
Abstract
Objectives
Routine analysis showed that between 1 June and 30 November 2014, only 47.6% of expected follow-up visits at the diagnostic level were registered in the Polish Universal Neonatal Hearing Screening Programme central database. We attempted to detect and analyse the reasons for this low percentage.
Methods
A telephone survey questionnaire was developed for parents whose children had not registered for consultation at the diagnostic level, or had not received a final diagnosis according to the programme database. Questions aimed to verify the database records and compare these with information received from and given to parents. From the 7888 children not registered at the diagnostic level, 3239 records were randomly selected, i.e. 52.4% of those who had been expected to attend.
Results
Questions were answered by 1950 parents (60.2% of the selected group). Of these, 52.1% (n = 734) had attended for diagnostic tests, but this was not recorded in the database. The most common reasons for not attending were the long waiting time for the visit (36.09%), lack of referral to a visit (25.9%) and conscious parent decision (16.35%).
Conclusion
The telephone survey disclosed omissions in database registration, and that in fact 83.6% of children had attended at the diagnostic level.
Introduction
In the Polish Universal Neonatal Hearing Screening Programme (PUNHSP), all newborns are tested using the otoacoustic emission (OAE) method on day 2 or 3 of their life (the 1st PUNHSP level). A second OAE test is performed on the day of hospital discharge, and information on risk factors (RF) for hearing loss is collected.1,2 Each screened infant either receives a certificate confirming the screening result for those who meet the OAE pass criteria without RF (blue certificate), or advising that further diagnosis is necessary for children who fail to meet the OAE pass criteria with RF for hearing loss or without the OAE test for any reason (yellow certificate). Under this programme, those children should attend a follow-up visit within the first three months of life (2nd PUNHSP level), and the centre at the 2nd PUNHSP level should give the final diagnosis by the sixth month of life. 3 Published data in the PUNHSP central database (CDB) have shown that attendance for follow-up at the 2nd PUNHSP level was 55.6%. 3 We aimed to identify and analyse the reasons underlying the low number of children attending the 2nd PUNHSP level, and to estimate the actual percentage of children coming for further diagnosis of hearing loss.
Methods
Between 1 June and 30 November 2014, 182,978 children were registered in the PUNHSP CDB at the 1st PUNHSP level. From this group, 15,049 children (8.2%) required further diagnosis at the 2nd PUNHSP level (children who failed to meet the OAE pass criteria, with RF, and children not tested) (Figure 1). An analysis of entries in the CDB at the 2nd PUNHSP level showed that only 47.6% (n = 7161) of children who should have been consulted were registered. A visit was not noted for 7888 children (52.4%). The telephone survey covered 3239 randomly selected records out of 7888 parents of children born in six successive months of the defined period, for whom a visit at the 2nd level was not recorded in CDB within at least three months of birth. Each parent of children participating in PUNHSP consents to the processing of personal data, so it was possible to carry out the telephone survey.
Flowchart of children in the central database of PUNHSP between 1 June 2014 and 30 November 2014 with the outcomes of telephone survey.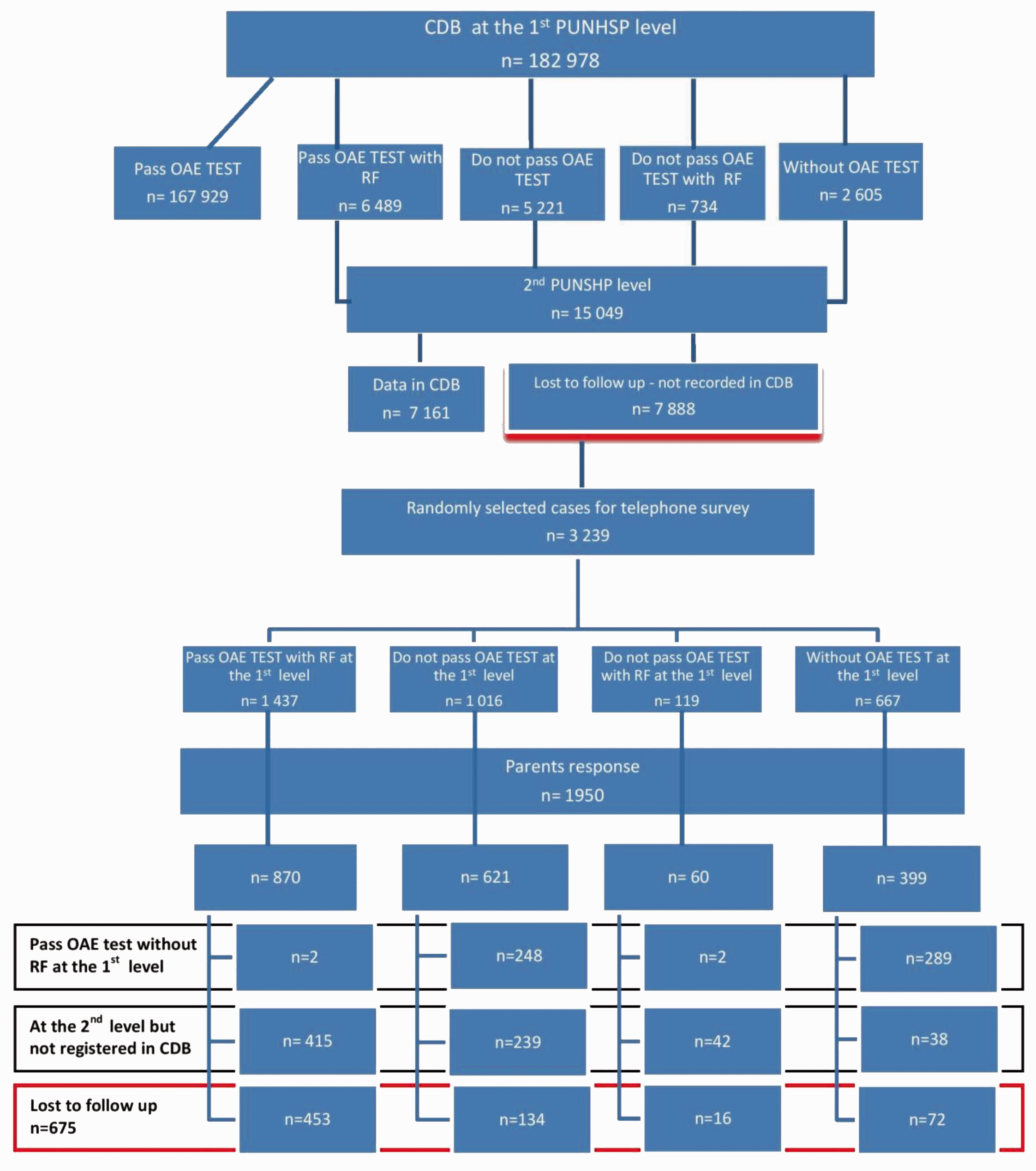
The questionnaire contained the following questions:
What was the result of the screening test? Possible answers: passed criteria of OAE test, did not pass criteria of OAE test, no screening test, do not remember. What was the colour of the certificate pasted into the book your child’s health? Possible answers: blue, yellow, none, do not remember. Did the child report risk factors for hearing loss? Possible answers: yes, no, I do not remember. Open question – If so, what? Did parents after leaving the hospital after delivery come to the further diagnostics to the 2nd PUNHSP level? Possible answers: yes, no, I do not remember. Open question – If not, why not?
Statistical analysis
Children were randomly selected proportionally to the group size, according to the result of the 1st PUNHSP level screening test. The statistical analysis was performed with a chi-square test for independence. Confidence intervals were used to estimate the percentage of actual follow-up visits at the 2nd PUNHSP level. The assumed confidence level was α = 0.05. All calculations were performed with Statistica 12 and MS Excel 2010 applications.
Results
From the 3239 parents selected for participation in the survey, 1950 (60.2%) answered the questions. No statistically significant differences were found for the percentage of parents selected for the questionnaire and those who answered it (p > 0.05). Hearing screening was performed in 94.4% (n = 1840) of children from the analysed group, and not performed in 5.6% (n = 110) of which 38 children were on the diagnostic level and 72 were not (Figure 1).
From information provided by parents, of children registered in the CDB as without a screening test (n = 399), 72.4% met the pass criteria for the OAE test (n = 289). Of children registered at the 1st PUNHSP level as those who failed to meet the pass criteria (n = 621), in 248 cases (39.9%) parents informed us that the final result at the 1st PUNHSP level was correct. Detailed analysis showed that only results of the first (not binding) screening test were entered in the CDB where a child failed to meet the OAE pass criteria, but the final results (correct OAE recording) of the screening test performed on the day of hospital discharge were not entered. The result of the survey study shows that 27.7% (n = 541) of children met the pass criteria for the OAE test during the hearing screening at the 1st PUNHSP level and no RF for hearing loss were noted, but those results were not registered in CDB. These nonconformities represent 0.2% of all entries made. The survey disclosed errors resulting from not entering data into the CDB. All children from this group received a blue certificate and were therefore excluded from further analyses. In the remaining group of 1409 children (72.3%), parents confirmed the result of the screening test recorded in the CDB at the 1st PUNHSP level. This group was used in further analyses (Figure 1).
In their responses to the questionnaire, 55.6% (n = 784) of parents answered that they had a yellow certificate, and 22.9% (n = 322) had a blue certificate. In this group, 73.9% of children met the OAE pass criteria with RF. There were 114 (8.1%) parents who did not receive a certificate, and 13.4% of parents did not remember the colour of the certificate they received.
Of 940 children with RF noted, 82.8% (n = 779) of parents confirmed their occurrence. Seven hundred and thirty-four (52.1%) children of those parents interviewed came for diagnostic tests, but this was not recorded in the CDB. Of parents who did not come with a child for further diagnostic tests (n = 675), 22.9% (n = 149) had a wrong certificate pasted in their child’s medical record book. In this group, 81.2% (n = 121) of children met the OAE pass criteria with RF for hearing loss. Lack of a certificate in a child’s medical record book was noted for 11.3% (n = 76) of interviewed parents. There was a statistically significant relationship between the certificate type and reporting to the 2nd PUNHSP level (χ2(2) = 32.245; p = 0.0000). Parents of children with a yellow certificate came to the 2nd PUNHSP level centres more frequently (60.06%) than parents of children with a blue certificate (53.07%) or without any certificate (26.4%).
