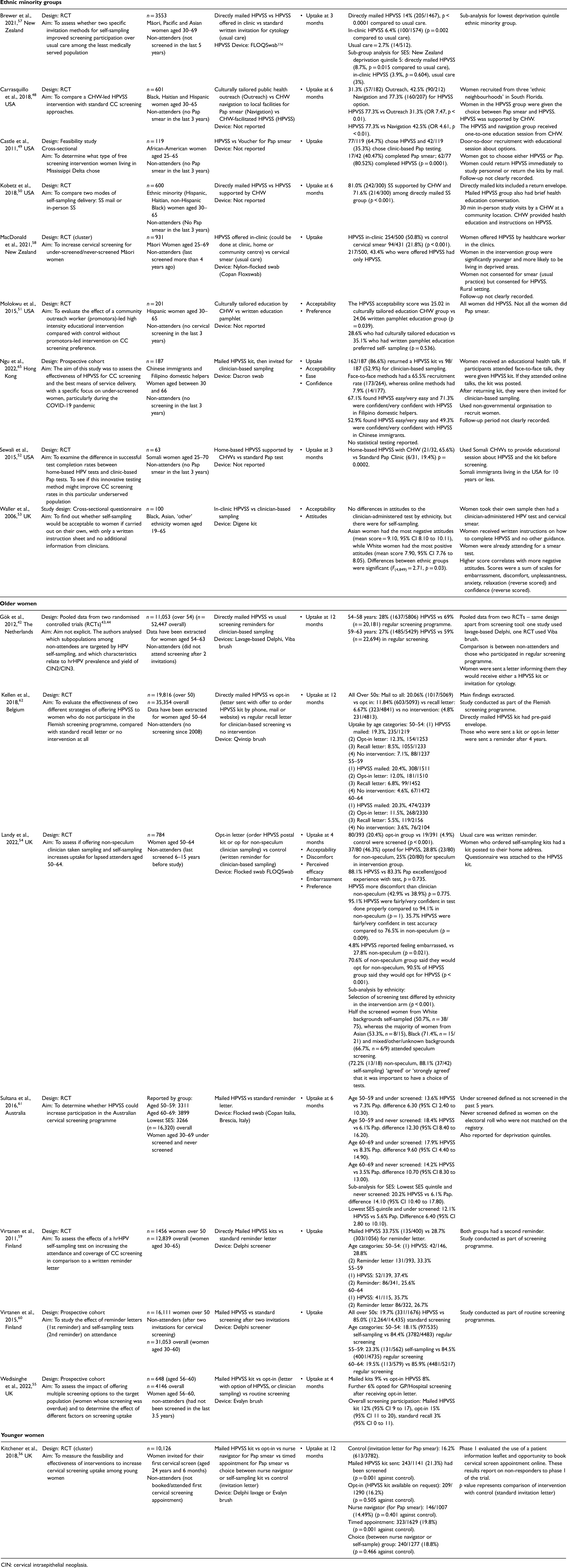
CIN: cervical intraepithelial neoplasia.
Quality assessment
The overall quality of the RCTs was high (Table 3). The majority of the concerns of bias in these studies were due to poor reporting of allocation concealment. Due to the nature of the intervention, participants were unable to be blinded. According to ROBINS-I, four studies were ‘moderate’, four studies were ‘serious’ and one study was ‘low’ risk of bias (Table 4). The results have been synthesised for each outcome and each underserved group.
Risk of bias in randomised controlled trials.
