
Abstract
Objective
Cervical cancer screening participation in China remains insufficient, possibly because of embarrassment or discomfort. We assessed knowledge of HPV and its link to cervical cancer, and whether HPV self-sampling might be an acceptable alternative to clinician-based screening, among Sichuan women.
Methods
A sample of healthy women undergoing routine physical examinations in 2017 at the West China Hospital, Sichuan University, completed a questionnaire.
Results
From 3000 questionnaires distributed, 1810 were completed and analyzed. Only 29.94% of respondents (n = 542) had heard of HPV, among whom 65.75% knew that it caused cervical cancer. Among the 766 (42.32%) who considered that HPV self-sampling for cervical cancer screening was an acceptable option, over 90% thought it would be convenient, private, not embarrassing, and not painful. However, 1044 women (57.68%) did not consider self-sampling acceptable, mainly because the result might not be accurate (85.63%), specimens may have gone bad (83.05%), and they may not perform the test correctly (79.98%). Respondents who believed HPV self-sampling was acceptable were more likely than other respondents to be young, and to have completed at least secondary education. Of the 1810 respondents, 1312 (72.49%) reported that they would be willing to be vaccinated against HPV.
Conclusion
Most women in Chengdu lack basic knowledge about HPV. Over 40% of women believed HPV self-sampling for cervical cancer screening was an acceptable option. To increase screening coverage, public health efforts to educate the public about HPV and HPV self-sampling for cervical cancer screening should be strengthened and expanded.
Introduction
Cervical cancer is the second most common cancer in women aged 15–45 in China, with 130,000 new cases diagnosed annually. 1 Cervical screening programs have substantially reduced cervical cancer incidence and mortality in many developed countries.2–4 In 2009, China launched a free cytology cervical cancer screening program to cover 10 million women living in rural areas until 2011, but there are around 350 million women of childbearing age in China. Although cervical cytology and human papillomavirus (HPV) testing have been used in clinical practice for several years, China has a vast territory, uneven development in various regions, and a lack of appropriate technical personnel or equipment. Women lack knowledge of cervical cancer prevention and treatment, and have a low awareness of active screening. Even when medical resources are available, some women do not attend cervical cancer screening due to embarrassment or discomfort during gynaecological examination, or practical factors such as time, cost, and access to screening facilities or a female practitioner.5,6 In 2010, the cervical cancer screening rate in China was about 21% (29.1% in urban areas and 16.9% in rural areas). 7
Most cervical cancer is caused by high-risk human papillomavirus (HR-HPV) infection,8–10 and current clinical guidelines recommend screening women aged 30 and older using a DNA-based HPV test. HR-HPV self-sampling allows women to take their test using a brush in a comfortable and convenient place by themselves, without the help of doctor. Self-sampling can save time travelling to and from the hospital, and also alleviates the difficulty for patients in seeking medical treatment. HPV self-sampling therefore has great potential to improve coverage and participation in cervical cancer screening in China. Key barriers to participation could also be addressed by overcoming disparities in HPV-related knowledge and perceptions about cervical cancer screening. 11 A systematic review of studies from several countries suggests that only 15–31% of respondents, regardless of age, have even heard of HPV, while only 0.6–11% know that HPV is a risk factor for cervical cancer. 12 The HPV vaccine, though very expensive, is now available in Chengdu, and medical centres are tasked with educating men and women about HPV, but it is unclear how much knowledge the general population has about HPV and its link to cervical cancer.
It is not known whether self-sampling is viewed as an acceptable screening option among women in Sichuan. Knowledge about HPV may strongly influence the acceptability of HPV self-sampling. In this study, we therefore aim to assess knowledge about HPV and its link to cervical cancer, and attitudes towards HPV self-sampling as an alternative to traditional clinician-based screening, among women in Chengdu. We analyse the relationship between sociodemographic characteristics and women’s attitudes to self-sampling and investigate the reasons why women consider self-sampling to be an acceptable or unacceptable option for cervical screening.
