
Abstract
Objectives
Few studies in China have focused on the economic evaluation of newborn screening (NBS) for inherited metabolic disorders (IMDs) by tandem mass spectrometry (MS/MS). This study assesses the total costs, benefits, benefit–cost ratio (BCR), cost–utility ratio (CUR) and incremental cost–utility ratio (ICUR) of NBS using MS/MS compared to the non-screened group.
Methods
The NBS outcomes of newborns who underwent MS/MS screening for IMDs in 2009–2018 were retrospectively reviewed. Records were extracted from a screening management system at the NBS Center of Zhejiang province. A cost–benefit analysis of screening was conducted, assessing screening costs for each subject, and direct and indirect treatment costs for IMDs detected by screening. The putative benefit of clinical outcomes related to early diagnosis was assumed to be improvement in quality of life and prolonged life expectancy in the screened group, as compared to the non-screened group.
Results
Of the 3,040,815 newborns screened, 735 (2.86%) cases were diagnosed through gene sequence analysis. The most frequently occurring types of IMD were amino acid disorders (n = 276), then fatty acid oxidation disorders (n = 248), followed by organic acidaemias (n = 211). The difference in quality-adjusted life-years (QALYs) ranged from 0.78 to 15.4 in the screened group. The CUR was CNY¥ 116,183.89/QALY in the screened group and CNY¥ 3,078,823.65/QALY in the non-screened group. The ICUR was CNY¥ –768,428.76/QALY, and the BCR was 6.09.
Conclusions
NBS using MS/MS can be considered cost-effective in China. The nationwide promotion of NBS using MS/MS deserves priority consideration and sufficient publicity.
Introduction
Newborn screening (NBS) programmes are recognised worldwide as secondary prevention interventions in the ‘field of Public Health’ and their scope is continuously expanding. 1 The early detection of inherited metabolic disorders (IMD) is part of the NBS programme. IMDs refer to a group of diseases with a series of clinical symptoms caused by enzyme defects, abnormal cell membrane function or receptor defects caused by pathogenic gene variants, resulting in collective biochemical metabolism disorder, accumulation of intermediate or bypass metabolites, or lack of final metabolites. 2 Screening aims to detect asymptomatic infants before the onset of clinical symptoms so that proper treatment can be provided to prevent the occurrence of bodily dysfunction and irreversible damage, and so reduces the morbidity, mortality and potential disabilities associated with IMDs. The history of NBS began in the early 1960s, dominated by single disease screening for a long time. Methods such as gas chromatography, mass spectrometry and liquid chromatography mass spectrometry demonstrate obvious flaws, mainly long analysis cycles, low sample fluxes and high false-positive rates; thus, they cannot meet the needs of mass application for NBS. Tandem mass spectrometry (MS/MS) has emerged as a rapid analysis technology with high sensitivity and specificity, which can be used to test a variety of IMDs, including amino acid disorders, organic acidaemias and fatty acid oxidation disorders, through one experiment. 3 The introduction of MS/MS enabled the simultaneous measurement of several metabolites and, consequently, the detection of several diseases in one blood spot and single analysis.
In China, exploratory NBS programmes for IMD began with the screening for phenylketonuria (PKU) in the 1980s in Beijing and Shanghai. In 1994, the ‘Maternal and Infant Health Care Law of the People’s Republic of China’ was promulgated. For the first time, the law proposed to ‘gradually conduct newborn screening’, which provided a fundamental legal guarantee for NBS. The management measures for NBS were issued in 2009, which clearly defined the responsibilities of healthcare administrative departments, all levels of NBS centres and medical institutions. 4 According to data from the National Maternal and Child Health Monitoring Office in 2013, there are 211 NBS centres in China. So far, Shanghai, Zhejiang, Guangzhou as well as other NBS centres have gradually started to use MS/MS to conduct mass screening and have demonstrated good outcomes. At the NBS centre in Zhejiang province, the largest in China, more than 40 newborn genetic and metabolic diseases can be detected by MS/MS. The technique has been used here for nearly 10 years, with 3 million newborns screened. By 2018, approximately 90% of the newborns in Zhejiang province were being screened by MS/MS.
However, owing to the expense of screening and high false-positive rates, an argument has emerged that MS/MS may not be cost-effective for NBS, but should only be used as a clinical diagnostic tool for suspected positive infants. Hence, the cost–benefit and cost–utility of using MS/MS in NBS remain to be investigated. This study is the first to assess the costs, benefits, benefit–cost ratio (BCR), cost–utility ratio (CUR) and incremental cost–utility ratio (ICUR) of the NBS programme using MS/MS in China.
Methods
Study design
We conducted a cost–utility analysis using a decision model. At a decision node (□), a screening or non-screening option must be selected, and at a chance node (○) a variety of outcomes may occur, each with some degree of probability. The clinical outcomes were assumed to be different between patients diagnosed early and late. The costs were calculated for the screening and non-screened groups, as shown schematically in Figure 1. As the false-negative rate of MS/MS could not be obtained from the management system (see below), we assumed a false-negative rate of 0. We took a societal perspective in the calculation of costs and benefits.