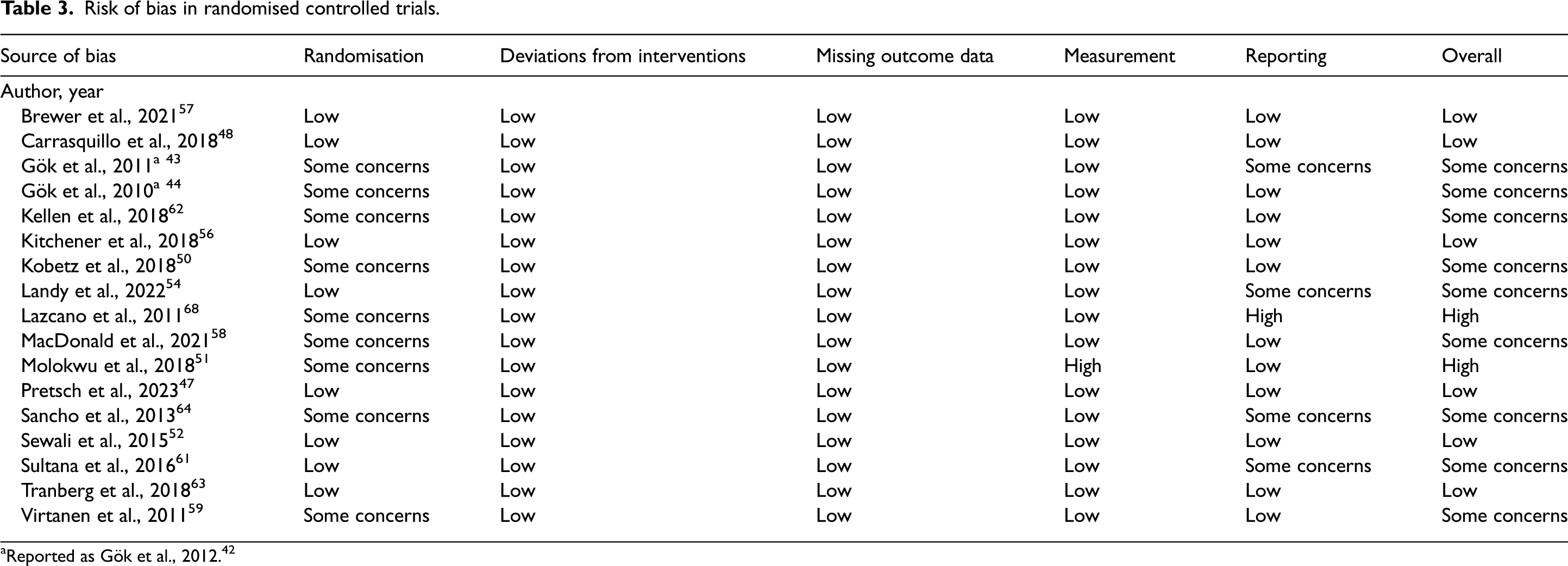
Reported as Gök et al., 2012. 42
Risk of bias in non-randomised studies.
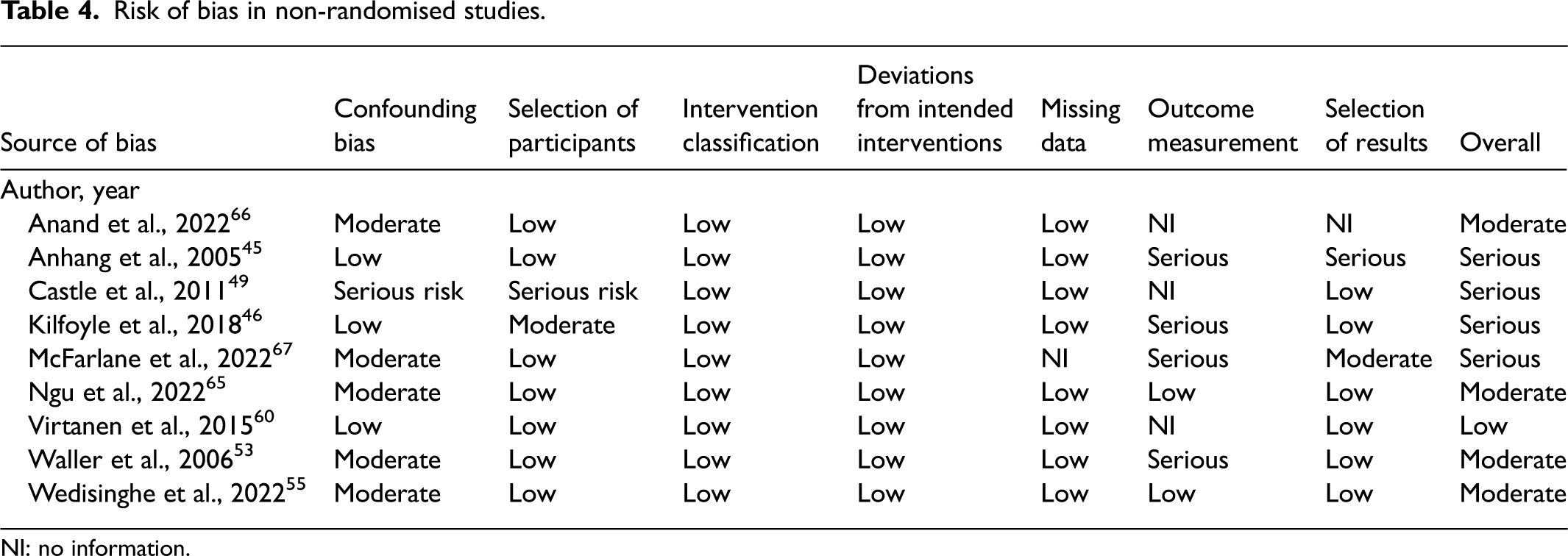
NI: no information.