Methods
Healthy women undergoing routine physical examinations in the Health Management Center of West China Hospital of Sichuan University between January and December 2017 were invited to take a single survey. They completed a paper-based questionnaire, which they then returned to staff (a method used in our previous study 13 ). We excluded women older than 75, and women with a history of cervical cancer. Included women were able to read and understand the questionnaire, either on their own or with the help of staff. The target study population was 2500 women, which assumed that a 75% response rate should provide a sample adequate to estimate proportions for which the 95% confidence interval would have a maximum width of 10%. This corresponds to a maximum error of ±5% for all estimates of proportions. 13 All participants provided written informed consent to participate in our study
A self-administered questionnaire based on the literature11–14 was designed specifically for this study. The questionnaire included outcome variables and correlate variables, and the number of questions was strictly limited to reduce bias due to cognitive boredom and fatigue. Because the Chinese name of HPV includes the word “papilla,” a statement that HPV has no relationship to breast cancer was inserted into the questionnaire, in order to avoid confusion. The questionnaire was piloted with a group of 30 women not included in the final study population. The survey was given to participants together with a covering letter explaining its purpose.
Questions 1 and 2 on the survey were used to assess HPV knowledge. Surveys on which the response to question 1 was “no” were excluded from the analysis of responses to question 2. Questions 3–5 were used to assess the acceptability of HPV self-sampling, and the reasons for women considering it to be an acceptable or unacceptable option. In addition to the above questions, sociodemographic characteristics, such as age, ethnicity, educational background, Pap testing experience, and family history of cancer were also included in the survey. All questionnaires were completed anonymously, to ensure confidentiality.
Data were managed in EXCEL and analysed using SPSS 17.0 (IBM, Chicago, IL). Descriptive statistics were used to evaluate knowledge about HPV infection and self-sampling acceptability. Responses of “don’t know” were re-coded as “no” in the statistical analyses. Associations between respondent characteristics and level of knowledge or self-sampling acceptability were explored in univariate analysis using the Chi-squared test. Factors in the univariate analysis for which the associated p < 0.05 were then used in multivariate logistic regression.
This study received ethics approval and consent from the Ethics Committee, Sichuan University, committee reference number 2016(207).
Results
From 3000 questionnaires distributed, 1972 (65.73%) were returned. Of these, 162 were excluded because they were incomplete. The remaining 1810 questionnaires were used in the final analysis.
The sociodemographic characteristics of the participants are shown in Table 1. The mean age was 38.52 ±8.82, and nearly all respondents (93.0%, 1683/1810) were Han Chinese. Of the 1810 respondents, 62.7% (1134) had at least a bachelor’s degree, 28% (507) reported never having undergone a Pap test, 37.0% (670) had undergone Pap testing inconsistently, and 35.0% (633) had undergone regular Pap testing.
HPV knowledge and acceptability of HPV self-sampling among respondents.
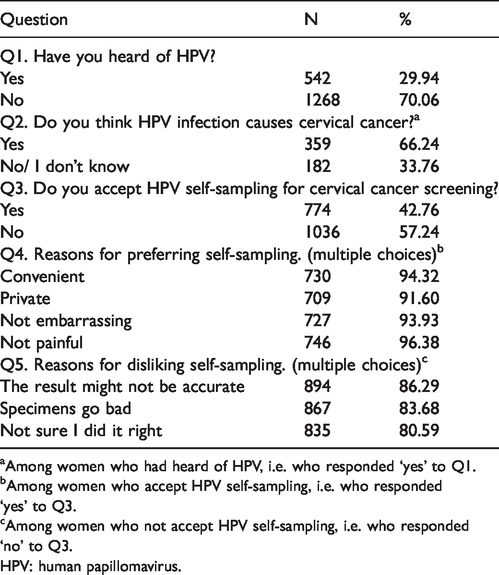
aAmong women who had heard of HPV, i.e. who responded ‘yes’ to Q1.
bAmong women who accept HPV self-sampling, i.e. who responded ‘yes’ to Q3.
cAmong women who not accept HPV self-sampling, i.e. who responded ‘no’ to Q3.