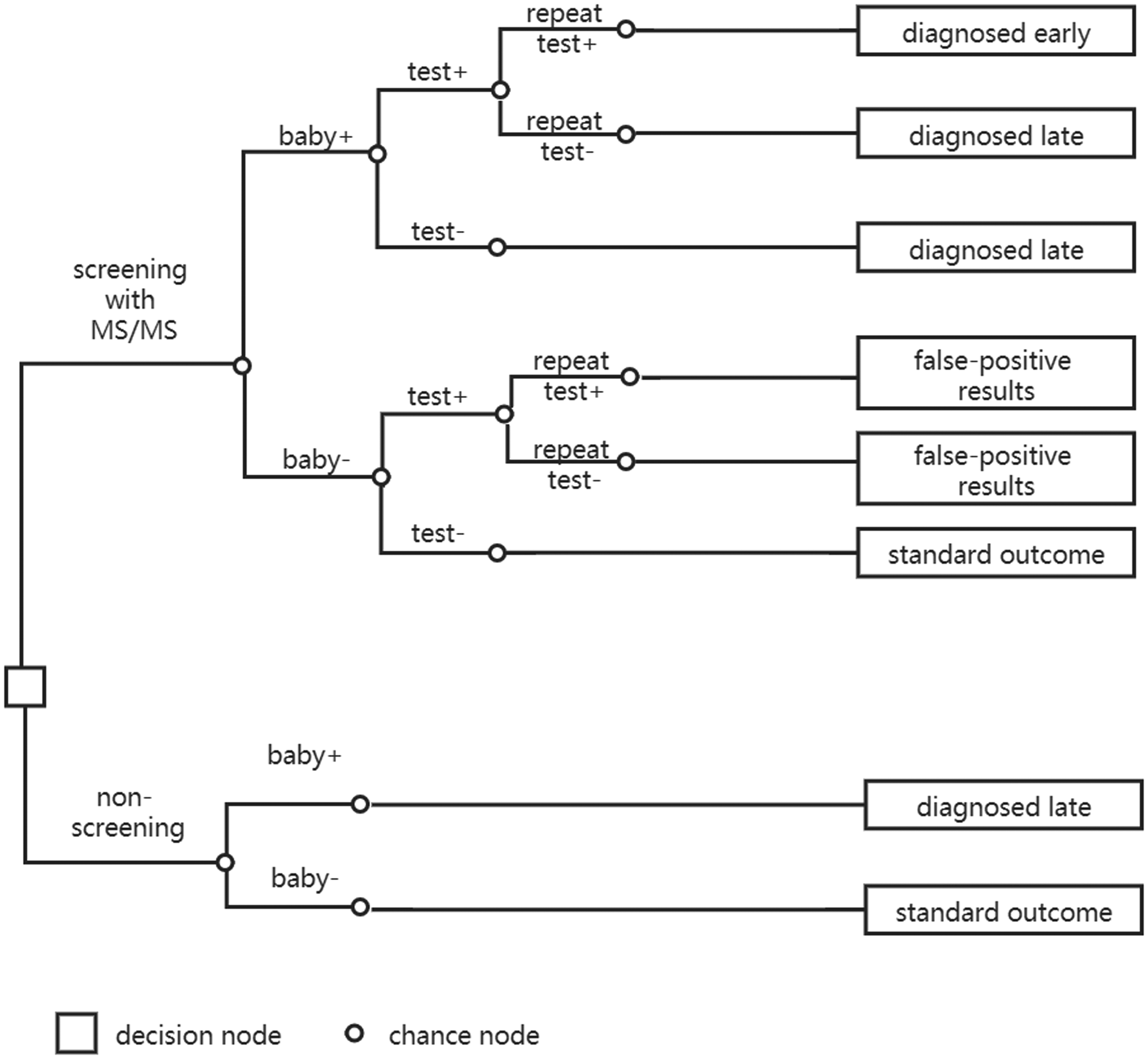
Schematic diagram of decision model.
Source of data
Incidence rate, false-positive rate and internal cost data were obtained from the NBS Management Information System of Zhejiang province, an automated system that currently manages metabolic disorders in more than 10,000 children. In addition, our research team included three paediatricians to estimate the frequency of follow-ups and hospitalisations.
Calculations were based on average costs of standard medical procedures in 3,040,815 newborns who underwent MS/MS screening for IMDs in the NBS centre of Zhejiang province from 2009 to 2018. Standard medical procedures were extracted from local clinical practice. The participating infants underwent first-round screening using dried blood spot no sooner than 72 h old and, for premature babies, no later than 30 days after birth. Those with a positive test result were called back to take another MS/MS test. In the case of two positive test results, a confirmatory test was required. Positive results from MS/MS tests were confirmed with gene sequence analysis, genetic counselling and disease-specified tests for diagnosis.
IMD incidence and false-positive rates
For cost calculation, the disease incidence and false-positive rates were obtained from the NBS Management Information System, which covered all the medical procedures of each NBS participant. For analysis, 28 diseases were diagnosed in the 3,040,815 newborns who underwent MS/MS screening.
Estimated costs
The direct medical costs (e.g. screening tests, confirmatory tests), direct non-medical costs (e.g. special care, transportation) and indirect costs (e.g. wage loss of family members) are specified in the Supplemental Table. Based on our two paediatricians’ experiences and Khneisser et al.’s work, 5 the costs of dietary and pharmaceutical treatments were not included, as they are supposed to be equally incurred once diagnosed. The cost data for screening tests, confirmatory tests, paediatrician consultations and hospitalisations were extracted from the medical department of Children’s Hospital of Zhejiang University School of Medicine.