Low socioeconomic groups
Ten studies reported on women from low-SES groups.45–47,57,61,63,64,66–68 Eight studies reported low-SES groups as their main population45–47,63,64,66–68 and two studies performed a sub-analysis for SES.57,61 The criteria for low SES varied across studies, but generally participants were identified based on income, accessing free healthcare or living in a deprived area.
Uptake
Four RCTs found mailing HPVSS kits to non-attenders increased uptake compared to a reminder for clinician-based screening: 31.4% vs 19.5%, 63 18.3% vs 2%, p < 0.001, 64 8.7% vs 3%, p = 0.0015 57 and 20.2% vs 6.1% for never-screened, 12.1% vs 5.6% for under-screened. 61 One of these RCTs found directly mailed kits resulted in higher uptake compared to an opt-in approach where women from low-SES groups were invited to order their own kits via website, email or phone: 31.4% vs 24.7%, participation difference = 6.7, 95% confidence interval (CI) 2.8 to 10.6. 63
One RCT found mailing HPVSS to low-SES women and offering assistance with scheduling in-clinic appointments increased uptake compared to scheduling assistance alone (72% vs 37%, relative risk 1.93, 95% CI 1.62 to 2.31). 47
Community nurses conducting home visits to offer HPVSS in an RCT resulted in significantly higher uptake than written invitations for clinician-based screening (98% vs 87%, p = 0.001). 68 However, the study was deemed to have a high risk of bias (Table 3); the analysis was ‘per-protocol’ and excluded women who were not at home during recruitment for HPVSS.
Anand et al. found uptake to be higher in a group that received an in-person health education session than a group that received written pamphlet education (98% vs 82%). 66
Acceptability
Two studies compared the acceptability of HPVSS with clinician-based sampling, both of which were deemed to have serious risk of bias (Table 4).45,46 Kilfoyle et al. mailed HPVSS kits directly to low-income women. 46 There was no significant difference between HPVSS and clinician-based sampling groups on attitudes towards test (81% vs 75%, p = 0.353), willingness to repeat (98% vs 98%, p = 1.00) or perceived safety of the test (99% vs 97%, p = 0.317). 46 However, pain and discomfort were higher for clinician-based sampling (43% vs 18%, p < 0.001 and 30% vs 8%, p = 0.001, respectively). HPVSS was more convenient (13% vs 31%, p = 0.003) and more women expressed a preference for HPVSS than clinician-based sampling (51% vs 19%, p < 0.0001). 46 Anhang et al. offered HPVSS in-clinic along with clinician-based sampling. 45 Having had both tests, of the women who indicated a preference, more preferred clinician-based sampling than HPVSS (68% vs 32%) but no statistical test was reported. 45
Two observational studies reported on the acceptability of HPVSS when given different supporting materials for HPVSS for low-SES women.66,67 Anand et al. found that an in-person health education session compared to a leaflet resulted in HPVSS being reported as more acceptable (100% vs 94%) and produced a greater uptake rate (98% vs 92%) of HPVSS, although there was no p-value stated. 66 McFarlane et al. found there was no difference in the acceptability or perceived efficacy of HPVSS between using a culturally tailored kit (which included illustrations and colours designed to appeal to Jamaican women), compared to a ‘plain’ kit (p = 0.09). 67 However, the ‘plain’ kit received more positive attitudes than the kit which was culturally targeted (M = 6.24 vs 5.86) (Table 2). 67
Women from minority ethnic backgrounds
Nine studies were conducted among minority ethnic groups.