HPV: human papillomavirus.
Only 29.94% (542/1810) of respondents had ever heard of HPV, and among this subgroup, 66.24% (359/542) knew that HPV causes cervical cancer (see Table 2). Univariate analysis showed that women who had heard of HPV were more likely to be aged 18–65, to be Han Chinese, to have a strong educational background, to have a family history of cervical cancer, and to have undergone Pap testing at least once. The odds ratios and 95% confidence intervals (CI) from the multivariate models are shown in Table 3. The following factors remained positively associated: educational background of Bachelor or above, family history of cervical cancer, and ever having undergone Pap testing.
Demographic characteristics of respondents (n = 1810) and univariate analysis of HPV knowledge and acceptability of HPV self-sampling.
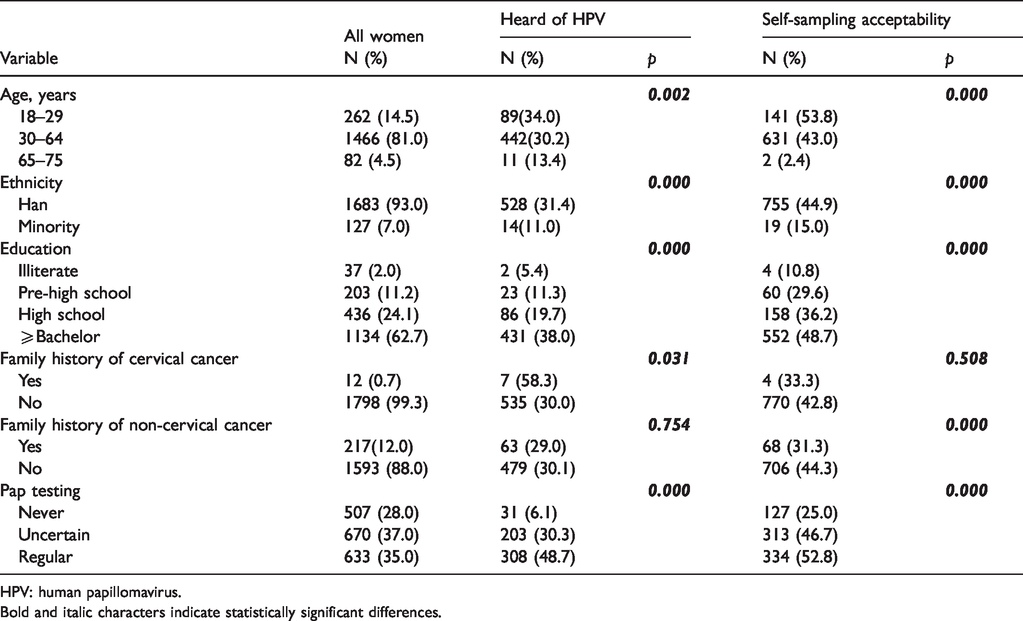
HPV: human papillomavirus.Bold and italic characters indicate statistically significant differences.
Multivariate logistic regression to identify factors associated with HPV knowledge and acceptability of HPV self-sampling.