We assumed that every newborn had a first specimen for screening collected within 72 h. Consequently, the first-round MS/MS requires no extra transportation cost or wage loss. Once they have a positive result, these newborns are called back for the second-round MS/MS, which obviously requires them to be brought by relatives. We assumed that each newborn had two accompanying relatives with the screening taking them a half-day away from work. The wage loss of accompanying relatives was calculated using the per capita income of Zhejiang province. 6 In line with Zhejiang practice, a confirmatory test is required after two positive results. The normal procedure necessitates a specified test for amino acid disorders (CNY¥ 60), specified tests for fatty acid oxidation disorders/organic acidaemias (CNY¥ 115), a paediatrician consultation (CNY¥ 14), genetic counselling (CNY¥ 80) and for some highly suspected cases, a gene sequence test (CNY¥ 3120). Usually, a false-positive result engenders a paediatrician consultation and a specified test for diseases, costing as much as CNY¥ 74–129 in total.
As the complications and severity vary between patients, some of them will also have hospitalisation costs. Expert opinions combined with medical records were used to estimate the hospitalisation frequency for different diseases. We assumed that patients with very long chain acyl-CoA dehydrogenase deficiency (VLCADD), carnitine palmitoyl transferase II deficiency type II (CPT-II), ornithine transcarbamylase deficiency (OTCD), arginosuccinic aciduria (ASA), argininaemia (ARG), methylmalonic acidaemia (MMA), propionic acidaemia (PA), isovaleric acidaemia (IVA) or glutaric acidaemia type I (GA-I) may become symptomatic within the first week of being born and may require hospitalisation owing to metabolic disorders in the first five years. Owing to less intensive hospital stays, the cost of each hospitalisation for early diagnosed infants is CNY¥ 5000. We assumed an initial hospitalisation cost saving of CNY¥ 5000 for early diagnosed infants versus diagnosis made after symptoms manifested. The number of hospitalisations was calculated based on three hospitalisations (early diagnosed) and four hospitalisations (late diagnosed) per year, in 20% of diagnosed patients with VLCADD. For CPT-II, we used three (early diagnosed) and four (late diagnosed) hospitalisations per year in 80% of patients. The data used for OTCD patients were three (early diagnosed) and four (late diagnosed) hospitalisations per year in 60% of patients. Patients with ASA or ARG required three (early diagnosed) and four (late diagnosed) hospitalisations per year in 20% of patients. Two (early diagnosed) and three (late diagnosed) hospitalisations per year were used in 50% of MMA patients and 10% of IVA patients. Hospitalisation calculation was based on two (early diagnosed) and three (late diagnosed) hospitalisations per year in 30% of diagnosed patients with PA/GA-I.
To calculate the cost of treatment, expert opinion was adopted to estimate the follow-up frequency and what tests needed to be done each time. The estimated follow-up tests included 17 categories, namely: MS/MS (CNY¥ 390), blood gas assay (CNY¥ 91), blood ammonia assay (CNY¥ 25), blood homocysteine assay (CNY¥ 48), liver function test (CNY¥ 60), phenylalanine determination (CNY¥ 30), alpha-fetoprotein determination (CNY¥ 25), urinary gas chromatography (CNY¥ 300), blood routine test (CNY¥ 15), blood biochemistry (CNY¥ 181), microelement test (CNY¥ 39), echocardiography (CNY¥ 130), electrocardiography (CNY¥ 20), magnetic resonance imaging (CNY¥ 689.6), Ages and Stages Questionnaires (CNY¥ 119), Wechsler Intelligence Scale (CNY¥ 184) and Bayley Scales of Infant development (CNY¥ 184). These tests were divided into different combinations to suit each disease, costing CNY¥ 810 (SCADD) to CNY¥ 4481 (MMA) per year. For most IMDs, we assumed an extra two annual follow-ups for patients who were diagnosed late.
Estimation of transportation cost during the years of life of IMD patients was based on a survey conducted on 307 patients from both local and non-local regions. As first-round MS/MS screening was carried out in the local hospital, the transportation cost for this was calculated as CNY¥ 18 per case. The proportions of local and non-local confirmed cases were used to estimate the distribution of the newborns who were recalled. CNY¥ 338 per visit was estimated as the transportation cost for non-local patients.
We used the per capita basic rehabilitative services subsidy to calculate the cost of rehabilitative services, 7 and the data on per capita compulsory education expenditure for disabled children to calculate the cost of special education. 8
For indirect costs, the wage losses of accompanying relatives/family members were calculated by the per capita income of Zhejiang province. Of disabled children, 70% can be regarded as total loss and 30% as partial loss of labour force. 9 We used the gap between per capita minimum wage and per capita income to calculate the partial wage loss of disabled patients. For the calculation of total loss of labour force, the per capita income of Zhejiang province was used. We also assumed a 50% wage loss of one family member for each disabled patient, because in China most disabled people are cared for at home by family caregivers.10,11
A lack of discount could encourage policymakers to delay implementing health programmes indefinitely.12,13 In this study, all the costs and benefits were discounted at 5% during the years of life of patients with IMDs, a commonly used figure that is recommended by the Chinese Guidelines for Pharmacoeconomic Evaluations. 14
Estimated life expectancy and quality-adjusted life-years
The onset of complications of a primary metabolic disease in both screened and non-screened patients depends on the integrated operation of many factors. The putative benefit of early diagnosis through MS/MS screening was assumed to be an improvement in life expectancy and quality-adjusted life-years (QALYs) after treatment. As the severity and responsiveness to treatment varies according to the type of disease, some would not be detected without MS/MS screening, 15 so the specified life expectancy for each IMD was used for calculation. We assumed a 0.5–55 year difference in life expectancy between patients diagnosed late and those diagnosed early by screening.