Uptake
Seven studies looked at uptake in ethnic minority groups. Two RCTs found that offering HPVSS in a clinic to Māori women 58 or Māori, Pacific and Asian women 57 in New Zealand resulted in greater uptake compared to offering clinician-based sampling: 6.4% vs 2.7%, p = 0.002 57 and 50.8% vs 21.8%, p < 0.001. 58 MacDonald et al. offered women HPVSS in a clinic; however, women were also allowed to complete the test at home. 58 One of these studies found higher uptake for the group mailed HPVSS kits compared to those given a written invitation to clinician-based sampling (14% vs 2.7%, p < 0.0001). 57
Three RCTs evaluated the use of HPVSS supported by a community health worker (CHW) among Black, Haitian and Hispanic women48,50 and Somali women 52 in the USA. The uptake of HPVSS supported by a CHW was significantly higher than mailing HPVSS kits (81.0% vs 71.6%, p < 0.001) 50 or offering clinician-based sampling (65.6% vs 19.4%, p = 0.002). 52 HPVSS supported by CHWs also resulted in higher uptake compared with using nurse navigators for clinician-based sampling (77.3% vs 42.5%, p < 0.001) or an educational outreach session (77.3% vs 31.3%, p < 0.01). 48
One study set in the USA found that after being given the choice between HPVSS or clinician-based sampling, African-American women were more likely to complete screening using home-based HPVSS than clinician-based sampling (80.5% vs 40.5%, p = 0.0001). 49 This study was deemed to have serious risk of bias (Table 4).
Ngu et al. found mailing HPVSS kits to Chinese immigrants and Filipino domestic helpers in Hong Kong after an education session had higher uptake compared to offering clinician-based sampling (86.6% vs 52.9%). Recruitment of women was greater using face-to-face recruitment compared to online methods (65.5% vs 7.9%); no p-value was reported. 65
Acceptability
A culturally tailored educational intervention for Hispanic women in the USA resulted in higher acceptability of HPVSS compared to an educational leaflet (acceptability score 25.02 vs 24.06, p = 0.039) but there was no effect on preference between self-sampling and clinician-collected sampling (28.6% vs 35.1%, p = 0.536). 51 This study was deemed to have high risk of bias due to the varying measurement of acceptability (Table 3).
Four studies reported differences between ethnic groups as sub-analysis.45,46,53,54 Women who were not Hispanic were more likely to prefer HPVSS than clinician sampling, than those women who were Hispanic (48.6% vs 28.5%, p < 0.05). 45 Kilfoyle et al. reported that Black women and women other than White were less likely than White women to prefer HPVSS over clinician-based sampling (odds ratio 0.52, 95% CI 0.30 to 0.92). 46 Landy et al. reported that half of the screened White women selected HPVSS (50.7%); however women from Black (71.4%), Asian (53.3%) and mixed/other/unknown backgrounds (66.7%) were more likely to choose clinician-based sampling (p < 0.001). 54 Furthermore, a UK study reported that Asian women had negative attitudes towards self-sampling but White women had more positive attitudes (mean score 9.10 vs 7.90, p = 0.03). 53
Younger women
Only one relevant study was identified which included younger women (aged 25) and it examined uptake 56 of initial screening invitations; no studies reported on acceptability of HPVSS for younger women. Therefore the results presented here cannot be generalised to young women.
Uptake
Kitchener et al. conducted an RCT in the UK and reported greater uptake for mailing HPVSS kits (21.3%) and timed appointments for clinician-based sampling (19.8%) compared with standard written reminder letters (16.2%; p = 0.001 and p = 0.01, respectively). 56 The opt-in approach for HPVSS resulted in an equivalent uptake rate to standard written reminders (16.2% vs 16.2%, p = 0.505). 56
Older women
Seven studies were conducted among older women.
Uptake
Seven studies reported on the uptake of HPVSS among older women (≥50 years).42,54,55,59–62 One of these exclusively included older women. 54 The other six studies stratified results by age; therefore data could be extracted from results tables in the studies, but significance testing using p-values was not reported for these.42,55,59–62
Three studies found that directly mailed kits had higher uptake than standard recall for clinician-based sampling59,61,62 (Table 2). Two studies found directly mailed kits had higher uptake than using an opt-in approach.55,62 The opt-in approach in one of these studies included both clinician sampling and HPVSS. 55 Two further studies found mailed HPVSS kits generated additional uptake in non-attenders who did not engage with clinician-based screening after two invitations (Table 2).42,60 The statistical significance of these results were not reported.