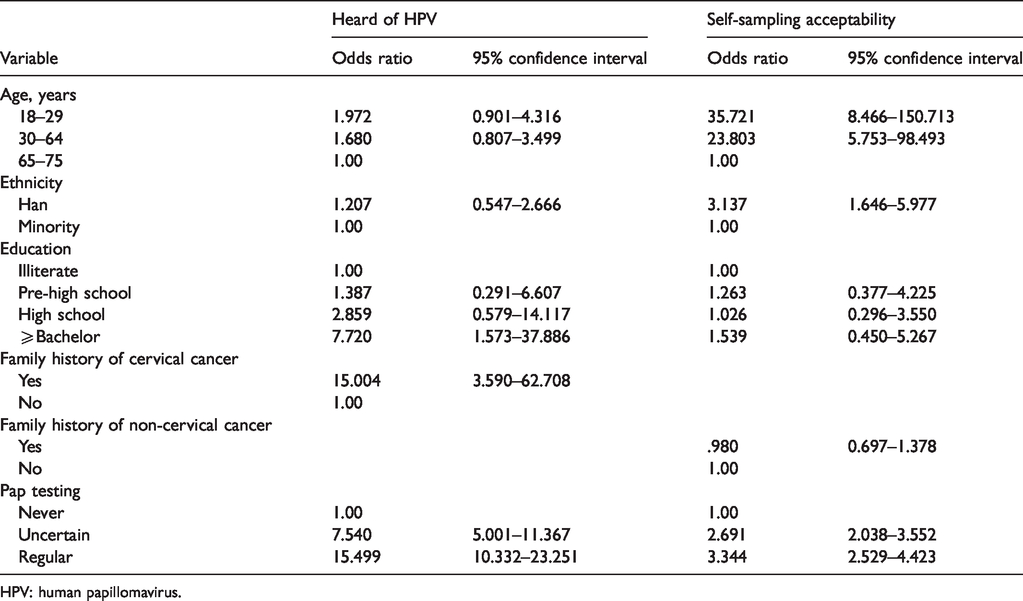
HPV: human papillomavirus.
Among all respondents, including those who had heard of HPV and those who had not, 42.76% (774/1810) felt that HPV self-sampling for cervical cancer screening was an acceptable option (see Table 1). Univariate analysis (Table 2) showed that these women were more likely to be aged 18–65, to have a strong educational background, to have a family history of non-cervical cancer, and to have undergone Pap testing at least once. The odds ratios and 95% CIs from the multivariate models are shown in Table 3, and the following factors remained positively associated: age 18–65, Han, and ever having had Pap testing.
Reasons for considering self-sampling to be an acceptable option were: convenient (94.32%, 730/774); private (91.60%, 709/774); not embarrassing (93.93%, 727/774); not painful (96.38%, 746/774). Among the 57.24% (1038/1810) of respondents who did not consider that HPV self-sampling for cervical cancer screening was an acceptable option, the main reasons were: the result might not be accurate (86.29%, 894/1036); specimens go bad (83.68%, 867/1036); not sure I did it right (80.59%, 835/1036).
Discussion
In this study, 42.76% of respondents considered HPV self-sampling for cervical cancer screening to be an acceptable option. This is lower than in other studies. HPV self-sampling was deemed acceptable by 68% of participants in a study in rural El Salvador, 15 and more than 90% of women in a Malaysian study. 16 A systematic review of 18,516 women from 24 countries across five continents indicated that there was a high level of acceptability of self-sampling (59%, 95% CI: 48%–69%), with participants preferring self-sampling over clinician sampling due to characteristics such as ease and privacy. 14
In the current study, 57.24% of respondents did not consider HPV self-sampling for cervical cancer screening acceptable, because “the result might not be accurate,” “specimens go bad,” and “not sure I did it right.” Similar concerns have been found in other studies on self-sampling. Most participants worried about whether they performed the test correctly and about the accuracy of test results.17,18 Our study indicated that to further increase the acceptability of HPV self-sampling, precise instructions about the operation of the kit would be needed.
A published meta-analysis 19 has shown that polymerase chain reaction-based HPV-DNA tests could address these concerns, as this test generally showed similar sensitivity on both self-samples and clinician-based samples. Another clinical trial 20 has shown that when HPV message ribonucleic acid analysis is used, the sensitivity of self-sampling HPV samples is lower than clinician-taken cervical HPV samples. To increase the acceptability of self-sampling, it is important to use the polymerase chain reaction-based-DNA analysis method.