The patient’s burden of having an IMD has also been described by impairment in utilities,16,17 although in some studies18,19 adult IMD patients had similar quality of life scores to normal. However, as the research design and sampling method ruled, only patients who finished the questionnaires or replied to the emails (which apparently indicates a higher cognitive level) were included, leading to inevitable bias in the results. Hence, the utility scores of patients with IMDs in this study were estimated to have a 0.3–0.7 difference. This difference between early and late diagnosed patients varied according to clinical outcome and severity of disorder. Additionally, a rate of 5% was adopted to calculate the total discounted QALYs.
Results
Incidence of IMDs
As infants with IMDs may die without clear diagnosis, we assumed that the incidence rates in the non-screened group were similar to those in the screened group. A total of 3,040,815 newborns were screened between 2009 and 2018; 26,297 of them were suspected to be positive after first-round screening and were called back for another MS/MS test. Of these, 25,670 responded and were re-tested, and ultimately 735 cases were diagnosed through confirmatory tests. The most frequent causes of IMDs are amino acid disorders, and fatty acid oxidation disorders in most cases, followed by organic acidaemias. The number of diagnosed cases and incidence rates of 28 IMDs are specified in Table 1.
Incidence rates of 28 inherited metabolic disorders diagnosed in newborns after tandem mass spectrometry screening in 2009–2018 in Zhejiang, China.
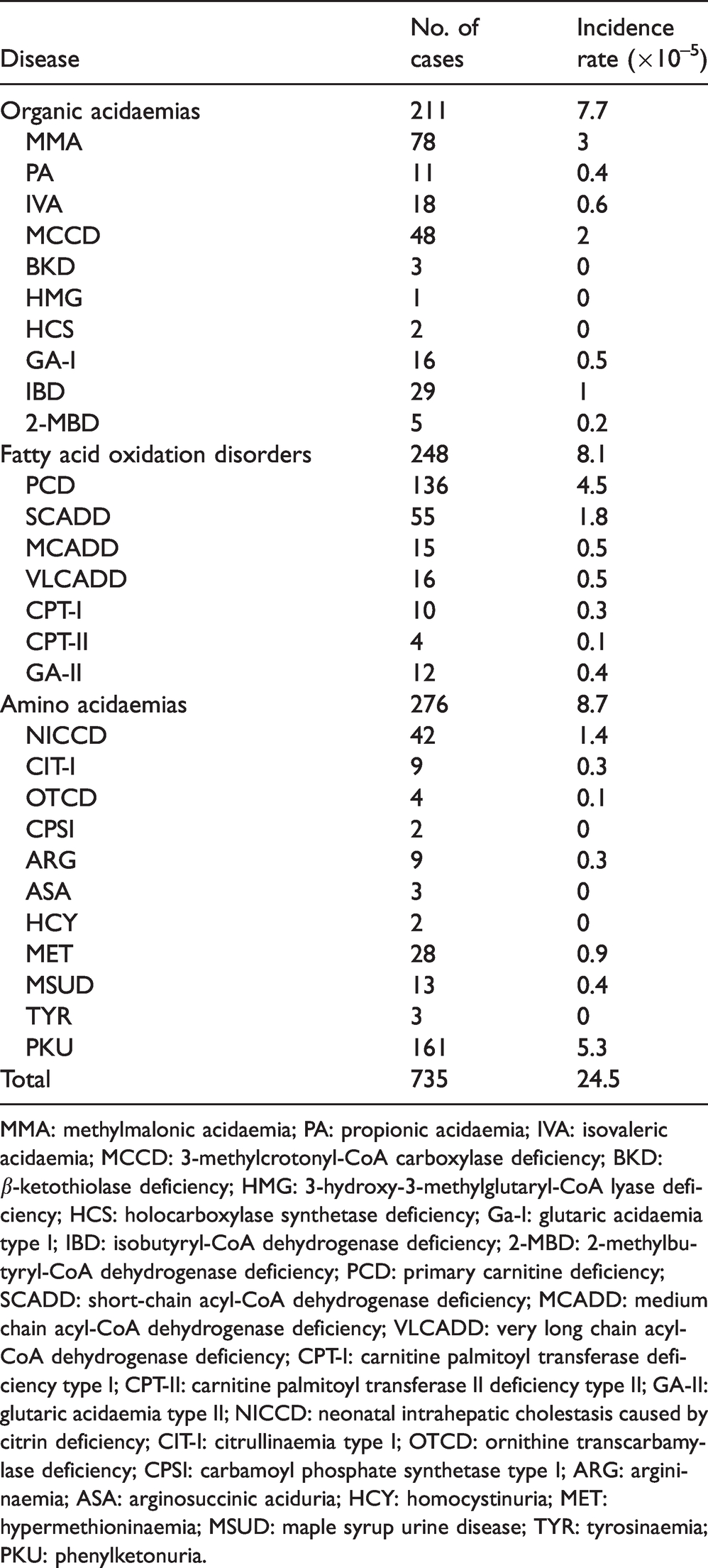
MMA: methylmalonic acidaemia; PA: propionic acidaemia; IVA: isovaleric acidaemia; MCCD: 3-methylcrotonyl-CoA carboxylase deficiency; BKD: β-ketothiolase deficiency; HMG: 3-hydroxy-3-methylglutaryl-CoA lyase deficiency; HCS: holocarboxylase synthetase deficiency; Ga-I: glutaric acidaemia type I; IBD: isobutyryl-CoA dehydrogenase deficiency; 2-MBD: 2-methylbutyryl-CoA dehydrogenase deficiency; PCD: primary carnitine deficiency; SCADD: short-chain acyl-CoA dehydrogenase deficiency; MCADD: medium chain acyl-CoA dehydrogenase deficiency; VLCADD: very long chain acyl-CoA dehydrogenase deficiency; CPT-I: carnitine palmitoyl transferase deficiency type I; CPT-II: carnitine palmitoyl transferase II deficiency type II; GA-II: glutaric acidaemia type II; NICCD: neonatal intrahepatic cholestasis caused by citrin deficiency; CIT-I: citrullinaemia type I; OTCD: ornithine transcarbamylase deficiency; CPSI: carbamoyl phosphate synthetase type I; ARG: argininaemia; ASA: arginosuccinic aciduria; HCY: homocystinuria; MET: hypermethioninaemia; MSUD: maple syrup urine disease; TYR: tyrosinaemia; PKU: phenylketonuria.