An opt-in approach resulted in higher uptake than standard recall: 20.4% vs 4.9%, p < 0.001 54 and 15% vs 3%. 55 The opt-in approach in both studies included the option of HPVSS or standard clinician sampling; thus the uptake for opt-in was not exclusively for HPVSS.
Acceptability
There was no significant difference in the acceptability, perceived efficacy or discomfort associated with HPVSS compared to clinician-based sampling (Table 2). 54 However, HPVSS was less embarrassing (4.8% vs 27.8%, p = 0.021) and was preferred to clinician-based sampling (90.5% vs 70.6%, p < 0.001). 54 Women had less confidence in HPVSS accuracy (35.7% vs 76.5%, p = 0.009). Women from both groups (offered self-sampling and clinician-based sampling) agreed it was important to have a choice about sampling options (Table 2). 54
Discussion
Overall, opt-out methods, such as directly mailing HPVSS kits and using CHWs to offer HPVSS, resulted in higher uptake of cervical screening compared to opt-in strategies for HPVSS or offering clinician-based sampling among most women. This review has shown higher uptake when offering underserved groups the option of HPVSS compared to clinician-based sampling. Although not as effective as the opt-out strategies, offering women the choice to opt-in for HPVSS still resulted in higher uptake than clinician-based sampling, particularly for some underserved groups. Although overall HPVSS was acceptable for underserved groups, differences were observed in the acceptability and preferences of screening modality between different ethnic groups. There was some variation in HPVSS acceptability based on how it was implemented (opt in/opt out), but the evidence was limited.
What is optimal: opt-in or opt-out
In relation to opt-out strategies, directly mailing HPVSS kits resulted in significantly higher uptake of HPVSS in low-SES groups, ethnic minority groups and younger women compared with an invitation or reminder for clinician-based sampling.56,57,64 This finding aligns with a recent meta-analysis showing a two-fold increase in screening uptake when HPVSS kits were mailed directly to women, as opposed to inviting them to clinician-based screening. 29 Mailing kits has been found to increase screening uptake in both non-attenders and the general population.29,69 This review builds on this evidence by confirming that directly mailing kits improves uptake in a range of underserved groups. Directly mailing kits can mitigate barriers such as accessing kits, embarrassment and inconvenience of in-clinic sampling. 31 The levels of uptake seen with directly mailed kits were higher than the uptake achieved by an opt-in approach and offer of clinician sampling.56,57
Although not as effective as the opt-out strategies, offering women the choice to opt-in for HPVSS still resulted in higher uptake than clinician-based sampling particularly for individuals who were older 54 and those from low-SES backgrounds. 63 In older women there was significantly greater uptake for an opt-in approach for HPVSS or non-speculum clinician sampling compared to clinician-based sampling. 54 This contrasts with results from Arbyn et al. who found opt-in approaches to not significantly increase uptake compared to routine invitations for clinician-based sampling. 12 However, there was a lack of literature focusing on young women. Only one study was identified and it focused on attendance to first screening invite in the UK. It found no difference between an opt-in approach for HPVSS and clinician-based sampling. 56 It is important that further research focusing on young women is to be conducted to explore preference for opt-in/opt-out choice of HPVSS.
