
Abstract
Objectives
Few countries in the Middle East-North Africa region have adopted national newborn screening for inborn errors of metabolism by tandem mass spectrometry (MS/MS). We aimed to evaluate the cost-benefit of newborn screening for such disorders in Lebanon, as a model for other developing countries in the region.
Methods
Average costs of expected care for inborn errors of metabolism cases as a group, between ages 0 and 18, early and late diagnosed, were calculated from 2007 to 2013. The monetary value of early detection using MS/MS was compared with that of clinical “late detection”, including cost of diagnosis and hospitalizations.
Results
During this period, 126000 newborns were screened. Incidence of detected cases was 1/1482, which can be explained by high consanguinity rates in Lebanon. A reduction by half of direct cost of care, reaching on average 31,631 USD per detected case was shown. This difference more than covers the expense of starting a newborn screening programme.
Conclusion
Although this model does not take into consideration the indirect benefits of the better quality of life of those screened early, it can be argued that direct and indirect costs saved through early detection of these disorders are important enough to justify universal publicly-funded screening, especially in developing countries with high consanguinity rates, as shown through this data from Lebanon.
Introduction
Disorders targeted and detected by newborn screening using MS/MS between 2007 and 2013.
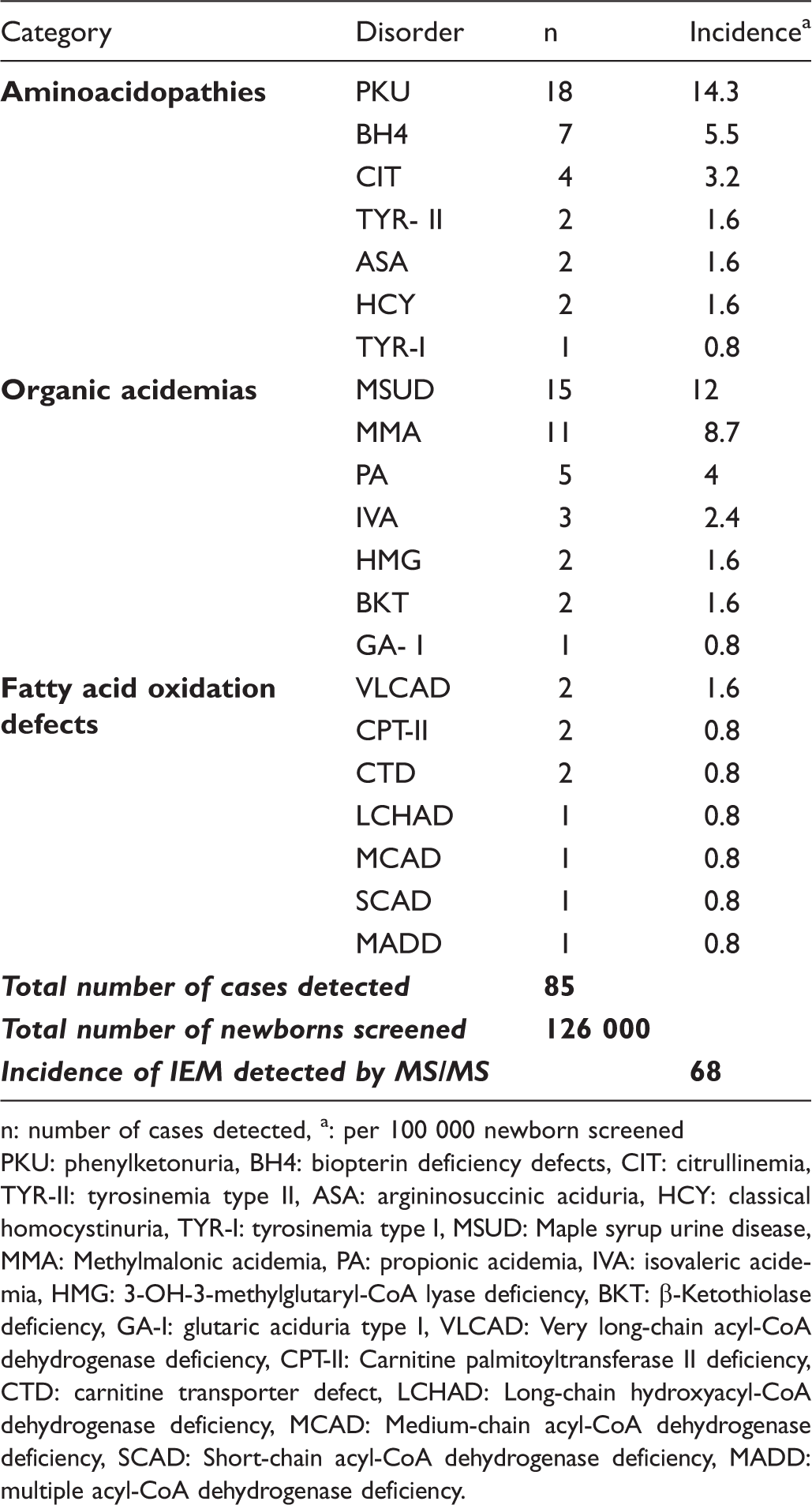
n: number of cases detected, a: per 100 000 newborn screened
PKU: phenylketonuria, BH4: biopterin deficiency defects, CIT: citrullinemia, TYR-II: tyrosinemia type II, ASA: argininosuccinic aciduria, HCY: classical homocystinuria, TYR-I: tyrosinemia type I, MSUD: Maple syrup urine disease, MMA: Methylmalonic acidemia, PA: propionic acidemia, IVA: isovaleric acidemia, HMG: 3-OH-3-methylglutaryl-CoA lyase deficiency, BKT: β-Ketothiolase deficiency, GA-I: glutaric aciduria type I, VLCAD: Very long-chain acyl-CoA dehydrogenase deficiency, CPT-II: Carnitine palmitoyltransferase II deficiency, CTD: carnitine transporter defect, LCHAD: Long-chain hydroxyacyl-CoA dehydrogenase deficiency, MCAD: Medium-chain acyl-CoA dehydrogenase deficiency, SCAD: Short-chain acyl-CoA dehydrogenase deficiency, MADD: multiple acyl-CoA dehydrogenase deficiency.
The cost of neonatal screening in Lebanon is rarely included in insurance schemes, and is still largely covered by the end-users. Consequently, less than half of Lebanese newborns receive any screening at birth. 4 Third party payers do cover hospitalization, treatment, and follow-up costs when a baby becomes ill. Late-diagnosed IEM cases may become symptomatic within the first weeks of life. Symptoms often lead to hospitalization, usually in expensive neonatal intensive care units. These infants may be referred to several medical specialists, and undergo various expensive tests, before an adequate diagnosis is suspected and established.