Costs
Based on the medical records from the MS/MS management system in the NBS centre of Zhejiang province, the number of false-positive test results and associated costs are presented in a cohort of 100,000 newborns. The mean per-patient cost of false-positive test results was CNY¥ 23,905.00. Life-time discounted treatment cost for each disease ranged from CNY¥ 2753.33 (GA-II) to CNY¥ 82,920.62 (HMG) for early diagnosed patients and CNY¥ 4578.62 (GA-II) to CNY¥ 108,993.5 (CPT-II) for late diagnosed patients. However, the life-time discounted treatment costs for early diagnosed patients were not always lower than those of late diagnosed patients. For BKD, HCS, CPT-I, CIT-I and TYR, the low number of years of life gained by screening and expensive treatment costs led to higher total discounted treatment costs (Table 2).
Costs of treatment and of false-positive results of MS/MS screening.
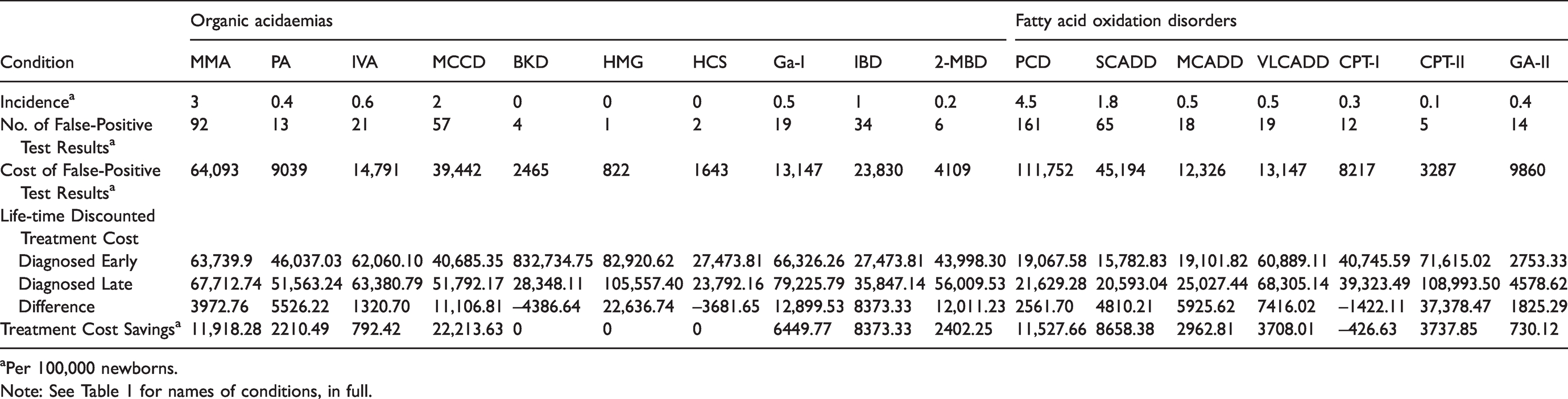
aPer 100,000 newborns.
Note: See Table 1 for names of conditions, in full.
Costs of treatment and of false-positive results of MS/MS screening (continued).
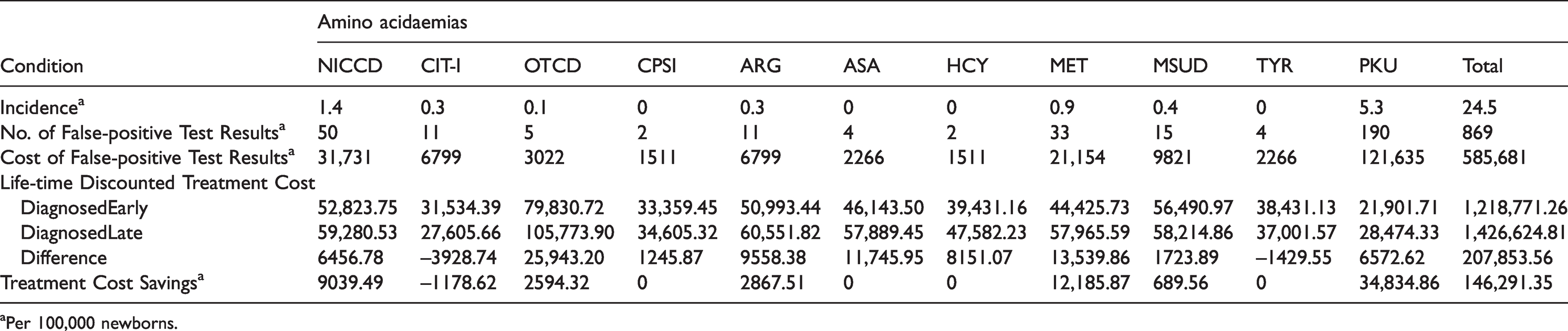
aPer 100,000 newborns.