The most common reasons for not coming to the 2nd PUNHSP level included the time taken between the 1st level test and the appointment at the diagnostic centre (36.09%), lack of referral to visit (25.9%), conscious parental decision not to come for a visit due to a lack of noticeable signs of hearing loss (16.35%), child’s illness at the time of the arranged visit (7.43%), no need for the visit as determined by a general practitioner (4.88%), parents forgetting about the visit (2.76%), lack of time in parents (1.27%), too large a distance to the 2nd PUNHSP level centre (0.63%) and child’s death (0.21%).
Discussion
Further analyses concerned only the answers from parents whose children required a visit at the 2nd PUNHSP level (n = 1409).1,3 This means that not 8.2% (n = 15,039) but only 5.9% of newborn infants required further diagnosis at the 2nd PUNHSP level (estimated 10,874); 27.7% of children who should have come to the 2nd PUNHSP level according to data in the CDB actually had a blue certificate, because they passed the second OAE test at the 1st PUNHSP level without RF for hearing loss. This group also included children whose personal details were entered into the CDB, but without information about results of the screening test at the 1st PUNHSP level.
When analysing reasons for non-attendance at the 2nd PUNHSP level according to the 1st level hearing screening result, most commonly, parents of children who did not undergo the hearing screening immediately after birth did not come for further diagnostics. In this group, only 70.4% of parents came for a diagnostic visit at the 2nd PUNHSP level. Parents of children who met the OAE pass criteria and with RF came for the 2nd PUNHSP level visit (85.9%) most frequently; 82.4% of parents of children who failed to meet the OAE pass criteria and without RF and 81.3% parents of children who failed to meet the OAE pass criteria and with RF came for further diagnostics. In countries such as the UK, where the hearing screening programme is a part of the National Health Service, and information about newborn infants and their complete medical history is collected automatically, 82.5% and 95.8% of parents come for diagnosis of hearing loss before the fourth week and by the sixth month of a child’s life, respectively. 4 In the United States, the CDC reported data on loss to follow-up, indicating that the main reasons for not coming for a follow-up visit included: parents’ refusal, relocation to another state, waiting for the visit or child’s death. This rate was 64.7% on average, and ranged from 2% to 97% depending on the state. 5
Previous statistical analysis of the percentage of follow-up visits at the 2nd PUNHSP level in Poland, based on data in the CDB, showed this to be 55.8%. 3 Based on the telephone survey, the data on the percentage of follow-up visits at the 2nd PUNHSP level in the CDB were significantly underestimated. The survey showed that the actual rate of follow-up visits at the 2nd PUNHSP level was 83.6% (95% CI 83.0%–84.2%). On this basis, it can be concluded that the actual number of children requiring consultation at the 2nd PUNHSP level in the studied period was 10,874, and not 15,039, as was recorded in the CDB. This result is comparable with the rate of follow-up visits at the diagnostic level in countries such as the UK (82.5%–95.8%), the Netherlands (92.3%), Germany (77.4%), the French-speaking part of Belgium (62.21%) or the United States (64.7%).5–8
These reports indicate that parents of children who did not undergo hearing screening immediately after birth were most common amongst loss to follow-up, followed by parents of children who met the OAE pass criteria but with RF noted. Two reports also indicated that factors such as an insufficient number of paediatric audiology specialists, distance to the place of living, no referral, insufficient monitoring by paediatricians and inadequate knowledge of parents, who are not always able to notice clinical signs of hearing loss, are the main reasons for not attending follow-up visits.9,10 Systems for reminding or notifying parents about the need to attend diagnostic level appointments, used in countries such as the United States, the UK, Germany, and the Netherlands,4,9–11 demonstrate that, by using uniform criteria and a patient monitoring system, it is possible to reduce the number of children with incomplete diagnosis within several years. In the United States, for example, the rate of children not completing diagnosis decreased from 44.8% to 35.4%.5,10,11
Conclusions
Our telephone survey disclosed omissions in registration of data in the CDB. When all collected information was considered, the actual percentage of children diagnosed at the 2nd PUNHSP level was 83.6%, a result comparable with those from countries with similar implemented programmes. After analysing the data received from the telephone survey, a recovery programme was implemented, to eliminate the problems relating to the registration data. The analysis shows that programmes and activities should be continuously monitored and adapted to new conditions. Over the years, a number of changes have been introduced to the PUNHSP, including an electronic version of the data registered by the centres, software changes and changes in protocols of data transfer. Each screening system requires continuous and detailed monitoring of all levels and components influencing quality of recorded data. 12 This analysis demonstrates that attention should now be focussed on developing a more controlled programme in respect of contact with parents of children requiring further diagnosis, and that certificates pasted in a child’s medical records book by family doctors should be monitored.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.