We here compare costs for IEM patients diagnosed early by newborn screening, versus costs for those diagnosed late, after the neonatal period and up to age 18 years. Our goal is to provide a simple, evidence-based model that may help to secure a governmental decision for a newborn screening programme provided free-of-charge to all newborns, and as a model for other developing countries in the region.
Methods
Calculations were based on average costs of medical procedures in Lebanon during the study period, without adjustment for annual inflation. For a late-detected IEM case, average cost of work-up needed to reach a diagnosis, including laboratory biochemical tests and radiological investigations, was calculated.
Cost of newborn screening was calculated, taking into account start-up costs, overheads, salaries, materials, sampling devices and transportation, and extra costs of confirmation tests for suspected cases for which no additional charge is requested. Cost of a case of any specific entity (or group of related entities) detected per 100,000 tested has been calculated using a direct formula: Cost per case = (unit cost * 100,000)/(incidence per 100,000).
For early- and late-detected IEM cases, average cost of hospitalizations, multidisciplinary medical consultations, and special care, including physical, occupational, speech and dietary therapy for treatment of complications and follow-up care was also calculated.
Remedial medication and/or special diet expenses were not factored into the analysis, as they are expected to be equally incurred for both early and late detected cases once a diagnosis is reached.
As an example, calculation of the actual cost of diagnosis, follow-up, medical care and hospitalizations of one early- versus two late- diagnosed methylmalonic acidemia (MMA) patients was also performed.
Results
In this cost-analysis of late-detected IEM, we have included only the conditions that would be expected to be detected by MS/MS screening (Table 1). The average calculated cost of diagnosis of a late detected IEM case in Lebanon is 2,900 USD. Delay in physical development and vulnerability to repeated infections will affect late diagnosed or treated IEM cases more so than those detected earlier. Hospitalizations in the first five years of life for any medical cause, related to the genetic problem or not, will also differ in frequency and severity, depending on the precocity of the genetic diagnosis. It is estimated that early diagnosed cases will be hospitalized once in the first five years versus three times for late diagnosed cases. 7 Number of hospitalizations was calculated based on at least one hospitalization in the first five years for an early-detected patient, and at least three times for a late–detected patient.