The total direct medical cost was CNY¥ 80,739.88 per patient diagnosed, with the biggest factor being treatment cost (CNY¥ 49,745.77) (see Table 3). Compared with the non-screened group, most savings for all cost factors were realised by reduction in wage loss because of decreased follow-up frequency, disability and mortality rates. Wage loss of accompanying relatives per patient was CNY¥ 160,420.19 and 232,917.86, for early and late diagnosed patients respectively. The cost of special care for disabled patients, including rehabilitation services for 0–6 years and special education for 7–15 years, was CNY¥ 246,640.21 and 1,651,432.05 per patient, respectively. The average cost of transportation was CNY¥ 7622.68 in the screened group and CNY¥ 10,220.98 in the non-screened group.
Lifetime costs per patient in screened and non-screened group.
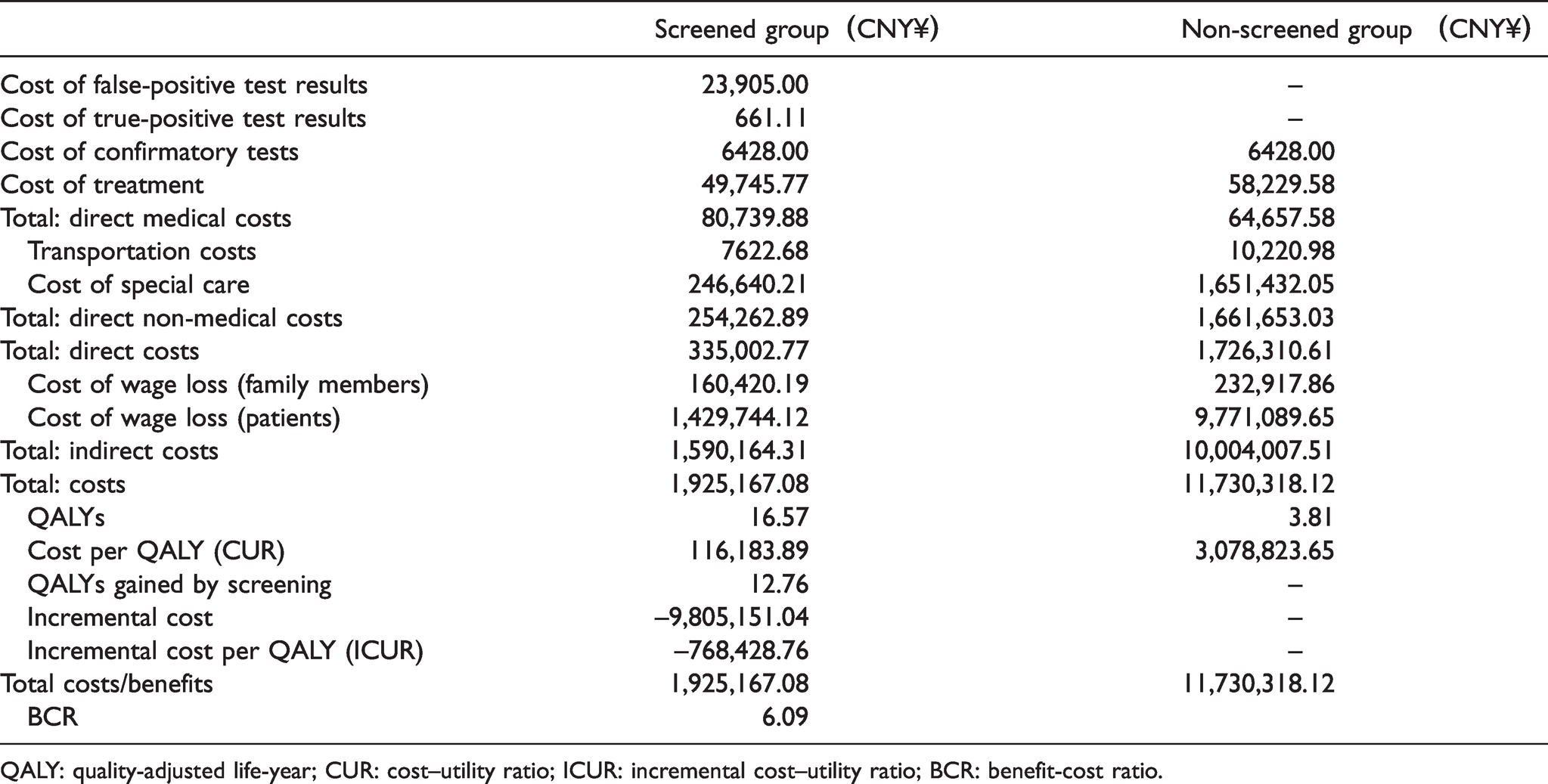
QALY: quality-adjusted life-year; CUR: cost–utility ratio; ICUR: incremental cost–utility ratio; BCR: benefit-cost ratio.
Utilities
The prolongation of years of life and improvement of utilities resulted in a total discounted QALY difference ranging from 0.78 to 15.40. Patients with BKD or HCS seemed especially to benefit from early diagnosis by screening. In contrast, the benefit was much less for those with GA-II or PA. The estimated life expectancy and QALYs for patients diagnosed early and diagnosed late are specified in Table 4.
Potential life expectancy (in years) and quality-adjusted life-years (QALYs).