Further strategies
As well as offering HPVSS, further strategies to increase uptake were explored in some studies, in particular those focusing on women from lower SES and ethnic minority backgrounds. A variety of alternative strategies were used, such as CHWs, an in-clinic HPVSS option and educational materials. All studies that reported on CHWs found significantly higher uptake compared to alternative strategies among ethnic minority and low-SES groups.48,50,52,68 Kobetz et al. found significantly higher uptake for HPVSS supported by a CHW than directly mailed kits. 50 Two studies found significantly higher uptake for an in-clinic HPVSS option compared to clinician-based sampling in ethnic minority women.57,58 One of these studies offered in-clinic HPVSS for women to do either in clinic or at home. 58
HPVSS modality acceptability
HPVSS was acceptable for underserved groups. However, differences were observed in the acceptability and preferences of screening modality between different ethnic groups. Hispanic women and Black women were less likely to prefer self-sampling to clinician-based sampling compared to White women.45,46 Black, Asian and women of other ethnic backgrounds were more likely to opt for clinician-collected samples than White women. 54 The cultural appropriateness and perceived lack of reliability of self-collected samples have been identified as barriers for uptake among ethnic minority women. 70 Three of the four studies reporting on CHWs in ethnic minority groups invited women to an education session pre-testing.48,50,52
Cultural tailoring improved acceptability of HPVSS in a group of Hispanic women 51 whereas no difference was found in a group of Jamaican women 67 from low-income backgrounds. The study which showed a significant difference was at high risk of bias, thus questioning confidence in the finding. 51 In another study higher levels of HPVSS acceptability were suggested for an in-person health education session compared with written education for women from a low-income setting (statistical significance not reported). 66
Recommendations for introduction of HPVSS modality
In addition to the modality of offering HPVSS, this review suggests that access to support from healthcare professionals (HCPs) and education about screening are important components for ensuring that implementation of HPVSS is planned in a manner that will aid equitable access to cervical screening. A previous review found the home to be a highly acceptable setting for HPVSS, but women were found to prefer clinic-based sampling if sampling in the home meant they would not have access to an HCP. 26 Using CHWs combines the benefits of home-based self-sampling with the support and reassurance offered by a trusted professional. CHWs are uniquely placed to reassure the women of their communities. Face-to-face interaction and education provided by CHWs is likely to alleviate concerns women have about self-sampling, such as lack of confidence in completing the kit. 70 Careful identification of suitable communities is necessary for implementing this approach in large-scale CSPs. High cost implications and practical considerations need to be evaluated within the NHS setting. CSPs might be most suitable for targeted interventions, such as CHWs, where particularly low levels of screening uptake within certain communities are identified.
Strengths of this research
We applied a critical lens to understanding what works best and for which individuals when planning the introduction of HPVSS into CSPs. The UK has recently trialled the use of HPVSS for increasing cervical screening among non-attenders as well as an option to complete a screening in clinic. 35 The findings from this study can directly inform plans for introduction of HPVSS in the UK and in other nations with an organised screening programme.
Most studies within this review were RCTs (with low or some concerns about bias). All studies reporting significance between implementation strategies were RCTs, most of which were high quality and well reported (Table 3). Studies reporting the acceptability of HPVSS based on hypothetical scenarios were excluded; therefore the findings reflect the views of participants who were actually offered screening (HPVSS or clinician sampling). Given the multifaceted and complex nature of implementation strategies within the included studies, a narrative synthesis was used to provide a comprehensive knowledge summary to understand how HPVSS implementation strategies work in different contexts, for different groups. This review is unique as it has looked at which underserved groups might benefit most from HPVSS and the best methods for implementing HPVSS to achieve maximum benefit.
Limitations
It is important to note that not all underserved groups were represented in this review and therefore findings cannot be assumed as applicable; no studies were identified that reported on LGBTQ+ groups, or women with physical disabilities or learning disabilities. Furthermore, only one study reported on younger women, and thus our results cannot be applied to young women broadly. Results focusing on older women were mostly extracted by sub-group data from studies looking at the general population, and the statistical significance of these findings was not reported in the individual studies. This limits the strength of our conclusions for the group of older women. Several other studies did not report significance testing. In their raw form, such results provide some insight into the effectiveness of implementation strategies; however the strength of conclusions that can be drawn from these studies is greatly limited.
There was limited evidence for the secondary objective of this review (to understand the impact of implementation strategies on acceptability of HPVSS) with only three studies examining the impact of different strategies for implementing HPVSS on acceptability.51,66,67
Many of the other studies compared HPVSS acceptability with clinician-based sampling acceptability. Further research is needed to explore whether and how implementation strategies can influence HPVSS acceptability.
Recommendations
The optimum implementation strategies for each group are summarised in Table 5.
Summary of key findings for each group.