The cost of each hospitalization for an average of five days for an IEM case is around 1500 USD for early detected versus 2500 USD for late detected cases. As late detected cases present with higher morbidity, due to the complications of their primary untreated metabolic disease, the cost of each acute decompensation is higher than for those detected and treated early in life. The average cost for outpatient follow-up during the first five years of life including specialized medical consultation fees and special care, as well as metabolic tests, is 2200 USD for early detected and 4700 USD for late detected cases. Assuming affected children survive their first five year of life, the costs of hospitalization between ages 5 and 18 will be higher than for unaffected children, while the overall probability of acute metabolic decompensation requiring hospitalization will decrease. Average hospitalization costs are 1400 USD for early detected versus 2600 USD for late detected cases, assuming that the same ratio of 1:3 hospitalizations remains at least the same over the entire life interval. Out-patient medical care for follow-up, including specialized metabolic and dietary consultations with regular metabolic testing, as well as special psychometric education and rehabilitation care during that life interval are 1,900 and 4,500 USD annually, respectively, for early or late detected cases.
Newborn screening conducted at the USJ-NSL costs 12 USD, consisting of 3 USD to cover G6PD screening 4 , 7 USD for IEM entities, and 2 USD for congenital hypothyroidism and galactosemia screening. Between 2007 and 2013, among 126,000 samples tested at USJ-NSL using MS/MS, 85 cases were confirmed to have an IEM (Table 1), yielding an IEM incidence of 68 per 100 000 newborns screened, or 1/1482. Using this incidence, the cost of an IEM case detected per 100,000 tested was calculated using the formula: Cost per case = (unit cost * 100,000)/(incidence per 100,000). This gives a direct cost to detect an IEM case of 10,295 USD. This analysis shows that there may be direct savings from early detection of IEM disorders.
Cost-comparison of a methylmalonic acidemia (MMA) case detected by MS/MS in the neonatal period and two “late-detected “cases (All costs in USD).
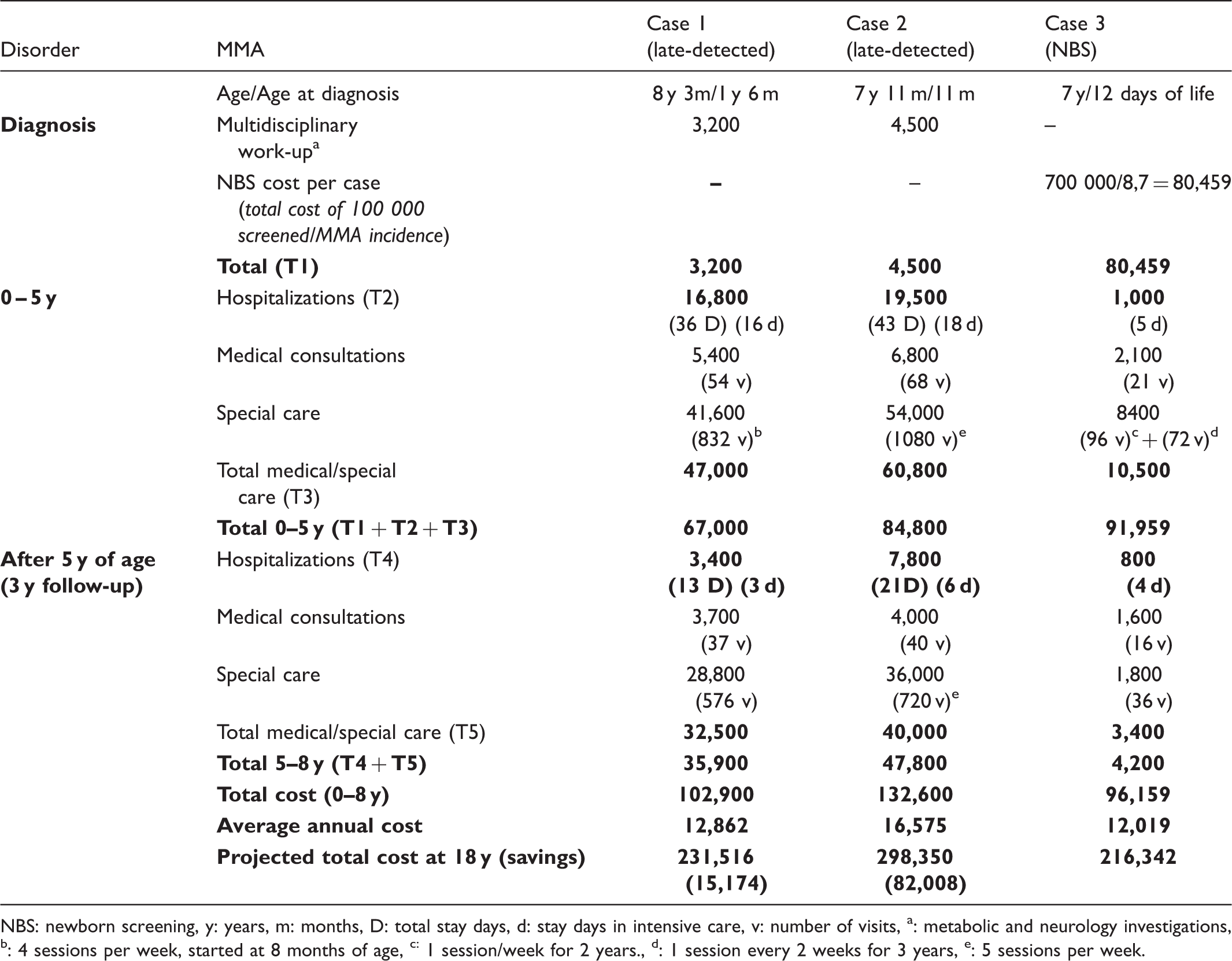
NBS: newborn screening, y: years, m: months, D: total stay days, d: stay days in intensive care, v: number of visits, a: metabolic and neurology investigations, b: 4 sessions per week, started at 8 months of age, c: 1 session/week for 2 years., d: 1 session every 2 weeks for 3 years, e: 5 sessions per week.
Discussion
Early diagnosis and adequate follow-up of IEM is important to reduce mortality and/or severity, and to delay or prevent the onset of incapacitating symptoms. Newborn screening for these disorders may lighten the social burden associated with irreversible effects of these diseases8,9, and a better outcome with fewer disabilities and lower mortality in patients at age six has been shown. 10