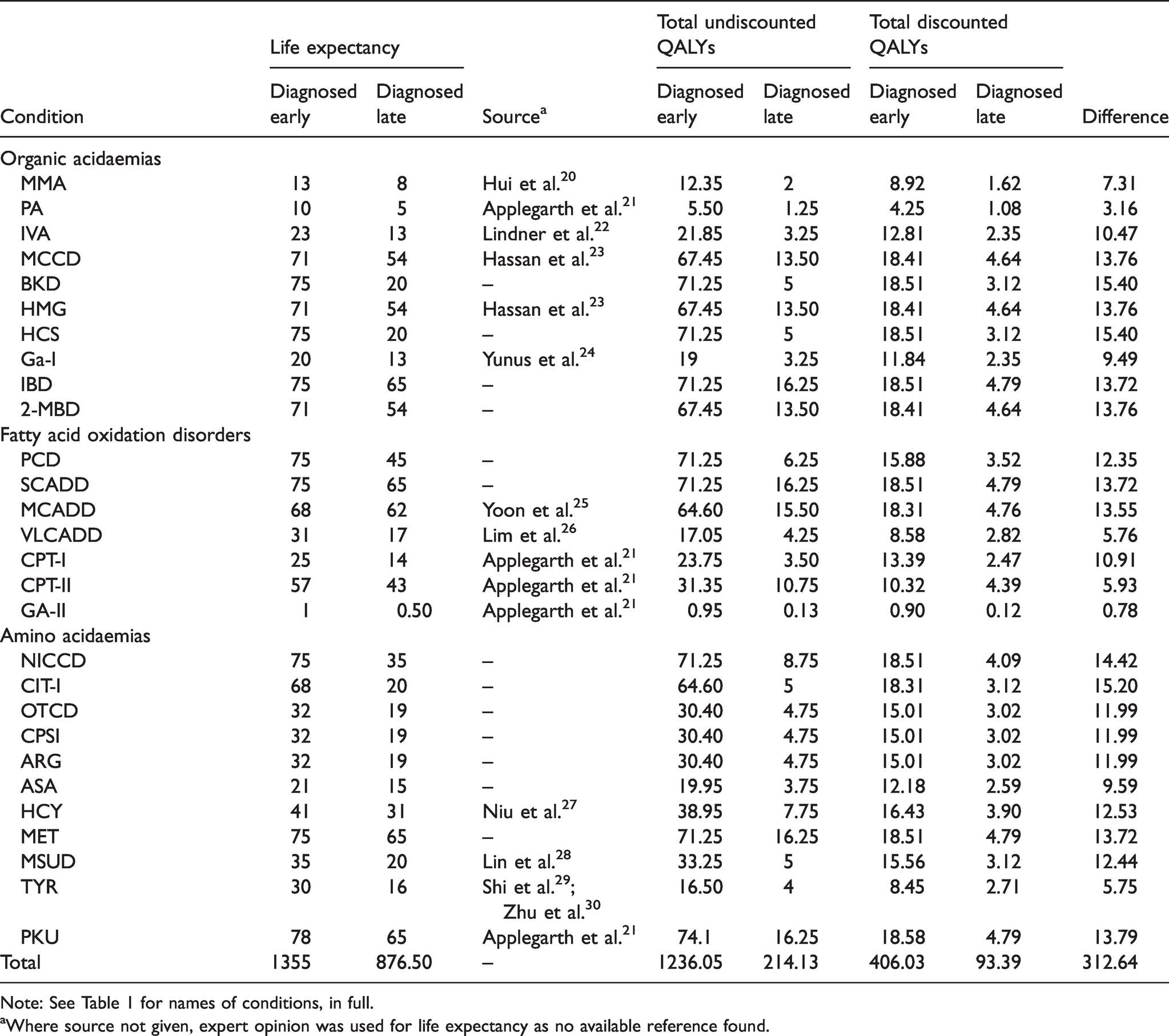
Note: See Table 1 for names of conditions, in full.
aWhere source not given, expert opinion was used for life expectancy as no available reference found.
Cost–utility analysis
The results of the cost–utility analysis are presented in Table 3. The CUR was CNY¥ 116,183.89/QALY and CNY¥ 3,078,823.65/QALY in the screened and non-screened group, respectively. The ICUR for the screened group was CNY¥ –768,428.76/QALY compared to the non-screened group. The costs and benefits per patient diagnosed were CNY¥ 1,925,167.08 and 11,730,318.12, respectively, and the BCR was 6.09.
Discussion
The spectrum and incidence of IMDs differ among populations, which has been well characterised in Caucasians but much less so in Chinese. 20 Several studies have been carried out in other countries,21–26 while a growing number of studies of IMDs in the Chinese population are emerging,27–31 mostly conducted by screening programmes. This study reports the incidence rates of IMDs in the eastern Chinese population using data from the NBS centres of Zhejiang province during 2009–2018, with 3 million newborns screened. The collective incidence rate of 28 IMDs included in the screening programme is 1/4137, which is lower than the reported incidence from a pilot study conducted in Mainland China (1/3795), 29 as well as from studies in many other countries; for example, 1/2500 in Canada, 21 1/2900 in Germany, 22 1/1944 in Egypt, 23 1/2916 in Malaysia, 24 1/2800 in South Korea 25 and 1/3165 in Singapore. 26 Compared to other regions in China,30–33 the incidence rate of IMDs in Zhejiang province was also relatively low, excluding Taiwan (1/5882).