To increase self-sampling participation, it is vital to improve HPV-related knowledge, and to raise public awareness of cervical cancer screening. 11 A study of the predominantly Hispanic population residing along the United States-Mexico border confirmed that after participants received education about the test, the acceptability of self-sampling was high. 21 We speculate that one reason for the lower acceptability of self-sampling in our study is that HPV awareness is low among women in Chengdu, although additionally self-sampling is a very new cervical cancer screening method for most women. Education efforts may contribute to wider acceptance of HPV self-sampling. 22
In our study, we found that HPV awareness is higher among women with a higher level of education, exposure to cervical cancer, and ever having undergone Pap testing. We also identified that age 18–65, Han ethnicity, and ever having had Pap testing positively correlated with HPV self-sampling. One implication of our findings was that women who have ever undergone Pap testing considered HPV self-sampling acceptable. Similar results were found: in other studies, 86.2% of women who had ever used self-sampling would choose self-sampling over clinician sampling, and 92.3% think they would test themselves more regularly. 23 However, women with a strong educational background (bachelor degree or above) had no significantly more positive attitudes towards self-sampling screening compared with those who attended high school or less. Similar results were found in Japanese women. 5 These findings indicate that educational background is not associated with the attitude toward self-sampling, and that the experience of physician-led cervical screening is not very good.
In the subgroup with a positive attitude towards self-sampling for the HPV test, 90% of women thought self-sampling were convenient, private, not embarrassing, and not painful. Similar results were found in the previous studies, with level I evidence indicating that HPV self-sampling can increase cancer screening coverage among hard-to-reach women, because of its convenience, privacy, ease of use and relatively low cost. 11 Three randomized controlled trial produced results supporting the efficacy of a self-sampling strategy to increase participation in screening programs.23–26 Our results suggest that HPV self-sampling has great potential in Chengdu, and might be an acceptable alternative to conventional physician-led cervical screening.
In addition to improving the acceptance of self-sampling, efforts should be made to overcome obstacles to the promotion of self-sampling. Anxiety induced by HPV-positive results should be considered, and anxiety may occur in some women with positive HR-HPV results, which may lead to undue cervical screening, unnecessary colposcopies and biopsies, overtreatment, and waste of medical resources.27,28 Future work should examine the effects of education on the psychology and health-seeking behaviours of women with positive HR-HPV, and ultimately on the incidence of cervical cancer. Therefore, future work should explore a reasonable triage strategy for women with positive HR-HPV test results.
This study had some limitations. The results should be interpreted with caution given that only a handful of respondents were non-Han, limiting our ability to assess the effects of ethnicity. Second, our study population consisted of people participating in a physical examination; most of the examinations were paid for by their employers, and most participants had a high degree of education, limiting our ability to assess the effects of self-paying women with less education. It should be considered, however, that the Chinese health authorities have been gradually introducing free screening for cervical cancer. Third, we do not know whether women who indicated that self-sampling would be an acceptable option would actually engage in self-sampling under non-study conditions so it is possible that we may overestimate willingness to use HPV self-sampling. Despite these limitations, our study is more comprehensive than others and so our results are more reliable
Conclusion
This study demonstrates that nearly half of women have positive attitudes toward HPV self-sampling. Education and intervention to raise awareness of HPV and its link to cervical cancer are still needed, although this has been improved. Concise guidance and effective introductory information can further increase the acceptability of the self-sampling HPV test. HPV self-sampling might be an acceptable alternative to conventional physician-led cervical screening in China.
Footnotes
Acknowledgements
We thank the nurses in the Health Management Center for their kind assistance in collecting data, and Liangcheng Xiang for designing the statistical analysis.
Authors' contributions
He JY collected and interpreted the data and drafted the article, He LX contributed substantially to design the questionnaire and revised the manuscript. All authors read and approved the final manuscript.
Availability of data and materials
The data sets used and analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
All the authors state that manuscripts reporting studies involving human participants got the ethics approval and consent from the Ethics Committee, Sichuan University, and the committee reference number is 2016(207). All the participants provided informed consent to take part in our study, and the consent obtained from the participants was written.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Health and Family Planning Commission of Sichuan Province (16PJ302). The funding body did not take part in the design of the study; in data collection, analysis, or interpretation; or in writing the manuscript.