This rough comparison of costs associated with early screening versus late diagnosis of these inherited disorders is the first conducted in Lebanon. Our results are similar to those found in countries with much more sophisticated means of cost assessment 11 and more specific testing. 12
Savings are primarily attributable to avoided costs of medical care, and to benefits derived from the prevention of mental disability, which may partially or totally disrupt the future life and productivity of patients.9,13 For instance, an early detected, well- managed maple syrup urine disease or methylmalonic acidemia patient in Lebanon may lead a virtually normal life, can hold a job during adult life, and earn at least the legal minimal wage of 5,400 USD 14 for each fully productive year with a normal life-expectancy of 69 years. Our estimates did not include benefits realized when early screening leads to saving a life in the perinatal period. Estimating the monetary value of a life is an actuarial exercise which usually includes several arbitrary assumptions, and this has never been attempted using the Lebanese population. While recognizing the importance of this element of benefit, we did not attempt to quantify the value of a life saved. 15 Similarly, indirect savings realized by caregivers when no personal income is lost while caring for sick children, or savings realized from avoidance of moral and emotional discomfort associated with long-term disabilities were not included in the calculation. 16 If these indirect costs were also considered, there are likely to be substantial benefits associated with early detection.
In developed countries with expanded newborn screening, the reported incidence of IEM cases diagnosed after detection by MS/MS is about 1 in 4,300 screened. 17 In countries with high rates of consanguineous marriages such as Lebanon (35,5%) 18 , where incidence of IEM diagnosed by MSMS reaches 1 in 1482, nationwide newborn screening becomes essential. Ideally such a programme should be Government funded, however, the national healthcare system in Lebanon covers only basic immunization. Screening at birth could be adopted nationally, and reimbursement mandated through social security or private insurance schemes (as has happened with breast cancer screening, which is now reimbursed by most insurers). For those without insurance cover, direct funding from the ministry of public health may be necessary.
This analysis shows that newborn screening for IEM may be considered economically beneficial, despite the relative rarity of these diseases. It supports previous economic analyses of similar programmes showing that screening is cost-effective. Patient advocacy and other concerned civil activist groups should be encouraged to revive their demands for mandatory universal publicly funded newborn screening for IEM in developing countries of the MENA region.
Footnotes
Acknowledgement
This study was partially funded by the Caisse Nationale de Recherche Scientifique in Lebanon, and by special funds from Saint Joseph University.
Declaration of conflicting interests
The authors have no conflict of interest to declare.