In this study, the most frequent cause of IMDs was amino acid oxidation disorders, in which PKU accounted for 58.33%. This suggests that PKU is the most common amino acid oxidation disorder in Zhejiang province. The second most common disorder was PCD, which accounted for 136 patients in this study, with an incidence rate of 1/22,359. Meanwhile, the incidence of BKD, HMG, HCS, CPSI, ASA, HCY and TYR were relatively rare, even lower than 1/1,000,000.
Early diagnosis of IMDs and regular follow-ups are important to improve quality of life and long-term survival, and to prevent the occurrence of body dysfunction and irreversible damage. NBS for these disorders could lighten the social burden related to the incapacitating symptoms of these diseases. Although MS/MS has been conducted in China for over 10 years, studies focused on the economic evaluation of this technique are still lacking, with more efforts devoted to studies on screening for a single disease (e.g. congenital hypothyroidism, PKU).34,35
In this study, the total cost per early-diagnosed patient was CNY¥ 1,925,167.08, saving CNY¥ 9,805,151.04 compared to late-diagnosed patients. Savings are primarily attributed to the reduction in wage loss of family members and patients (85.60%), and the avoidance of costs of special care (14.29%), which both benefit from the reduction in mortality and severity of IMDs. Treatment cost savings only accounted for 0.09% of the total cost savings, indicating that the direct medical cost would not show a substantial decrease because of MS/MS screening. Some diseases will continue to have high mortality and poor clinical outcome even when detected by MS/MS before symptom onset and being well managed from then on. Table 2 presents the life-time discounted treatment cost savings for each disorder both per patient and per 100,000 newborns, the latter taking the incidence rate into consideration. It seems that MCCD, MMA and MET could each achieve a treatment cost saving of more than CNY¥ 10,000 per 100,000 newborns screened. While not considering the incidence rate, HMG, OTCD and CPT-II could each have more than CNY¥ 20,000 saved in treatment costs per early-diagnosed patient. Similar to some other studies, we quantified the monetary value of years of life saved and the wage loss of caregivers due to sick children as indirect cost. Failure to add indirect cost in a cost–utility analysis might make the results more likely to be cost-effective.
The estimated cost per QALY (CUR) was CNY¥ 116,183.89 (for the screened group) and CNY¥ 3,078,823.65 (for the non-screened group), saving CNY¥ 2,962,639.76 per QALY. The incremental cost per QALY (ICUR) was CNY¥ –768,428.76 compared to the non-screened group, indicating that the NBS programme could both gain QALYs and save costs at the same time.
NBS has been found to be cost-effective by other research groups in China,32–35 although the estimated BCR varies widely. In their 2011 study, 35 Zhang et al. reported that the estimated BCR of screening for PKU and hypothyroidism in China was 1:6.9, whereas the BCRs were estimated to range from 1:1.17 to 1:141.96 in studies carried out on these two disorders separately.33,34,36 Meanwhile, some of the benefits of early detection of IMDs cannot be estimated through a monetary analysis, such as improved psychosocial development in both patients themselves and caregivers. The results still showed that MS/MS screening for IMDs may be considered to be economically beneficial, which is consistent with the studies carried out in other countries.5,21,37
Despite the use of MS/MS in China for many years, its application is mainly concentrated in Shanghai, Zhejiang, Guangdong and other developed areas with high-end laboratories. 38 Neither corresponding technical specifications nor NBS data have been reported from less-developed areas, which are more likely to have a high rate of consanguineous marriages leading to a high incidence of IMDs. From early 2015, the NHS Newborn Blood Spot Screening Programme in England started to offer screening for nine disorders, six of which were IMDs. The screening programme was regulated by the Department of Health through the National Screening Committee (UK), and clear recommendations exist regarding management and follow-up of positive screen results. 39 Similar technical specifications or recommendations need to be agreed in China, as does the reimbursement policy related to NBS expenses nationwide.
The major limitation of this study is that it did not apply a Markov model-based analysis to evaluate the costs and health benefits of MS/MS screening in China. Moreover, this study did not consider poor adherence in follow-up, assuming that all patients would treat their disease for life. However, a substantial number of patients do have their treatment discontinued because of economic problems faced by their parents. 38
Conclusions
NBS using MS/MS can be considered cost-effective, as it provides a BCR of 6.09, comparing favourably with some screening programmes for a single disease. The CUR and ICUR for the screened group were CNY¥ 116,183.89/QALY and –768,428.7649/QALY, suggesting that the MS/MS screening programme could gain QALYs and save costs at the same time. The results indicate the need for sufficient publicity and priority consideration for nationwide promotion of NBS using MS/MS in China.
Supplemental Material
sj-pdf-1-msc-10.1177_09691413211021621 - Supplemental material for Newborn screening for inherited metabolic diseases using tandem mass spectrometry in China: Outcome and cost–utility analysis
Supplemental material, sj-pdf-1-msc-10.1177_09691413211021621 for Newborn screening for inherited metabolic diseases using tandem mass spectrometry in China: Outcome and cost–utility analysis by Zixuan Zhao, Chi Chen, Xueshan Sun, Duo Zhou, Xinwen Huang and Hengjin Dong in Journal of Medical Screening
Footnotes
Authors’ contributions
Xinwen Huang and Hengjin Dong initiated, planned and designed the study. Xinwen Huang had full access to all the data in the study. Zixuan Zhao and Chi Chen conducted the data acquisition, management and analysis. Xueshan Sun and Duo Zhou provided the statistical input for the data analysis. Zixuan Zhao and Chi Chen drafted the manuscript. All authors interpreted the study results and critically revised the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Key Research and Development Program of China (Grant Number 2018YFC 1002200).
Supplemental Material
Supplemental material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.