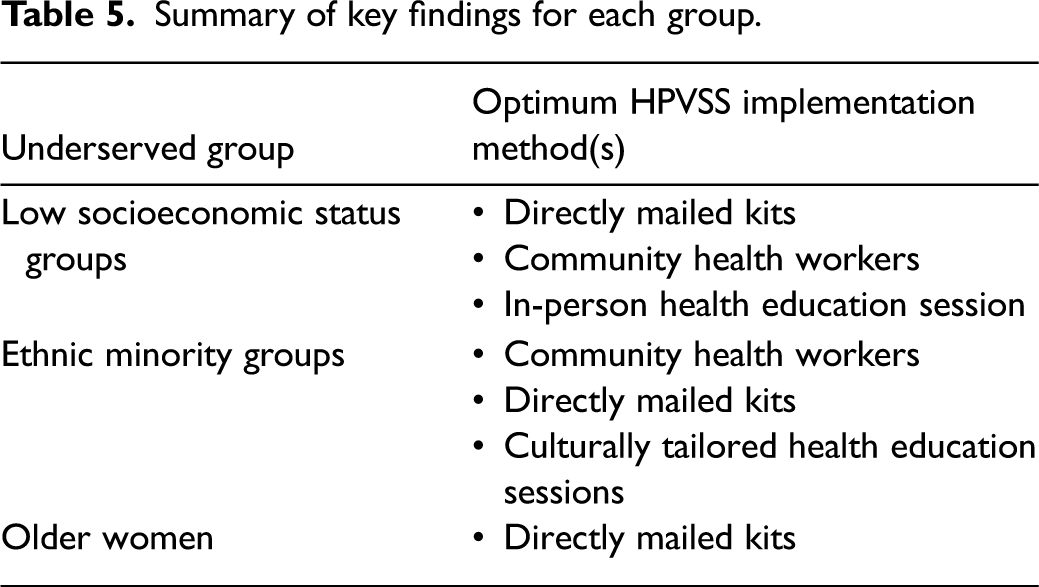
Directly mailing HPVSS kits as part of the UK CSP should be considered for reaching underserved groups. Examination of appropriate supporting materials and health education promotion components to include with directly mailed kits is important to optimise uptake.
As seen by the success of CHWs, the face-to-face engagement of women from underserved groups remains important. Ensuring women have access to HCPs and are well supported is important for the implementation of HPVSS.
Although inferior to directly mailing kits, offering HPVSS in clinic and opt-in approaches should not be dismissed. Several studies observed an increase in uptake using opt-in approaches compared to standard screening pathways. This increase was seen in younger women (although only one study), women from ethnic minority backgrounds, older women and low-SES group (one study). Opt-in and in-clinic strategies are more economical when considering implementation on a national level. 31
It is essential to consider the needs of underserved groups to minimise screening inequalities and to promote uptake. 71 Given the paucity of evidence for some underserved identified by this review, future work should examine the implementation of HPVSS among those with LGBTQ+ identities, learning disabilities, physical disabilities and among younger women.
Conclusion
To facilitate an equitable and person-centred approach to HPVSS implementation, the offer of opt-out HPVSS methods (e.g. directly mailing HPVSS kits) should be considered a priority as it has the potential to increase uptake of cervical screening in underserved groups. Screening uptake may further improve in women from low-SES and ethnic minority background groups when CHWs are used within HPVSS implementation.
Supplemental Material
sj-docx-1-msc-10.1177_09691413241274312 - Supplemental material for Identifying optimum implementation for human papillomavirus self-sampling in underserved communities: A systematic review
Supplemental material, sj-docx-1-msc-10.1177_09691413241274312 for Identifying optimum implementation for human papillomavirus self-sampling in underserved communities: A systematic review by Olivia Mackay, Kate Joanna Lifford, Anahat Kalra and Denitza Williams in Journal of Medical Screening
Supplemental Material
sj-docx-2-msc-10.1177_09691413241274312 - Supplemental material for Identifying optimum implementation for human papillomavirus self-sampling in underserved communities: A systematic review
Supplemental material, sj-docx-2-msc-10.1177_09691413241274312 for Identifying optimum implementation for human papillomavirus self-sampling in underserved communities: A systematic review by Olivia Mackay, Kate Joanna Lifford, Anahat Kalra and Denitza Williams in Journal of Medical Screening
Supplemental Material
sj-docx-3-msc-10.1177_09691413241274312 - Supplemental material for Identifying optimum implementation for human papillomavirus self-sampling in underserved communities: A systematic review
Supplemental material, sj-docx-3-msc-10.1177_09691413241274312 for Identifying optimum implementation for human papillomavirus self-sampling in underserved communities: A systematic review by Olivia Mackay, Kate Joanna Lifford, Anahat Kalra and Denitza Williams in Journal of Medical Screening
Footnotes
Acknowledgement
The authors thank subject librarian Delyth Morris for assisting with the search strategy.
Data availability statement
Data sharing is not applicable to this article as no new data were created or analysed in this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.